Chapter 53 Graft Tensioning in Anterior Cruciate Ligament Reconstruction
Introduction
On the basis of clinical experience, pioneers of current ACL reconstruction procedures preferred to apply relatively high initial tension to not only the doubled pes tendon autograft but also the patellar tendon autograft at the time of fixation.1–4 For example, Clancy et al1 performed ACL reconstruction using the distally stacked and proximally free central third of the patellar tendon as an autograft and recommended that the patellar bone block be pulled with three sutures through the femoral tunnel as far as it would go within the tunnel. On the other hand, a number of in vitro and in vivo experimental studies suggested that a high initial tension had detrimental effects not only on the graft but also on the knee after ACL reconstruction. Some recent studies, however, reported that a high initial tension was better than a low initial tension in simulation of a middle- or long-term effect. Thus there has been considerable disagreement on the effects of initial graft tension among the previous studies. It has been necessary therefore to conduct randomized clinical trials on the effect of initial graft tension on the outcome after ACL reconstruction. At the present time, four articles on the effect of initial graft tension on the clinical outcome are available for review. In this chapter, the author reviews recent experimental and clinical studies on the effect of graft tensioning during ACL reconstruction on the graft and the ACL reconstructed knee and explains what has and has not been clarified at the present time.
In Vitro Biomechanical Studies on Graft Tensioning
The Effect of the Initial Tension on the Tension-Flexion Curve
In the normal knee, tension in the normal ACL decreases with knee flexion from the maximum value obtained at 0 degrees to the minimum value near 30 degrees and then slightly increases with further flexion.5,6 This relationship between the ACL tension and the knee flexion angle is well known as a tension-flexion curve. In ACL reconstruction, the initial tension is defined as a tension applied to the graft at a selected angle of knee flexion during surgery. Then we should know the effect of the initial tension on the tension-flexion curve in ACL reconstruction. In vitro biomechanical studies5,7 reported that in the standard single-bundle ACL reconstruction procedures, increase of the initial tension applied at some angle of knee flexion increased the graft tension by a constant magnitude at every flexion angle during knee motion and that consequently the shape of the tension-flexion curve was not changed (Fig. 53-1). Namely, it means that an increase of the initial graft tension at 30 degrees of knee flexion results in an increase of the graft tension at every knee flexion angle. In 2001, Fleming et al8 measured the laxity in nine different tensioning conditions: three tension magnitudes (30, 60, and 90N), each applied with the knee at three angles (30, 60, and 90 degrees), in a goat ACL reconstruction model using a bone–tendon–bone (BTB) graft. They stated that both the graft tension and the knee angle produced significant changes on anteroposterior laxity values.
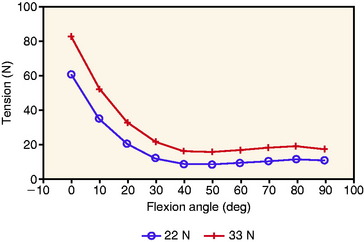
These in vitro studies indicated that both the initial tension value and the knee flexion angle at the time of tensioning and fixation are critical in the ACL reconstruction. In the standard ACL reconstruction procedures, when a surgeon applies a certain “initial” tension value at about 30 degrees of knee flexion, a graft tension value obtained at more extension positions or more flexion positions is greater than the initial tension value.7 Conversely, when a surgeon applies a certain initial tension value at the full extension position of the knee, graft tension values at flexion positions are lower than the initial tension value. Clinically, a number of surgeons have preferred to fix the graft at approximately 30 degrees of knee flexion in order to avoid an insufficient tension after surgery, specifically for the hamstring tendon graft. On the other hand, recently many surgeons who perform ACL reconstruction with the BTB graft have preferred to fix the graft at the full extension position to avoid postoperative flexion contracture of the knee due to overtensioning of the graft.
Relaxation of Graft Tension after Surgery
In vitro biomechanical studies have shown that viscoelastic creep of the graft causes relaxation of graft tension. Howard et al9 quantified viscoelastic creep in the BTB graft using both an in vivo and an in vitro model. In the in vivo model, 10-mm BTB grafts were elongated by 14.0% after 89N was applied for a minimum of 4 minutes. In the in vitro model, grafts were elongated by 10.1% after 89N was applied for 15 minutes. This study highlights the importance of the time for preconditioning the graft before grafting.
