Hernia Repair With Open Component Separation
Ibrahim Khansa
Jeffrey E. Janis
DEFINITION
Traditional component separation, now termed “anterior component separation,” involves separating the external oblique muscle from the remaining components of the abdominal wall.
This requires two steps:
Incision of the external oblique aponeurosis
Delamination of the external oblique muscle from the underlying internal oblique muscle
A third step (optional) is entry into and development of the retrorectus space.
“Posterior component separation,” also known as a transversus abdominis release (TAR), is another type of component separation. It requires two steps:
Entering and developing the retrorectus space
Transection of the posterior lamella of the internal oblique and transversus abdominis
Delamination of the transversus abdominis and transversalis fascia
ANATOMY
The layers of the lateral abdominal wall, from superficial to deep, are the external oblique, internal oblique, and transversus abdominis muscles, transversalis fascia, and peritoneum.
The segmental intercostal nerves to the abdominal wall musculature travel in the layer between the internal oblique and transversus abdominis muscles.
Vascular perforators to the abdominal wall skin emerge from the deep epigastric vessels.
They are arranged into a medial and a lateral row.
The medial row is dominant, especially the periumbilical perforators.
PATIENT HISTORY AND PHYSICAL FINDINGS
Assess if any indications for urgent surgery are present.
Bowel obstruction
Incarceration/strangulation
Infected mesh
Assess effect of hernia on the patient.
Ability to carry out activities of daily living
Pain at hernia site
Difficulty with defecation
On physical examination, look for:
Peritoneal signs
Reducibility of hernia
Edges of fascial defect
All scars on the abdomen (which will affect vascularity)
Presence of skin graft
Presence of a fistula
Presence of an ostomy
IMAGING
CT scan of the abdomen is useful to delineate:
The size, extent, and borders of the fascial defect
Whether component separation has been performed previously
The integrity of the musculofascial components (may have been previously resected)
An estimate of the loss of domain
Presence and position of prior mesh, if applicable
The thickness of soft tissue between the hernia (sac) and overlying skin
SURGICAL MANAGEMENT
Preoperative Planning
Assess suitability of the patient for major surgery.
Smokers and tobacco users should completely abstain for at least 4 weeks preoperatively and 4 weeks postoperatively.1,2
Nutrition should be optimized before surgery (prealbumin greater than 15 mg/dL, albumin greater than 3.25 g/dL).2,3
Diabetes should be well controlled (HbA1c ≤7.4%).2
Body mass index should be 42 or less, and preferably less than 40.2
After hernia dissection and lysis of adhesions, assess whether component separation is needed:
Apply Kocher clamps on the medial edge of the rectus complex on each side.
Attempt to simulate midline reapproximation of the rectus complexes by bringing the two sides toward each other.
If too much tension is present, which may result in fascial cheese wiring or inability to obtain primary musculofascial reapproximation, start with unilateral component separation and reassess.
If still there is too much tension after unilateral component separation, perform bilateral component separation.
Positioning
Supine with arms abducted 90 degrees and all pressure points padded
Approaches
Multiple approaches are possible for component separation.
Anterior component separation through the hernia defect itself:
Open
Minimally invasive
Anterior component separation through separate lateral incisions: Endoscopic
Posterior component separation: Transversus abdominis release (TAR)
TECHNIQUES
▪ Open Anterior Component Separation
Identify the medial rectus reflection on each side.
Using Bovie electrocautery, dissect from medial to lateral just above the anterior rectus sheath along the anterior rectus fascia. Multiple vascular perforators may be encountered depending on the extent of the dissection.
In the classic open anterior component separation, these perforators are sacrificed and wide skin flaps are developed.
In more modern perforator-sparing anterior component separation approaches, they are identified and preserved or remain undissected by limited undermining and preservation of composite tissue to decrease complication rates.
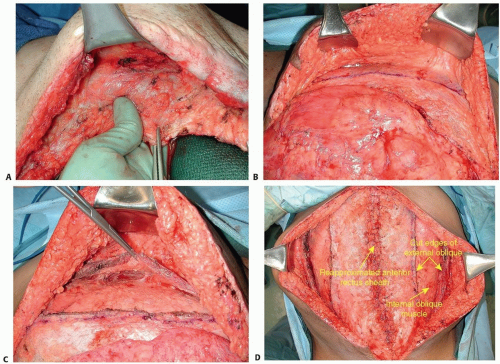
TECH FIG 1 • A. “Tube of toothpaste” maneuver: the rectus complex is displaced laterally in order to accentuate the linea semilunaris. B. Marking of the external oblique aponeurotomy in classic “Ramirez-style” open anterior component separation. C. Elevation of the external oblique muscle off the underlying internal oblique muscle in an areolar, avascular plane, up to the midaxillary line in classic “Ramirez-style” open anterior component separation. D. Closure of the anterior rectus sheath after bilateral classic “Ramirez-style” open anterior component separation. Note the degree of medial advancement obtained.
Identify the semilunar line either by palpating the lateral rectus complex margin between your fingers (intraperitoneal) and thumb (extraperitoneal) or by displacing the rectus muscle laterally.
This latter maneuver, described by the senior author as the “tube of toothpaste maneuver” (TECH FIG 1A), accentuates the indentation of the semilunar line, making it more visible.4
Once the semilunar line is fully exposed, make an incision in the external oblique aponeurosis 2 cm lateral to the semilunar line (TECH FIG 1B).
Enter the plane between the external oblique and internal oblique muscles. This plane is identified by the presence of an avascular layer between the two muscles.
Using a blunt dissection instrument (such as a plastic Yankauer suction), bluntly dissect the plane superiorly and inferiorly. Then use Bovie electrocautery to continue the external oblique aponeurotomy from the iliac crest inferiorly to 6 cm above the costal margin superiorly.
Superiorly, the aponeurosis is more muscular, and care must be taken to obtain adequate hemostasis as the muscle is incised.
Apply two Allis clamps to the medial edge of the cut external oblique muscle, and lift it off the underlying internal oblique muscle.
Place a wide malleable on the internal oblique to push it posteriorly, and use Bovie electrocautery or a spreader-dissector to dissect the plane between the external and internal oblique muscles from medial to lateral (TECH FIG 1C).
This plane should be dissected laterally until sufficient release is performed, varying between the anterior axillary line and posterior axillary line, if needed.
Near the posterior axillary line, the vascular pedicle to the external oblique muscle will be encountered along its undersurface and should be preserved.
This technique allows advancement of 5, 10, and 3 cm in the epigastric, waistline, and suprapubic areas, respectively, on each side (TECH FIG 1D).5
If needed, the retrorectus space can be entered by incising along the medial rectus reflection, identifying the rectus muscle, and keeping the anterior rectus sheath and muscle together as a complex, as well as dissecting the space between the muscle and the posterior sheath.
Segmental neurovascular bundles (which enter laterally) should be visualized and preserved.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree