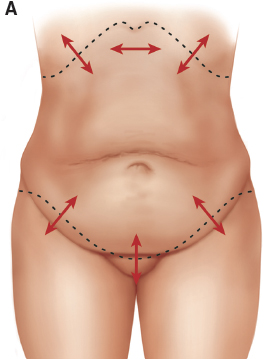
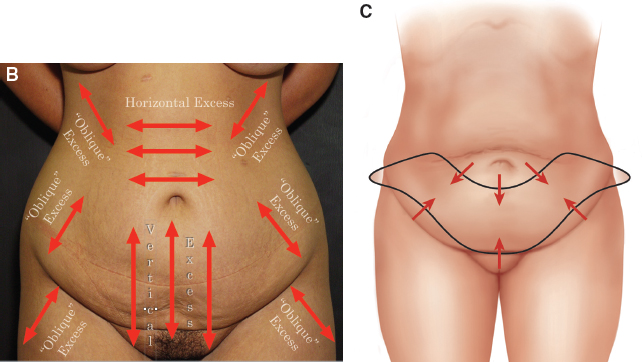
CHAPTER 7 The traditional primary goals of abdominoplasty have always been to excise the excess skin or pannus of the central lower abdomen and to plicate the abdominal fascia through a suprapubic incision. Unfortunately, the classic abdominoplasty often falls short of this goal and results in a high-riding scar, or leaves remaining skin and lipodystrophy at the pubis, thighs, flanks, and hips, and there is a persistent incidence of midline skin necrosis or wound dehiscence. The HTA addresses these shortfalls. This procedure may be defined as a more complete treatment of the trunk aesthetic unit from the abdomen to the pubis, hips, and thighs, with a greater aesthetic result and a margin of vascular safety. This chapter outlines the techniques and tools needed to obtain these superior results safely and consistently. The abdominoplasty technique has evolved significantly over the past 40 years. The modern technique was developed in South America during the 1960s. The basic surgical tenets have always been to conduct a rectus plication that involves maximal excision of the central skin excess through extensive undermining of the entire abdominal wall. The closure is often performed under some tension, so it is conducted with the patient in significant flexion. When liposuction was introduced during the 1980s, it soon became apparent that its exuberant application during an abdominoplasty was fraught with an unacceptable incidence of flap ischemia and skin necrosis. Liposuction then evolved into a more conservative adjuvant treatment. Although there were indeed fewer physiologic problems with this technique, the aesthetic results were also, once again, more constrained. Then, during the early 1990s, Lockwood published a series of seminal articles that single-handedly changed the tack of the abdominoplasty. With his extensive experience with body contouring surgery, he decisively demonstrated and definitively modified the surgical principles of abdominoplasty and reported greater safety and improved aesthetics. He enumerated several surgical tenets that were in many ways diametrically opposed to those of the classic or traditional abdominoplasty. These included the undermining of only the central skin flap to facilitate plication, with discontinuous dissection elsewhere (to enhance vascularity and allow judicious concomitant liposuction), as well as the initial resection of the lateral excess skin, with more conservative resection of the central skin flap (to accomplish a more complete and natural repair) by using a planned and controlled high-tension closure with the diligent use of the underlying superficial fascial system (SFS). Thus the HLTA was born. Since 2000 I have become a diligent student of these Lockwood principles, and I have applied them to several hundred patients. The application of these principles and the critical analysis of their results have driven the successful evolution of the original HLTA procedure. For a patient’s results to be considered truly successful, strict self-imposed standards were applied: the procedure had to demonstrate the greatest degree of safety (zero tolerance for complications) and the maximal aesthetic result (correction of all deformities), with consistent reliability of the technique (regardless of patient presentation). Several important expanded principles can be distilled from this experience to define a true 2.0 advancement in technique. Surgeons performing the abdominal procedure should not adhere slavishly to the age-old mandate that all of the excess skin between the pubis and the umbilicus be excised. This approach only truly works for a patient with an enormous pannus. For all other cases, the excisional marking has traditionally been placed above the pubic hairline to accomplish wound closure. Despite the harnessing of excess pubis, the closure often remains overly tight. This results in an excessively high scar, a superiorly retracted pubis, an unnaturally flat hypogastrium, and, more seriously, an increased opportunity for wound dehiscence and skin necrosis. The redundant pubis should instead be excised rather than harnessed to ensure an inconspicuous wound closure. With the exception of the most redundant cases, this approach often involves deliberately leaving some of the skin between the pubis and the umbilicus intact, thereby necessitating closure of the original umbilical site. The surgeon must resist the temptation to remove even these few centimeters of intervening central abdominal skin for fear of re-creating the usual overly tight closure. Any surgeon performing abdominoplasty should consider not only what is above the future incision (the traditional pannus) but also what is below it: excess pubis, anterolateral and medial thigh redundancy, and buttocks laxity. If these areas are not addressed, the tissues below the incision may be distractingly untreated, and thus the full effect of HTA will not be realized. This tenet underlines one of the greatest benefits of HTA, which is not usually considered possible with traditional abdominoplasty: one can affect a true body lift through an anterior incision. This approach describes what is actually more of a global tension abdominoplasty, with maximal sequential tension placed from laterally to medially (hence the evolution of HLTA [with emphasis on the lateral] to, more simply, HTA). It has always been important to evaluate the magnitude of the excess skin to be excised. However, to actually design the most efficient length and cant of the incision, the extent and orientation of the skin to be left behind should also be assessed. The surgeon can at once ensure that the