Trichoscopy (hair and scalp dermoscopy) analyzes the structure and size of growing hair shafts, providing diagnostic clues for inherited and acquired causes of hair loss. Types of hair shaft abnormalities observed include exclamation mark hairs (alopecia areata, trichotillomania, chemotherapy-induced alopecia), Pohl-Pinkus constrictions (alopecia areata, chemotherapy-induced alopecia, blood loss, malnutrition), comma hairs (tinea capitis), corkscrew hairs (tinea capitis), coiled hairs (trichotillomania), flame hairs (trichotillomania), and tulip hairs (in trichotillomania, alopecia areata). Trichoscopy allows differential diagnosis of most genetic hair shaft disorders. This article proposes a classification of hair shaft abnormalities observed by trichoscopy.
Key points
- •
Trichoscopy allows analysis of the structure and size of growing hair shafts.
- •
With trichoscopy is possible to diagnose most genetic hair shaft defects without the need of pulling hairs for light microscopic evaluation.
- •
Hair shaft structure abnormalities may provide diagnostic clues for multiple causes of hair loss beyond genetic hair shaft disorders.
Trichoscopy is dermoscopy of hair and scalp. Among other diagnostic functions, trichoscopy allows analysis of the structure and size of hair shafts. This function has two major applications in clinical practice. First, trichoscopy may replace light microscopy in diagnosing patients with genetic hair shaft defects. Second, the structure of hair shafts may provide a clue for diagnosing multiple conditions beyond classic hair shaft abnormalities. In these disorders, changes in hair shaft structure is secondary to an underlying, acquired pathologic process. Examples of such diseases are tinea capitis, alopecia areata, and trichotillomania.
Normal hairs
A normal terminal hair is uniform in thickness and color throughout its length. An individual may have hair shafts that differ from each other by color and by thickness. Presence of diversely pigmented hairs is a normal finding in graying persons. In children and young adults, simultaneous presence of dark and gray hairs is rare and may be indicative of vitiligo, ectodermal dysplasia, or another other cause of premature graying.
The thickness of normal hairs is usually more than 55 μm. Hair shaft thickness may be roughly estimated with a handheld dermoscope (thin, normal, thick). Some digital dermoscopes (videodermoscopy) allow detailed assessment of hair shaft thickness in micrometers. Precise measurement of hair shaft thickness is not essential for clinical diagnosis, but may be useful for monitoring treatment efficacy, especially in clinical trials.
Terminal hairs may have a medulla that is continuous, interrupted, fragmented, or absent. The impression of a fragmented medulla results from a thick medulla separated by thin medulla that is not visible by trichoscopy. The thickness or presence of a medulla has no influence on hair strength.
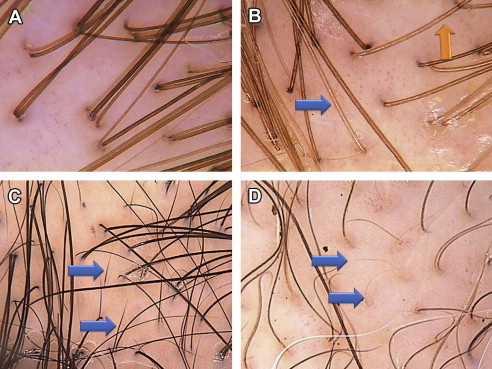
Up to 10% of normal human scalp hairs are vellus hairs. These are hairs that are less than 3 mm long and less than 30 μm thick. An increased proportion of vellus hairs may be present in androgenetic alopecia and in long-lasting alopecia areata. Vellus hairs are more visible in patients with dark skin phototypes. They have to be differentiated from short, healthy regrowing hairs ( Table 1 ). Variants of normal hairs are presented in Fig. 1 .
| New Regrowing Hairs | Vellus Hairs |
|---|---|
| Short (usually 3–5 mm) | Very short (below 3 mm) |
| Thin (below 50 μm) | Very thin (below 30 μm) |
| Normally pigmented | Hypopigmented |
| Upright position | Wavy shape |
| Firm appearance | Weak appearance |
| Pointed distal end | Blurred distal end |
Normal hairs
A normal terminal hair is uniform in thickness and color throughout its length. An individual may have hair shafts that differ from each other by color and by thickness. Presence of diversely pigmented hairs is a normal finding in graying persons. In children and young adults, simultaneous presence of dark and gray hairs is rare and may be indicative of vitiligo, ectodermal dysplasia, or another other cause of premature graying.
