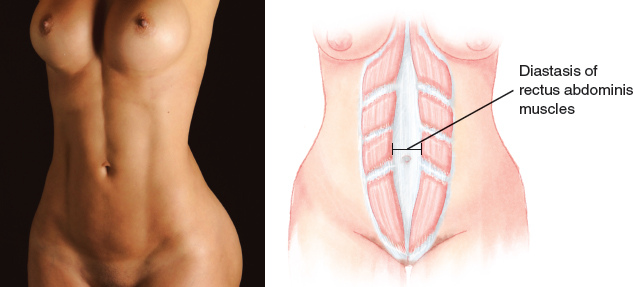
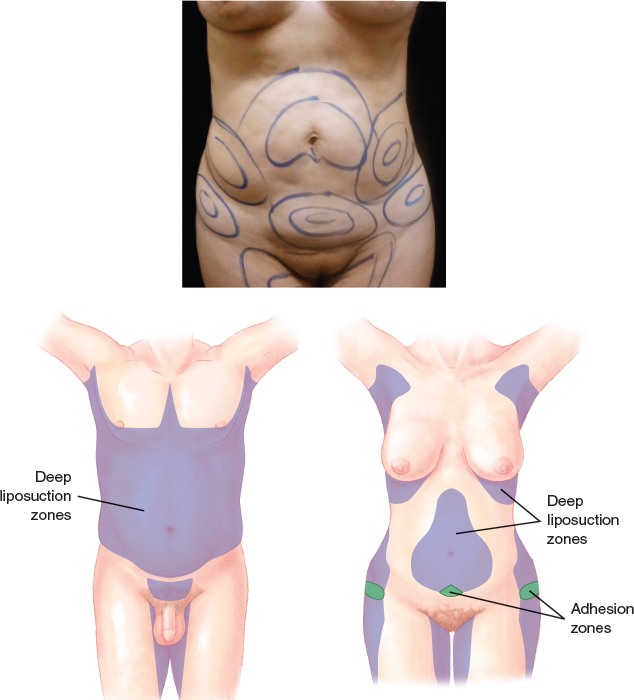
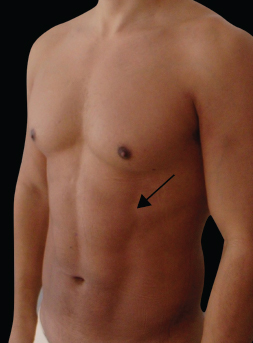
CHAPTER 20 Alfredo E. Hoyos The pinnacle of fitness is a toned and defined abdomen; this is evidenced by a “six pack” in men and a “two pack” in women. All athletic individuals want this look, and many athletic men and women have the strong will to go to the gym every day to try to get it. However, few can truly achieve it. Those who do obtain it have the appropriate genetics to store the fat in the right places so that it does not obscure the abdominal muscles, and they also put in a lot of work at the gym. For others, the desired muscle definition is elusive, no matter how much they work out. Fig. 20-1 The ideal body biotype for men has remained almost exactly the same across time. Sculptures and paintings from different epochs and cultures have displayed the ideal male body, and this ideal remained nearly identical from the art of ancient Greece and Rome, to the works of the Renaissance masters, to contemporary artistic movements. The ideal athletic man has always been shown to have a very well-defined and muscular figure. ■ During the late 1940s and 1950s, with a return to a wealthier lifestyle after World War II, the curvy hourglass shape was the ideal for women. More importance was given to breast size, and little attention was paid to the waist. Marilyn Monroe exemplifies the iconic form that was preferred during this period. ■ During the 1960s, everything changed. The women’s liberation movement took hold, and women started to take part in the social and political activities of America. The miniskirt was the official trend, and the curvy woman was no longer the ideal. The popularity of a model nicknamed “Twiggy” led to a desire for women to have thinner bodies and long legs and to wear chic, revealing outfits. ■ The 1970s were a time of reaction against the established patterns in the social and political realms, and aesthetic preferences were affected as well. The “hippie” trends led to a relaxation of lifestyle, apparel, and even undergarments; the informal look was the rule. ■ The 1980s saw the birth of the supermodel. A sexy, curvy, pretty woman could be rich, famous, and successful just because of the way she looked. Women everywhere considered this the ideal and did their best to achieve it. ■ The look portrayed by celebrities and models during the 1990s was known as “junkie chic,” with a trend toward waiflike, even gaunt contours. The prevailing idea was “the thinner the better,” and this became so pervasive that women’s health was a serious concern as an epidemic of anorexia occurred. ■ Paradoxically, in the last decade of the century, adult men and women began gaining weight at an alarming rate, leading to a higher incidence of obesity and its attendant morbidities. ■ The twenty-first century began with the consequences of the trends of the 1990s, which led to a change in the public’s perception of the ideal and a move toward healthier-looking bodies. The main focus today for a woman is what she wants for her own body. This can only be addressed by considering each woman’s distinctive characteristics, including her geographic location, her age, her chosen fashion trends, and her ethnicity. For example, Asian women tend to prefer rounded faces and want very slim bodies, whereas Western women prefer a defined, bony, and squared face and a slender but more robust shape. Younger women tend to strive for an athletic body type, whereas women who have given birth tend to prefer a subtly curvaceous, toned look. For men there has been a growing body consciousness, with the media portraying sleek, lean, toned men at every age, leading many to feel insecure about their physique. This has proved a boon to manufacturers of fitness equipment and purveyors of diet programs as Americans struggle to overcome the results of their sedentary lifestyles, but diet and exercise may not achieve the desired aesthetic appearance in some individuals. The first attempts to remodel the human body involved altering the fat layers to remove tissue and to make the external contour flat. However, the human anatomy involves a complex mixture of concave and convex shapes, and the outcomes of these procedures left much to be desired. Shaping the contour by selectively extracting fat from some places and grafting it onto others achieves the best possible results and the desired look of an athletic body. This approach allows the surgeon to analyze the individual needs of each patient and to offer a tailored option for each body biotype. Liposuction has traditionally been dedicated to flattening an area by removing unwanted fat. However, the desired outcomes are far more complex and cannot be simply “flat.” High-definition liposculpture involves the removal of the fat from between the muscles and produces the desired result. After a high-definition liposuction procedure, many patients convert to a healthy lifestyle and use exercise and a healthy diet to preserve their results. This cycle of positive feedback improves results and long-term outcomes. Much of the abdominal contour is the result of the appearance of the rectus abdominis muscle. This is a vertically oriented paired strap muscle that runs along the central part of the anterior abdominal wall. The rectus abdominis arises from the symphysis, the crest, and the pectineal line of the pubis, and it then goes upward to insert into the xiphoid process and the costal cartilages of the fifth, sixth, and seventh ribs. The inferior portion of the muscle is covered only on its anterior surface by the rectus sheath; above the costal margin, the muscle lies directly on the costal cartilages. Fig. 20-3 The surface anatomy can be easily palpated in slim patients. Muscular intersections divide the abdomen into segments and create individual muscular bellies that are commonly referred as the “six pack.” The lateral border of the muscle is visible as a vertical groove in the anterior abdominal wall between the ninth costal cartilage and the pubic tubercle (arrow). This line, which is known as the linea semilunaris, typically runs along a line drawn from the midpoint of the clavicle to the middle of the thigh. The midline, which is also called the linea alba, is a site of frequent anatomic disruption. The diastasis or separation of the rectus abdominis muscles widens the linea alba. This can occur as a congenital deformity, after a pregnancy, or in response to intraabdominal obesity, and it may result in an abnormally convex abdomen. The thoracic arch forms an angle of about 90 degrees in men and 60 degrees in women. In men, a more rounded arch is created by the costal margin laterally and the highest tendinous intersection of rectus abdominis medially. The umbilicus lies within a defect in the linea alba opposite the fourth lumbar vertebra. In athletic men, a sharp rim is usually present at the upper border of the umbilicus, whereas the lower border is less well defined. In women, a periumbilical fat pad deepens the navel and obscures its borders. Anatomic Danger Zones ■ The adequate localization of the linea semilunaris is of paramount importance. When there is uncertainty about the location of this landmark, it is better to create an incision that is more lateral than planned. The surgeon can always go back and redo this line. However, if the incision is too medial, the correction will be more difficult. ■ The best possible contour appears when the real anatomy is followed, no matter how awkward it may seem. The failure to detect and contour the spaces between the muscles will affect the patient’s outcome. When the patient starts to exercise and follow a healthy diet, he or she will observe double lines and recognize the poor result. ■ Liposuction should never be performed from the lower incision into the costal margins; these areas should be approached from inframammary sites in women and sites beneath the nipple in men. Working with the suction cannula against the costal margin may lead to penetration of the abdominal wall. Patients with significant cardiovascular disease, hematologic or metabolic disorders, or thromboembolic disease are not good candidates for high-definition liposuction. Patients who have achieved massive weight loss and in whom severe laxity and stretch marks are present are also not ideal candidates. Hernias, myofascial laxity, defects of the abdominal wall, and indented scars may also be risk factors for this procedure. It is essential to understand and discuss the patient’s expectations regarding the procedure and to talk about the importance of physical activity and a healthy diet to improve and maintain the postoperative outcome. The surgeon must emphasize that this is not a weight-loss procedure. During the physical examination, the surgeon must evaluate muscle strength, the thickness of the fat layer, and the correlation of extraabdominal fat to intraabdominal fat. Myofascial laxity, hernias, indented scars, and rectus diastases must also be assessed. The individual’s body biotype is the main factor to consider when choosing the type of abdominal high-definition liposuction procedure to use, but the desired outcome is always an athletic body type. In an overweight patient, the main focus of the surgery is to remove as much fat as possible. If the patient is already slim or athletic, the amount of fat removed will be slight, and the purpose will be to reshape rather than to debulk the patient. In slimmer patients, fat may be transferred to the muscles to increase their definition. General anesthesia is preferred for these procedures. The potential loss of body temperature is avoided with the use of warm intravenous and infiltration solutions as well as heating blankets. Thromboembolism prophylaxis must include the use of low-molecular-weight heparin, intravenous corticosteroids, and compression devices on the legs. Correct abdominal marking is an essential part of the technique. Markings are created in three layers, and all markings should be made with the patient in a standing position. The use of markers of different colors is advisable.
High-Definition Liposculpture of the Abdomen
 David E. Guarin
David E. Guarin

Surgical Anatomy
Indications and Contraindications
Patient Evaluation
Preoperative Planning and Preparation
Surgical Technique
ANESTHESIA
MARKINGS
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine