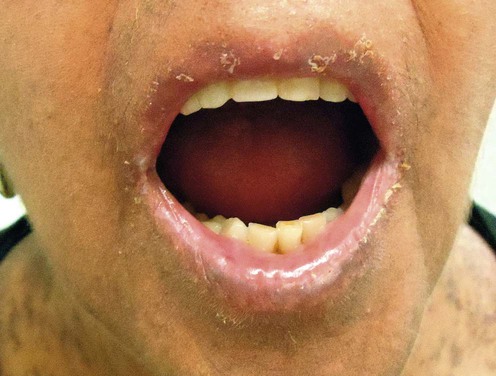
Graft-versus-host disease
Get Clinical Tree app for offline access
Acute gvhd
Specific investigations
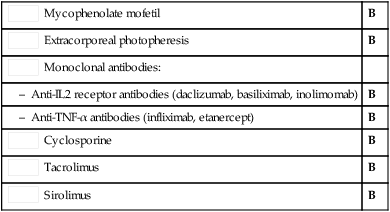
Second-line therapies

Graft-versus-host disease
Get Clinical Tree app for offline access
Acute gvhd
Specific investigations
Second-line therapies








 Corticosteroids (methylprednisolone 2 mg/kg/day)
Corticosteroids (methylprednisolone 2 mg/kg/day) Mycophenolate mofetil
Mycophenolate mofetil Extracorporeal photopheresis
Extracorporeal photopheresis Monoclonal antibodies:
Monoclonal antibodies: Cyclosporine
Cyclosporine Tacrolimus
Tacrolimus Sirolimus
Sirolimus