CHAPTER 11 Gluteal Flap Breast Reconstruction

Summary/Key Points
Patient Selection
Breast reconstruction using autologous tissue has been performed for several decades and has become a safe and reliable technique.1 Abdominal flaps, either pedicled or free, remain the first choice for breast reconstruction using autologous tissue. However, in patients who are very thin or who had previously undergone abdominoplasty or prior breast reconstruction with an abdominal flap, a gluteal flap can be an excellent alternative.2–5
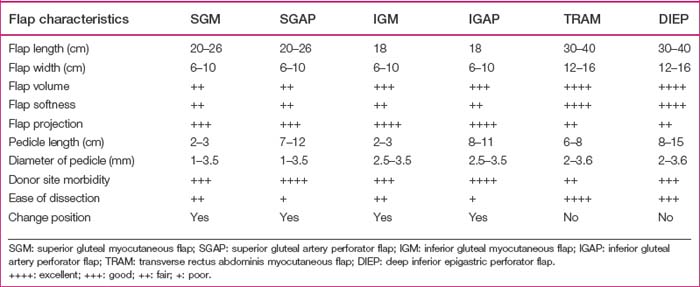
The reconstructed breast mound using gluteal flaps may have more projection, but not be as soft or mobile as when using abdominal flaps. Patient selection should be based on the patient’s individual characteristics, such as the volume of tissue required to achieve symmetry with the contralateral breast, the donor flap size, the pedicle length and caliber, and the relative advantages and disadvantages of each flap (Table 11.1). In patients with inadequate abdominal tissue or in whom an abdominal flap had been used before, gluteal flaps present an alternative for autologous breast reconstruction.6–8 Selection between the SGAP or IGAP flap depends on the patient’s desired scar position, distribution of adiposity, and where sizable perforators can be found (Table 11.1). In patients with a sagging buttock, the IGAP flap is usually preferred. We prefer to harvest a perforator flap rather than a myocutaneous flap to obtain a longer pedicle and to avoid sacrifice of the gluteus maximus muscle.
Indications
Indications for using gluteal flaps for breast reconstruction include:
Contraindications include previous buttock surgery, buttock liposuction or buttock lift, and heavy tobacco use. Dissection of the SGAP or IGAP flap is technically demanding and is better done by an experienced reconstructive microsurgeon. It is especially difficult in Asian women, who are relatively thin and have tiny perforators.6–8
Operative Technique
Surgical anatomy
After emerging from the external iliac artery, the superior and inferior gluteal arteries pass through the sciatic foramen and become the dominant pedicles of the gluteal maximus muscle. The superior gluteal artery runs superior to the piriformis muscle and gives several branches to the gluteus maximus muscle. A few musculocutaneous perforators go through the gluteus maximus muscle and supply the superolateral aspect of the buttock. The diameter of the major perforators ranges from 1.0 to 1.5 mm in Koshima’s series and averages 3.5 mm in Allen’s report.9,10 This disparity is probably due to the differences among races. The mean pedicle length from the perforator is 8 cm (Table 11.1).
The inferior gluteal artery runs inferior to the piriformis muscle and proximal to the coccygeus muscle. During passage through the sciatic foramen, the inferior gluteal artery is accompanied by the internal pudendal vessels, sciatic nerve, posterior cutaneous nerve of the thigh, and pudendal nerve. It supplies the inferior part of the gluteus maximus muscle. Musculocutaneous perforators pass through the muscle and supply the inferomedial aspect of the buttock. During its intramuscular course on the way to the subcutaneous tissue, the pedicle runs distally, accompanied by the posterior cutaneous nerve of the thigh. To avoid injury to these adjacent neurovascular structures, the dissection of the IGAP flap is more technically demanding than the SGAP flap.11,12 The perforators of the inferior gluteal artery are located along a line in the middle third of the gluteal region above the gluteal crease.13 The diameter of the inferior gluteal artery can be greater than 2 mm when dissection continues to their origin. Average pedicle length is 8 to 11 cm. The mean internal diameter of the perforators was 0.6 ± 0.1 mm in cadaveric dissections.13
Preoperative marking and flap dissection
Superior gluteal artery perforator flap
Preoperative marking
Preoperative marking is done with the patient in the prone or lateral decubitus position. A line is marked from the posterior superior iliac spine to the greater trochanter. The superior gluteal artery is located at the medial one third of this line.3,4 Two or three audible perforators are usually detectible by hand-held pencil Doppler. An elliptical skin paddle is designed around the perforators and its axis can be oriented transversely or obliquely (Fig. 11.1).

Flap dissection
After reaching the subfascial plane, dissection is carried out from lateral to medial to identify the perforators. One large perforator is usually enough to supply the entire flap. After choosing the largest perforator, dissection is continued by splitting the gluteus maximus muscle along the direction of its fibers. A self-retaining retractor is used to spread the fibers of the gluteus maximus muscle. When proceeding to the deeper layer, good exposure of the surgical field by retracting the piriformis muscle is crucial to allow a clear visualization and to prevent any vascular damage. During dissection, any side branches or sacrificed perforators should be adequately coagulated or clamped with hemoclips to prevent postoperative hematoma or seroma accumulation. The perforator is traced to its proximal origin to gain as long a pedicle as possible. A longer pedicle can be obtained by using a perforator located more laterally in the flap. A pedicle averaging 8–12 cm in length can be dissected (Table 11.1
Related posts:
 Saline Implants: Getting a Good Result
Saline Implants: Getting a Good Result
 Surgery of the Breast in Poland’s Syndrome
Surgery of the Breast in Poland’s Syndrome
 Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
 Autologous Flap Use in Breast Reshaping after Massive Weight Loss
Autologous Flap Use in Breast Reshaping after Massive Weight Loss
 Fat Injections to the Breast: The Lipomodeling Technique
Fat Injections to the Breast: The Lipomodeling Technique
 Subfascial Breast Augmentation
Subfascial Breast Augmentation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