remaining skin is sufficient to close the defect and is efficiently relieved of its own redundancy. This principle should be applied to both the central and lateral closures. More specifically, laterally, the excess skin at the hip and thigh is often neglected by traditional abdominoplasty. This primarily obliquely oriented excess tissue is most efficiently removed through the oblique incision and vector of the HTA. Centrally, the superfluous skin at the epigastrium (supraumbilical area) actually constitutes primarily horizontal excess. This excess skin can neither be efficiently removed nor used to close a lower abdominal defect through the horizontal incision. Therein lie the essential flaws of the traditional abdominoplasty and the compelling efficacies of the high-tension technique: conflicting and unintended consequences may occur with the former and be mitigated with the latter. The central epigastric excess is not treated effectively, and the suprapubic wound closure is too tight, despite this epigastric redundancy. Laterally, the excess cannot be effectively treated, because the remaining abdominal flap has been recruited primarily to close the wound centrally. To reconcile this paradox, less skin should be excised centrally and more skin excised laterally through an HTA-oriented incision and repair. The more the procedure follows the vectors of excess of both what is taken and what will remain, the more efficient the treatment of redundant skin will be. By applying this vector of excess principle, the necessary direction of the most desirable HTA central and lateral incision placement is easily understood and defined. Fig. 7-1, B and C With the use of this vector analysis, the tissue above and below the planned incision is then appreciated to be redundant in a more oblique vector and so should be removed through an opposing oblique incision. Serendipitously, this same vector matches the relative direction of the desired HTA lateral scar placement. And at the same time, this oblique vector more efficiently treats the predominantly horizontal excess in the epigastrium. However, centrally in the suprapubic region, the excess is truly vertically oriented, so a fully horizontal incision remains most efficacious. When applying this vector of excess principle, the necessary direction of the most desirable HTA central and lateral incision placement is easily understood and defined. Thus, the more a procedure follows the vectors of excess of both what is taken and what will remain, the more efficient the treatment of redundant skin will be. These principles will be clearly illustrated in the Physical Examination section later in this chapter. There is a corollary of the vector of excess principle: The extent of the incision should follow the extent of the skin excess, permitting the application of the high-tension approach and a more dramatic result. In fact, as will be discussed later in this chapter, a virtual lower body lift can be accomplished with the patient in an entirely supine position. Although the most posterior aspects of the buttocks and thighs cannot be fully addressed, this technique can and does gratify the majority of patients. And, most importantly, this more conservative body lift reduces the surgical time and the operative risks as compared with a full truncal lift procedure. Lockwood—originally and rightfully so—emphasized the lateral tension nature of this technique. Contrary to the traditional approach, he stated that one must begin the resection laterally rather than medially. This admonition emanated from his original observation that there was actually more redundancy laterally at the hip, thigh, and buttock as compared with centrally. Indeed, if the surgeon respects and executes this principle, he or she will realize a superior correction (hence Lockwood’s “lateral tension” eponym). However, as previously explained, it is more instructive and in fact more efficacious to consider the entire length of the wound to be available for a tension repair. If this tension principle is honored, it is possible to realize maximal correction centrally as well as in the pubic area and the inner and anterior thigh regions. The goals of the design and placement of the future abdominoplasty wound are to harness its access and hide its scar. Lockwood originally described a very high (French-cut) lateral closure, probably because of the style of clothing that was more fashionable at the time and also because a more oblique vector of pull does indeed efficiently treat the upper abdominal excess, as described previously. However, because fashion changes and a hidden scar will always trump some residual excess skin, it is a basic tenet of this HTA 2.0 technique to deliberately mark patients within the outlines of their preferred style of clothing. This philosophy becomes particularly relevant when contending with a low-cut jeans fashion so as to prevent displacement of the lateral scar too far superiorly. The location and extent of the remaining subcutaneous fat must also be evaluated. This assessment represents an age-old plastic surgical battle between beauty and blood. In other words, at what cost to the blood supply does the surgeon attempt to remove all remaining excess subcutaneous fat? Lockwood originally described a reasonable treatment détente: Liposuction could be conducted beneath any tissues that have not been undermined. More recently, the proverbial pendulum has swung backward, with certain publications once again giving surgeons permission to conduct more aggressive full truncal liposuction at the time of the abdominoplasty. This recommendation is predicated on Lockwood’s admonition that the restrained abdominal flap dissection preserves enough