The thickness of normal hairs is usually more than 55 μm. Hair shaft thickness may be roughly estimated with a handheld dermoscope (thin, normal, thick). Some digital dermoscopes (videodermoscopy) allow detailed assessment of hair shaft thickness in micrometers. Precise measurement of hair shaft thickness is not essential for clinical diagnosis, but may be useful for monitoring treatment efficacy, especially in clinical trials.
Terminal hairs may have a medulla that is continuous, interrupted, fragmented, or absent. The impression of a fragmented medulla results from a thick medulla separated by thin medulla that is not visible by trichoscopy. The thickness or presence of a medulla has no influence on hair strength.
Up to 10% of normal human scalp hairs are vellus hairs. These are hairs that are less than 3 mm long and less than 30 μm thick. An increased proportion of vellus hairs may be present in androgenetic alopecia and in long-lasting alopecia areata. Vellus hairs are more visible in patients with dark skin phototypes. They have to be differentiated from short, healthy regrowing hairs ( Table 1 ). Variants of normal hairs are presented in Fig. 1 .
| New Regrowing Hairs | Vellus Hairs |
|---|---|
| Short (usually 3–5 mm) | Very short (below 3 mm) |
| Thin (below 50 μm) | Very thin (below 30 μm) |
| Normally pigmented | Hypopigmented |
| Upright position | Wavy shape |
| Firm appearance | Weak appearance |
| Pointed distal end | Blurred distal end |
Classification of hair shaft abnormalities in trichoscopy
The authors propose a classification of hair shaft features observed in trichoscopy ( Fig. 2 ). The proposed classification adopts a structure-based approach, also observed in light microscopy, wherever applicable. It distinguishes the following groups of hair shaft abnormalities observed by trichoscopy: (1) hair shafts with fractures, (2) hair narrowings, (3) hairs with node-like structures, (4) curls and twists, (5) bands, and (6) short hairs. We consider hairs as short hairs when the entire hair shaft is visible in one field of view of a dermoscope (10- to 20-fold magnification). These hairs are usually less than 10 mm long.
Many types of hair shaft abnormalities may provide clues for differential diagnosis of inherited and acquired causes of hair loss ( Table 2 ). Examples of hair shaft abnormalities are presented in Fig. 3 .
| Hair Shafts in Trichoscopy | Description | Most Common Clinical Association |
|---|---|---|
| Normal hairs | ||
| Normal hairs | Hairs, uniform in shape and color | Normal |
| Fractured hairs | ||
| Trichoptilosis | Longitudinal splitting of the distal end of hair shaft | Unspecific manifestation of a defect in hair shaft structure |
| Trichoschisis or trichoclasis | A clean transverse fracture across the hair shaft | Trichothiodystrophy, secondary to conditions that weaken the hair shaft |
| Broken (fractured) hairs | Irregular transverse fracture across the hair shaft | Trichotillomania, traction alopecia, alopecia areata, tinea capitis |
| Golf tee hairs | A hair with a concave distal end | Specific for Netherton syndrome |
| Narrowings | ||
| Monilethrix | Hair with regularly distributed nodes and narrowings The nodes correspond to normal hair shaft thickness; the internodes are the narrowings | Specific for monilethrix |
| Monilethrix-like congenital hypotrichosis | As in monilethrix, but the spaces between narrowings are extremely short | Specific for monilethrix-like congenital hypotrichosis |
| Monilethrix-like hairs (Pohl-Pinkus constriction) | Hair with irregularly distributed narrowings (Pohl-Pinkus constrictions) | Alopecia areata, chemotherapy-induced alopecia, bleeding, malnutrition Artificial: monilethrix-like effect from hair styling gel or immersion fluid |
| Pseudomonilethrix | Differs from monilethrix—nodes appear thicker than the normal hair shaft and internodes have the thickness of the normal hair | Controversial |
| Exclamation mark hairs | Hairs with a thin, usually hypopigmented proximal end and thicker, pigmented distal end | Alopecia areata, chemotherapy-induced alopecia, intoxication, trichotillomania |
