44 High-Density Transplants
Summary
Keywords: dense packing high density recipient sites graft survival safe density single session
Key Points
•High-density transplants can produce dense and natural results in one session.
•Patient and site selection are important when using this technique.
•The main advantage of this technique is outstanding patient satisfaction.
44.1 Introduction
The density of recipient site incisions has changed markedly over the years since hair transplants were first performed. Initially, the recipient site was of relatively low density because of the large size of the grafts. Each large punch graft required a large recipient site. Each recipient site had a large surface area and volume, and created a significant amount of vascular trauma. However, with the use of smaller grafts, recipient sites became smaller and thus created less vascular trauma per site, enabling more sites per square centimeter.
The use of high-density recipient sites is also known as dense packing. There is no established definition as to what constitutes dense packing or high density, but it can be generally described as a density over 30 grafts/cm2.1,2 Graft densities of ≥40 to 50 grafts/cm2 are done routinely by many surgeons under select conditions. Hair transplants performed to this standard can achieve outstanding results in one session (Fig. 44.1 and Video 44.1).
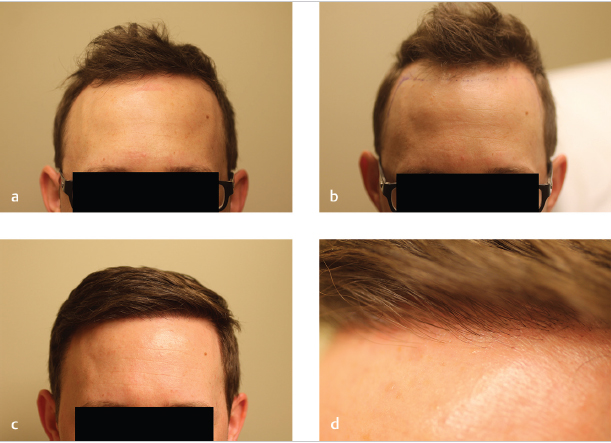
Fig. 44.1 (a) Preoperative photo prior to lowering of the hairline. (b) Preoperative marking of the recipient area. (c) Patient results after one high-density transplant of 1,933 grafts to lower the frontal hairline. (d) Close-up of the hairline after one transplant.
44.2 Are High-Density Transplants Safe?
As with most new techniques, early detractors of dense packing questioned the safety of this approach.3 Safe density can be considered in two distinct ways. The first is a determination of the highest achievable density that avoids tissue necrosis. The second is a determination of the highest achievable density that avoids a significant decrease in graft survival. In other words, a safe density is the highest density that can be achieved without compromising the safety of the recipient tissue (i.e., the scalp) and the donor tissue (i.e., the grafts).
The most worrisome concern with higher density is the possibility of tissue necrosis from vascular trauma. One of the initial theoretical concerns was that the large number of incisions created a huge cumulative amount of linear trauma. For example, if a 1 cm2 area was transplanted at a density of 55 grafts/cm2 using a 1-mm-wide flat blade, this would create a cumulative length of incision of 55 mm from the incisions, which sounds like a lot considering it is occurring in a 1 cm2 area. However, it is important to consider that each incision has a height (i.e., thickness) and a depth, with the thickness being only 0.1 to 0.2 mm (depending on the blade being used). In other words, it is better to discuss incision trauma in three dimensions rather than in only one dimension. With this in mind, it would take approximately seven times as many 1-mm flat blade incisions as 1-mm punch incisions to produce an equal volume of trauma. Moreover, the most important factor in terms of vascular trauma is the depth of the incision and this must be carefully controlled in cases of dense packing. In the cases where the depth of each incision is longer than 5 mm, it is prudent to avoid dense packing too tightly (e.g., no higher than 45 grafts/cm2) to avoid the possibility of tissue necrosis. In most cases, however, incision depth can be kept below 5 mm. The author has been performing high-density transplants for over 10 years and has never had a case of tissue necrosis. Tissue necrosis is an exceedingly rare complication of dense packing if done correctly.
In one series of reports, surgeons were able to transplant 45 and 64 grafts/cm2 with good survival rates of up to 107 and 96%, respectively.4,5 One of the surgeons then demonstrated survival rates of 92 to 96% in patients transplanted at densities of 100 follicular units/cm2.5 One of the limitations was that the test areas were isolated with no hairs grafted around them. As a result, it was unclear if this result could be replicated over large areas.