perforators to allow central liposuction. However, one fact must be persistently respected: the abdominal flap remains a random flap. In addition, some of these same precious perforators must already be sacrificed with the repair of the more protuberant abdomen. Lockwood’s past principles, built on a prodigious amount of experience, embody these very facts. Today’s surgeon should perhaps still pause and consider second-stage liposuction of the flap as a safer alternative. Thus, in an abdominoplasty patient with the more common higher BMI of 26 or more, liposuction should be restricted to the waist and hip rolls, with a secondary central liposuction planned for some 6 to 12 months after the initial procedure; only at that time can zero tolerance for skin-flap necrosis and dehiscence be honored. A general survey of the abdominal wall’s anatomy has already been described in great detail in Chapter 1. For greater efficacy, the specific anatomy most relevant to the understanding, planning, and application of the HTA involves three critical anatomic points that should be understood and respected: 1. The SFS: Scarpa fascia was described more than 200 years ago, but it was Lockwood who rediscovered this powerful anatomic layer. Lockwood’s vision of maximally lifting the body’s skin envelope with the use of tension mandated a more secure closure, and this resulted in his revelation that this fascial layer had tensile properties far beyond the local wound. The Scarpa layer was anything but passive and could instead act more like a finger trap that tightened reliably as the wound tension increased. Thus the SFS layer must be harnessed to at once realize the maximal lift that this technique can proffer and prevent wound dehiscence. 2. The perforator blood supply: It is a poorly respected fact that, when the abdominal skin is undermined, it becomes a random flap and therefore must be protected just as judiciously to avoid flap ischemia. Once again, Lockwood was the first to emphasize the importance of sacrificing only those perforators within the boundaries of the prospective fascial plication during flap elevation. Although the remaining flap has not been fully undermined, the application of discontinuous dissection still ensures its efficient mobilization and preservation of its perforators. 3. The zones of adherence: Lockwood emphasized the existence of various points of skin attachment. Practically speaking, the skin must simply be released, at least bluntly, wherever adhered if one is to realize the maximum translation of the pull of the remaining skin envelope. This is particularly true in the region of the anterolateral hip and thigh. The one exception to this rule is the supraumbilical constricted waistband of adherence, which I originally described. This impressively immobile zone is most often identified in heavier patients and in those who have experienced significant weight loss. Although it can indeed inhibit the mobility of the upper abdominal flap, this inordinately tight band should be left intact. Even with significant undermining, the overhanging excess skin cannot be treated effectively, and the ischemia risk will remain predictable. This situation is further discussed later in this chapter. Anatomic Danger Zones ■ The SFS: This layer must be maximally used to accomplish a proper tension lift, and it must be fully harnessed to prevent wound dehiscence. ■ The costal perforators: The remaining skin flap of an abdominoplasty should properly be considered a random flap, and the superior and lateral costal perforators are its sole nourishment and insurance against skin necrosis. Efforts to preserve these vessels include conservative skin-flap elevation (which occurs in combination with discontinuous dissection) without direct liposuction. ■ The supraumbilical band of adhesion: This scarlike crease and its overhanging skin excess are best left not elevated. Only a nominal degree of additional skin will be realized at the expense of a significantly higher chance of skin necrosis. ■ The lateral femoral cutaneous nerve is quite vulnerable to inadvertent injury. This structure is best protected by mindfully preserving a layer of tissue over the iliac when dissecting the flap. The most effective way to define the best use of the HTA is to discuss the characteristics of the ideal patient. In so doing, there is a necessary correlative principle: Rather than trying to fit an abdominoplasty technique to every patient, the surgeon must concede that some patients are simply not good surgical candidates. The indices that should guide the surgeon when determining abdominoplasty candidacy include the following: ■ Omental fat: A patient with voluminous omental fat and attendant prodigious abdominal wall protrusion will resist effective fascial plication. ■ Subcutaneous fat: A patient with significant excess subcutaneous fat will tempt aggressive liposuction and possible skin necrosis. Excessive fat also acts like a glue that immobilizes the skin, resisting the adequate translation of pull and therefore its removal. ■ Skin: A patient with excessively deflated skin often responds after contouring with an annoyingly inevitable recurrence of relaxation that I call the “double stretch.” This potential deformity mandates effective and thorough preoperative counseling. The patient criteria to be considered must be exhaustive and respected if the surgeon is to avoid major complications and patient disappointment. The ideal patient criteria include the following: ■ Weight: The patient should not be grossly overweight (BMI less than 30). His or her weight should be stable for more than 6 months if a significant amount of weight has recently been lost. ■ Medical condition: No major medical