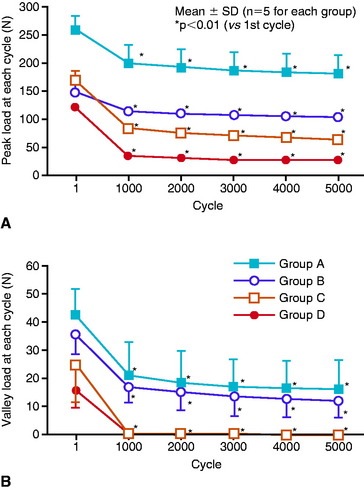
The author and his colleagues10–12 reported that more obvious relaxation of graft tension occurred due to elongation of a bone–graft–bone complex that is composed of bones, tendon grafts, and all artificial materials to be used for graft fixation. They measured the influence of 5000 cycles of submaximal cyclical displacement upon the tension of various types of the bone–graft–bone complex after ACL reconstruction. For example, Yamanaka et al10 showed that initial tension of 80N applied to the four-strand flexor tendon graft tethered to the screw post with a suture was reduced to 0N after 5000 cycles of 2-mm stretching, while the same initial tension applied to the BTB graft fixed with interference screws was reduced to 17N (Fig. 53-2). In addition, the relaxation rate in the BTB graft fixed with interference screws was less than that in the BTB graft fixed with sutures and screw posts, whereas the relaxation rate in the flexor tendon graft fixed with sutures and screw posts was greater than that in the BTB graft fixed with the sutures and screw points (see Fig. 53-2). Boylan et al13 applied an initial tension of 68N, 45N, and 23N to the hamstring graft at 30 degrees of flexion, fixed with a suture and post technique. After 1000 cycles of knee motion between 0 and 90 degrees, the tension in the graft decreased to 34.5N, 16.8N, and 15.4N, respectively. Arnold et al14 applied 40N initial tension to the BTB graft at 20 degrees of flexion in ACL reconstruction with cadavers, fixed with interference screws. The graft tension at 0 degrees of flexion dropped from 208N, or by 41% at 500 cycles. Anterior laxity increased from +1.4 to +2.8 mm by 500 cycles.
Effects of a High or Low Initial Tension on the Graft and the Knee
A number of in vitro studies with cadaver knees, which simulated conditions immediately after ACL reconstruction, showed that an increase of ACL tension decreased the degree of anterior translation of the tibia to the femur.7,15–17 Melby et al17 described that an 18N tension applied to the graft at 30 degrees of knee flexion restored the laxity and stiffness most closely resembling that of the intact knee, without inducing significant abnormal laxities, but that tensions greater than 54N overconstrained the knee. Several in vitro studies warned that overtensioning might result in restriction in range of motion and graft failure.18–20 For example, Nabors et al19 showed that when a high initial tension was applied to the BTB graft at 30 degrees of knee flexion, loss of knee extension frequently occurred after surgery. Graf et al20 indicated that a high tension induced wear-related graft failure. Eager et al21 reported that a high initial tension induced posterior subluxation of the tibia with respect to the femur, specifically when a graft having low stiffness was used. Thus the just-described in vitro studies recommended a low initial tension be applied to the graft in ACL reconstruction.
However, a criticism of these in vitro studies is that they did not take the graft relaxation into account. Beynnon et al15 reported that because the tension applied on a graft at the time of fixation was acutely decreased by creep elongation of an autograft or transposition of an autograft in the bone tunnel, insufficient initial tension applied on the graft during surgery might result in slackness of a reconstructed ligament tissue. In 2002, Numazaki et al12
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Anterior Cruciate Ligament Reconstruction Utilizing the Rigidfix for Femoral-Sided Fixation
Anterior Cruciate Ligament Reconstruction Utilizing the Rigidfix for Femoral-Sided Fixation
 Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
 High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