| Tapered hairs | Long exclamation mark hairs, the distal end is outside the field of view of a dermoscope | Alopecia areata, cicatricial alopecia, trichotillomania, bleeding, malnutrition, chronic intoxication |
| Node-like appearance | ||
| Trichonodosis (hair knotting) | A single or double knot in the hair shaft | No clinical significance |
| Trichorrhexis nodosa | A hair shaft with a restricted area where the shaft splits longitudinally into numerous small fibers The outer fibers bulge out, causing a segmental increase in hair diameter | Multiple acquired and inherited diseases, commonly due to mechanical or chemical trauma |
| Trichorrhexis invaginata (bamboo hairs) | The hair shaft telescopes into itself The proximal part of the abnormality is concave and the distal end is convex (bulging), producing an impression of nodular swelling along the hair shaft | Specific for Netherton syndrome |
| Hair casts (peripilar keratin casts) | Firm, white, tubular masses that encircle the hair shafts | A nonspecific finding, commonly associated with scaling or epidermal detachment Traction alopecia |
| Curls and twists | ||
| Pigtail hairs | Short, regularly coiled hairs with tapered ends | Alopecia areata |
| Coiled hairs | Irregularly coiled hairs with a jagged end When not fully coiled, they may have a hook-like appearance | Trichotillomania |
| Comma hairs | Short, comma-like (C-shaped) hairs, homogeneous in thickness and pigmentation | Tinea capitis |
| Corkscrew hairs | Hairs with multiple twists and coils, forming corkscrew-like structures | Tinea capitis |
| Zigzag hairs | Hairs, bent at sharp angles, form zigzag structures | Tinea capitis, alopecia areata |
| Pili torti | Hairs that are flattened and twisted on their own axis at irregular intervals, usually through an angle of 180° | Associated with multiple inherited and acquired hair diseases |
| Wooly hairs | Hair shafts with waves at very short intervals, giving a crawling snake appearance | Inherited syndromes |
| Bands | ||
| Continuous medulla | Longitudinal white band along the midpart of the hair shaft that covers less than 50% of the hair shaft thickness | Normal |
| Interrupted medulla | Interrupted longitudinal white band along the midpart of the hair shaft The band covers less than 50% of the hair shaft thickness | Normal |
| Pili annulati | Hair shafts with transverse light, blurry, whitish bands covering (nearly) the width of a hair | Inherited hair shaft abnormality; possible association with alopecia areata |
| Interrupted (Morse Code-like) hairs | Hairs with multiple thin white bands across the hair shaft | Tinea capitis |
| Short hairs | ||
| Upright regrowing | New, healthy, regrowing hairs that have a tapered end and a straight-up position | Normal If abundant, may reflect a regrowth phase of telogen effluvium |
| Vellus hairs | Short, thin, hypopigmented, delicate, nonmedullated hairs, usually somewhat wavy in shape | Normal If abundant, may reflect androgenetic alopecia |
| Dark lines | Thin, short, intensely pigmented hairs, appearing tapered at both sides | Noncicatricial alopecia |
| Tulip hairs | Short hairs with a tulip leaf-like hyperpigmentation at the distal end | Trichotillomania |
| Block hairs | Very short hairs with a transverse horizontal distal end | Noncicatricial alopecia associated with shaft hair fragility |
| i-Hairs | i-Hairs are block hairs with an accented dark distal end | Noncicatricial alopecia associated with high shaft hair fragility (eg, tinea capitis) |
| Broom hairs | Few or more linear, short hairs emerging from one follicular opening | Observed in diverse entities, both cicatricial and noncicatricial |
| Broom fibers | Few or more linear, short, dark fibers (significantly thinner than terminal hairs) emerging from one follicular opening | Observed in diverse entities, both cicatricial and noncicatricial |
| Flame hairs | Hair residues, semitransparent, wavy, and cone-shaped, resembling a fire flame | Trichotillomania |
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