Another study demonstrated that grafts can be safely transplanted at densities of 72 grafts/cm2.6 In this study, test areas were carefully delineated with tattoos and the areas surrounding the test areas were transplanted at densities of 30 to 40 grafts/cm2 to see if this would affect graft survival. In the most densely packed area of 72 grafts/cm2, there was 98.6% survival, providing evidence that it is possible to achieve good growth with high-density transplants.
44.3 Techniques and Procedures
In the author’s practice, the donor hair is first harvested using either the strip method or follicular unit extraction (FUE). The techniques involved in the harvesting of the donor hair are discussed extensively in other chapters in this text.
In theory, many techniques can be used to create high-density recipient sites, ranging from needles to chisel blades, from stick and place to premade incisions, and from sagittal to coronal (lateral slit) incisions. One difficulty with using the stick-and-place technique for high-density transplants is the generation of lateral pressure on the surrounding tissue every time a recipient site is created. The incising device has the potential to add lateral pressure to the surrounding tissue, increasing the possibility of popping. Despite this potential difficulty, high-density transplants can be successfully accomplished using this method.2
Coronal and sagittal slits can both be used to create high-density recipient sites; however, higher densities with sagittal slits can be more difficult to achieve unless smaller blade sizes are used because the incision length of a sagittal slit is always longer than the blade width unless the blade is inserted perpendicular to the skin. For example, a 1-mm blade will yield a 1.4-mm sagittal incision on the skin surface if inserted at a 45-degree angle, and will yield a 2.0-mm incision if inserted at a 30-degree angle. The flatter the angle, the longer the incision size. Conversely, a 1-mm blade will always yield a 1-mm coronal incision on the skin surface.
The use of coronal slits was pioneered by Dr. Jerry Wong and offers several other advantages, including the following: (1) encouraging the hairs in the graft to line up coronally, which maximizes the shingling effect, (2) precisely controlling the angulation of the hairs as they exit the scalp, and (3) decreasing popping.7
The author’s preference is to create premade slits using tiny chisel blades in a coronal orientation (Fig. 44.2and Fig. 44.3). In a typical transplant where the frontal half of the scalp or hairline is transplanted, the author first creates the two-hair recipient sites at the frontal hairline from temple to temple in a zone approximately 2 to 4 cm in width at a density of approximately 50 to 55 grafts/cm2 followed by the creation of one-hair recipient sites anterior to the two-hair grafts. Moving posteriorly, the remaining two-hair recipient sites are made at densities of about 45 grafts/cm2 and the three-hair recipient sites are made at about 35 grafts/cm2. Blade sizes used to create the recipient sites depend upon several factors, including the size of the follicular units, the fragility of the follicular units, and the firmness of the recipient area tissue. In most cases, the author will use 0.65- to 0.75-mm blades for one-hair grafts, 0.75- to 0.95-mm blades for two-hair grafts, and 0.95- to 1.15-mm blades for three or four-hair grafts. If sagittal slits are used, smaller blades are required.
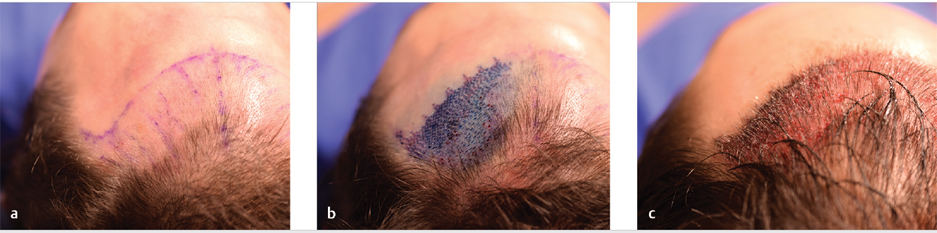
Fig. 44.2 (a) Photograph of the recipient area prior to the creation of the recipient sites. (b) Recipient site incisions stained with methylene blue. (c) Recipient area after insertion of the grafts.
Related posts:
 Methods and Techniques to Study Hair Cell Survival
Methods and Techniques to Study Hair Cell Survival
 Hair Transplantation: The Promise of Cell Therapy
Hair Transplantation: The Promise of Cell Therapy
 The Patient with Minimal Hair Loss: Planning and Decision-Making
The Patient with Minimal Hair Loss: Planning and Decision-Making
 The Young Patient: Planning and Decision-Making
The Young Patient: Planning and Decision-Making
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 East,West, and Southern Asian Hair Transplant Specifics
East,West, and Southern Asian Hair Transplant Specifics
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