issues should be present, such as labile hypertension, diabetes, coronary disease, and nutritional deficiency (check albumin and protein levels). ■ Psychological state: The patient should be well motivated to complete his or her postsurgical care and realistic about the results of the procedure. ■ Habits/lifestyle: Patients should preferably perform regular exercise, eat a reasonable diet, and not smoke or consume excessive amounts of alcohol. ■ Anatomy: The patient should have an absence of multiple abdominal scars, no extreme abdominal protrusion, a moderate subcutaneous fat layer, and easily mobile and translatable redundant skin. A comprehensive examination is essential to enable the surgeon to properly prepare the patient and accurately plan the surgery. The physical examination should include evaluation of all layers of the abdominal wall: skin, subcutaneous fat, and the underlying fascia and muscle, with an indirect assessment of the extent of intraabdominal fat. The skin examination should involve much more than just assessment of the classic pannus of excess lower abdominal skin above the pubis. Striae The boundaries and extent of any striae that may not be included in the resection should be duly noted and explained to the patient, particularly if they affect the area above the umbilicus. Fig. 7-2 Adhesions Note should be made of any adhesions of the skin in the thighs and the abdomen proper. An adhesion can also be found at the level of the waist, particularly laterally; this is the waistline zone of adherence and contraction. There is most often what one may call a “secondary roll” of excess skin that rests above this valley, most notably in the larger patient or in the patient who has lost a significant amount of weight. This band essentially divides the abdominal excess skin into superior and inferior segments. The surgeon must be aware that this adhesion will resist efforts to efface the upper abdominal excess of skin. Because this zone harbors vital perforators, only a judicious release of the area with the use of discontinuous undermining should be attempted. Otherwise, the upper abdominal redundancy is best addressed with either a fleur-de-lis type of abdominoplasty or a second-stage reverse abdominoplasty. Excess Skin The extent of obvious anterior redundant skin (the width of the pannus) is noted first. This evaluation most accurately defines the potential length of the incision. However, a proper assessment must extend beyond this obvious excess if a more complete correction of the entire anterior trunk aesthetic unit is to be made. In other words, the extent of redundancy should also be evaluated in a few areas: below the pannus; at the hips, thighs, and pubis; and above the pannus at the upper abdominal and epigastric area. The mobility or translation of the skin is also very telling: the looser the skin, the better the potential result. Fig. 7-3 Examination must be made of the redundancy of the skin at the upper abdomen, which can be more “stealthy” in its presentation, being evident only when the patient is asked to sit, bend over, or lie flat and the skin is “gathered.” As previously explained, in the case of the horizontal “secondary roll” (Fig. 7-2), it is the waistline zone of adhesion that resists its full excision from below and thus would actually require a reverse-type abdominoplasty repair. In addition, for the more horizontal excess redundancy that may be seen at the upper, primarily midline zone, a fleur-de-lis type of approach would be necessary for full correction. Clearly, these more aggressive surgeries are primarily indicated in the massive-weight-loss patient, but the fact that this excess skin can be found in the routine patient underlies the necessity to duly inform patients that this same excess may not be fully removed through the traditional lower abdominoplasty approach. Scars All scars of the abdomen are assessed. Of greatest concern are scars in the subcostal and midline areas; these require the surgeon to map out the safest and most effective surgical approach. For a subcostal scar, it is best to restrict undermining and, if possible, to convert the HTA into a fleur-de-lis type of procedure so that the scar is included within the pattern. The midline scar presents a similar challenge, and either a fleur-de-lis type of procedure or a reverse abdominoplasty pattern should again be considered. The subcutaneous layer must be carefully assessed and a “topographic” map of the underlying fat must be visualized. A “topographic” sense of the extent of underlying fat must be achieved. This mapping of the subcutaneous layer can serve as a guide for future markings to show where liposuction should be performed and, just as importantly, where it should not be performed. Usually the contouring will focus on the waist, hips, and lateral thighs. This liposuction enhances the HTA by both facilitating the translation of the pull of the skin with its liposuction-induced discontinuous dissection as well as accentuating the abdominoplasty’s shaping effects. If the central flap is particularly thick with fat, then it is best to inform the patient that a second-stage liposuction surgery may be necessary to complete the repair safely.
High-Tension Abdominoplasty
Evolution of the Modern Abdominoplasty
HIGH-TENSION ABDOMINOPLASTY VERSION 2.0
Excess Skin Above the Incision
Excess Skin Below the Incision
Excess Skin Left Behind
Length of the Incision
Tension of the Incision
Placement of the Incision
Treatment of the Remaining Subcutaneous Fat
Surgical Anatomy
Indications and Contraindications
PATIENT SELECTION
Patient Evaluation
PHYSICAL EXAMINATION
Skin


Subcutaneous Fat
Abdominal Wall
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine