The Glidelift is an innovative approach that meets the demand for an operation that integrates the substantial outcomes of surgical approaches with the esthetic subtlety of minimally invasive techniques. It merges tried-and-tested practices with fresh, inventive concepts. This amalgamation results in a unique and effective solution for facial rejuvenation that concurrently minimizes visible scarring.
Key points
- •
Noninvasive methods can only give limited effects in comparison to surgery but have the benefit of not leaving a visible scar.
- •
A proper patient evaluation is vital when deciding the type of surgical intervention required.
- •
Knowledge of the facial nerves and their trajectories is essential.
- •
The Glidelift can be combined with other procedures to provide comprehensive facial rejuvenation.
- •
The surgical net has opened new horizons in esthetic surgery.
Video content accompanies this article at http://www.advancesincosmeticsurgery.com .
Introduction
Facial esthetic surgery has a rich history dating back to the early twentieth century when it was first introduced as a means of correcting facial deformities and age-related changes, typically appealing to those in their late 50s and 60s. With advancements in science and technique, surgical facelifts evolved to offer a more comprehensive solution to facial rejuvenation [ ]. However, the advent of the twenty-first century saw an increase in the prevalence of noninvasive procedures, primarily due to their less noticeable scarring and significantly improved options that enhanced procedure quality. The preference for noninvasive procedures, especially among the 36 to 50 age bracket, surged significantly, with this demographic accounting for 41% of nonsurgical procedures performed in 2021 [ ].
Although nonsurgical and minimally invasive procedures offer significant advantages such as reduced scarring and shorter recovery times, their capabilities are inherently limited in terms of the level of anatomic correction that can be achieved. Some intricate surgical techniques, such as endoscopic approaches, are designed to minimize scars while delivering surgical results. These procedures provide greater precision, but require extensive training and expensive endoscopic equipment, making them less attainable for many practitioners [ ].
Recognizing these limitations, this article introduces the “Glidelift,” an innovative procedure that amalgamates the precision of surgical intervention with the appeal of minimally invasive techniques. Although the Glidelift requires a learning curve, this is balanced by the fact that it is a fusion of existing techniques and thus is within reach of any plastic surgeon with adequate training. Moreover, it eliminates the need for costly endoscopic equipment, making it a more accessible technique.
The Glidelift offers a comprehensive approach to periorbital shaping and midface lifting through non-visible, hidden incisions. This procedure not only draws on established practices in the field but also introduces new concepts that make it a unique addition to the surgical repertoire [ , ].
Surgical anatomy
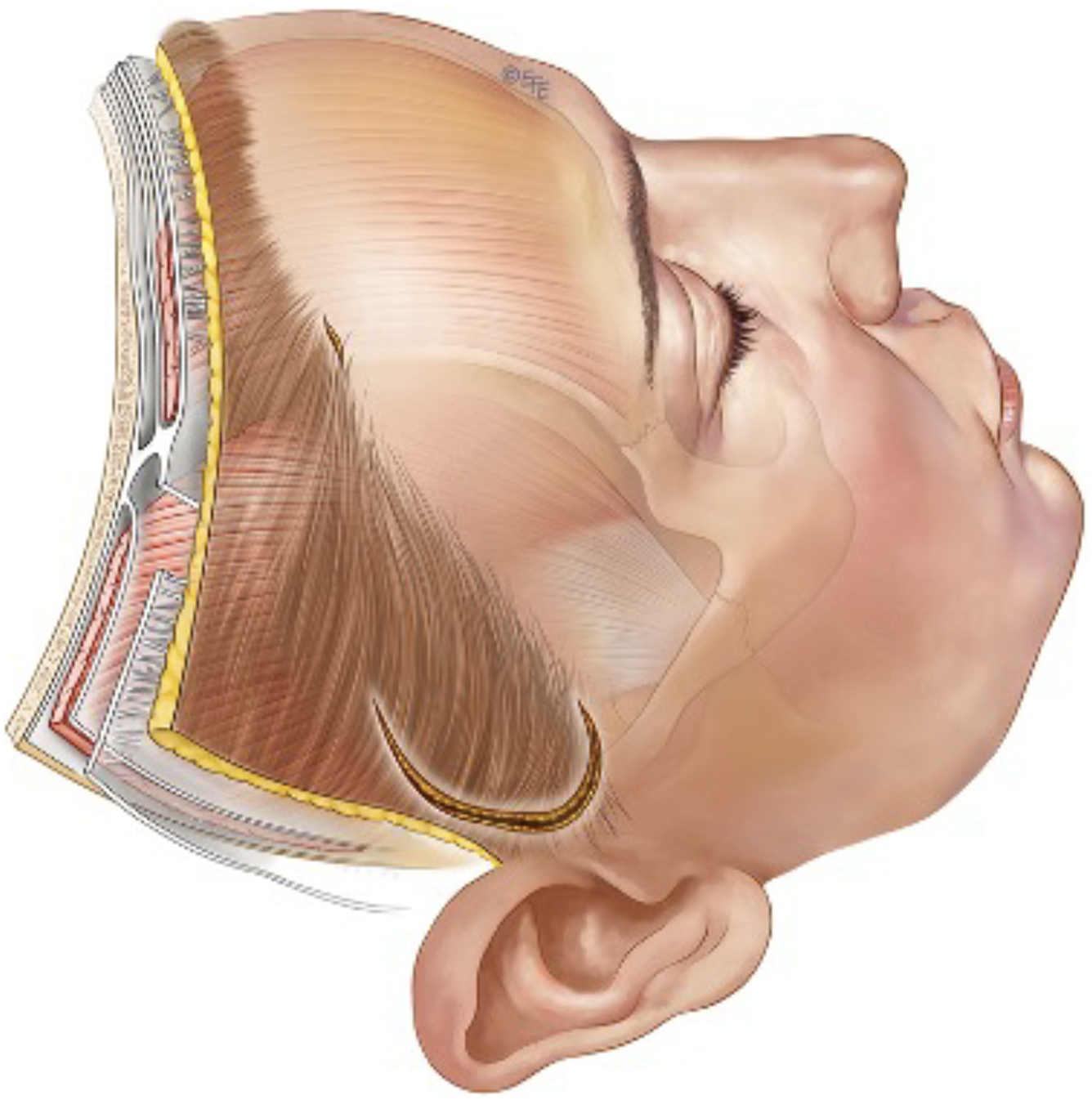
Just as with traditional facelift procedures, the Glidelift operates in a surgical plane above the superficial musculoaponeurotic system (SMAS) layer [ ]. This strategic positioning safeguards the facial nerves from potential harm, allowing for appropriate plication of the mobile SMAS via sutures without risking exposure of the nerves lying beneath. Moreover, the procedure enables a vertical plication of the SMAS without necessitating the division of the zygomatic and masseteric retaining ligaments. This is accomplished as the subcutaneous dissection is extended medial to these retaining ligaments, which is not traditionally done during a deep plane or sub-SMAS facelift, and thus would require the division of the retaining ligaments to achieve a similar vector of plication [ ] ( Fig. 1 ).
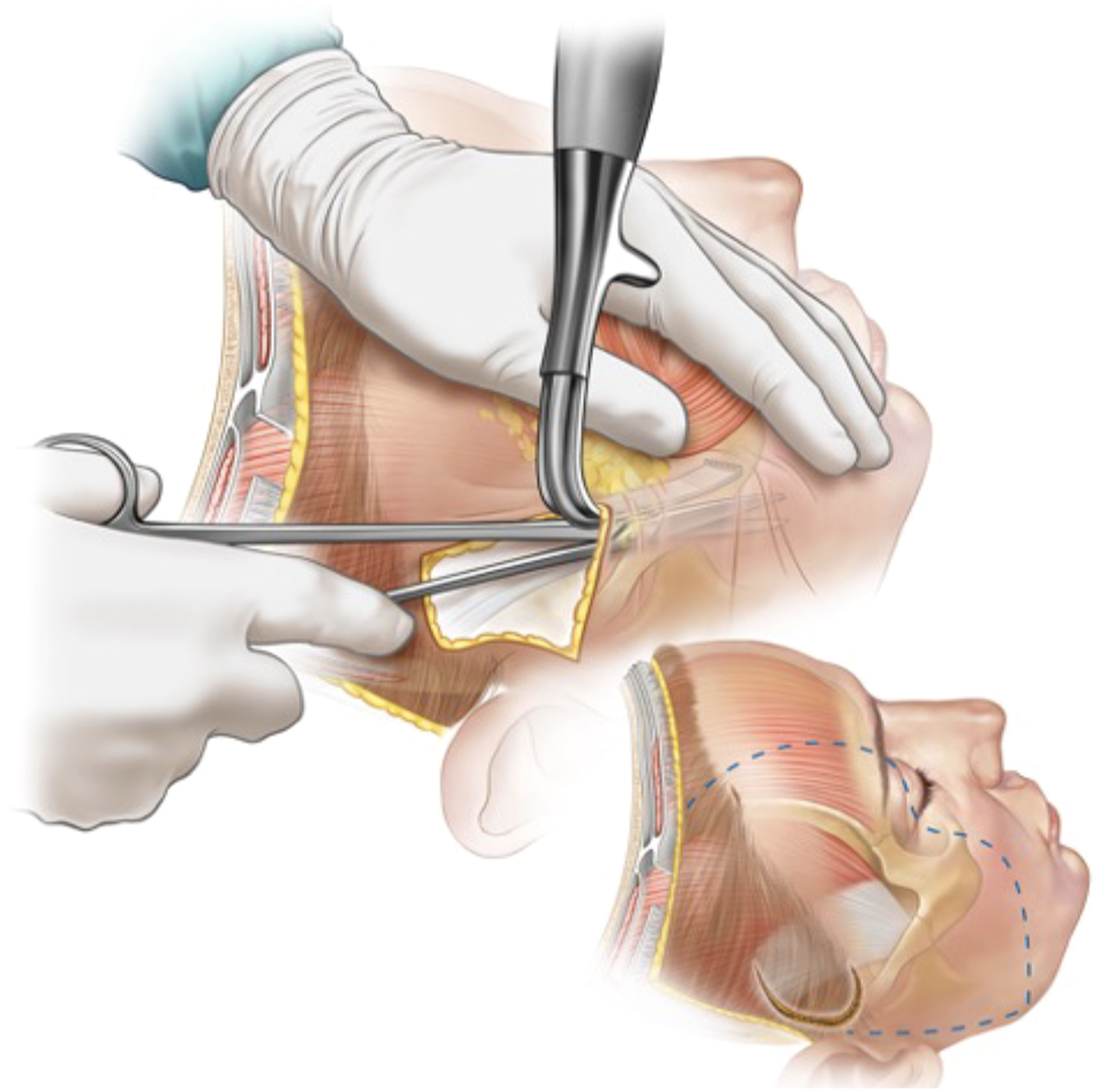
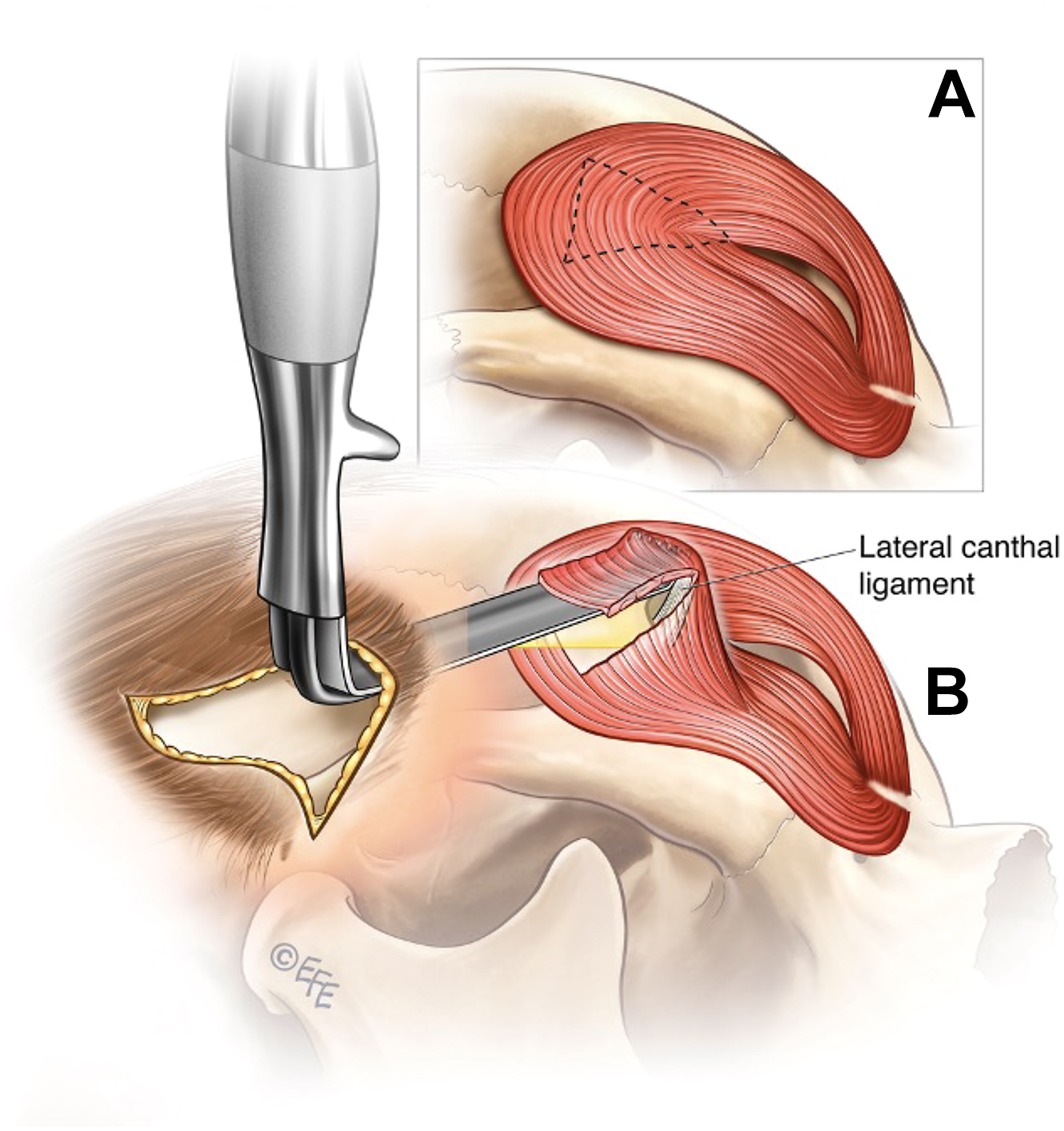
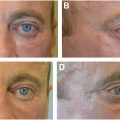
When the procedure approaches the region of the lateral orbit, the intricacies of the anatomy require a nuanced approach. Given the thin skin in this area, the technique modifies the approach slightly; the skin and subcutaneous flap at this point include a portion of the lateral orbicularis muscle. This integration allows for precise identification of the lateral canthal ligament, facilitating manipulation if necessary ( Fig. 2 ).
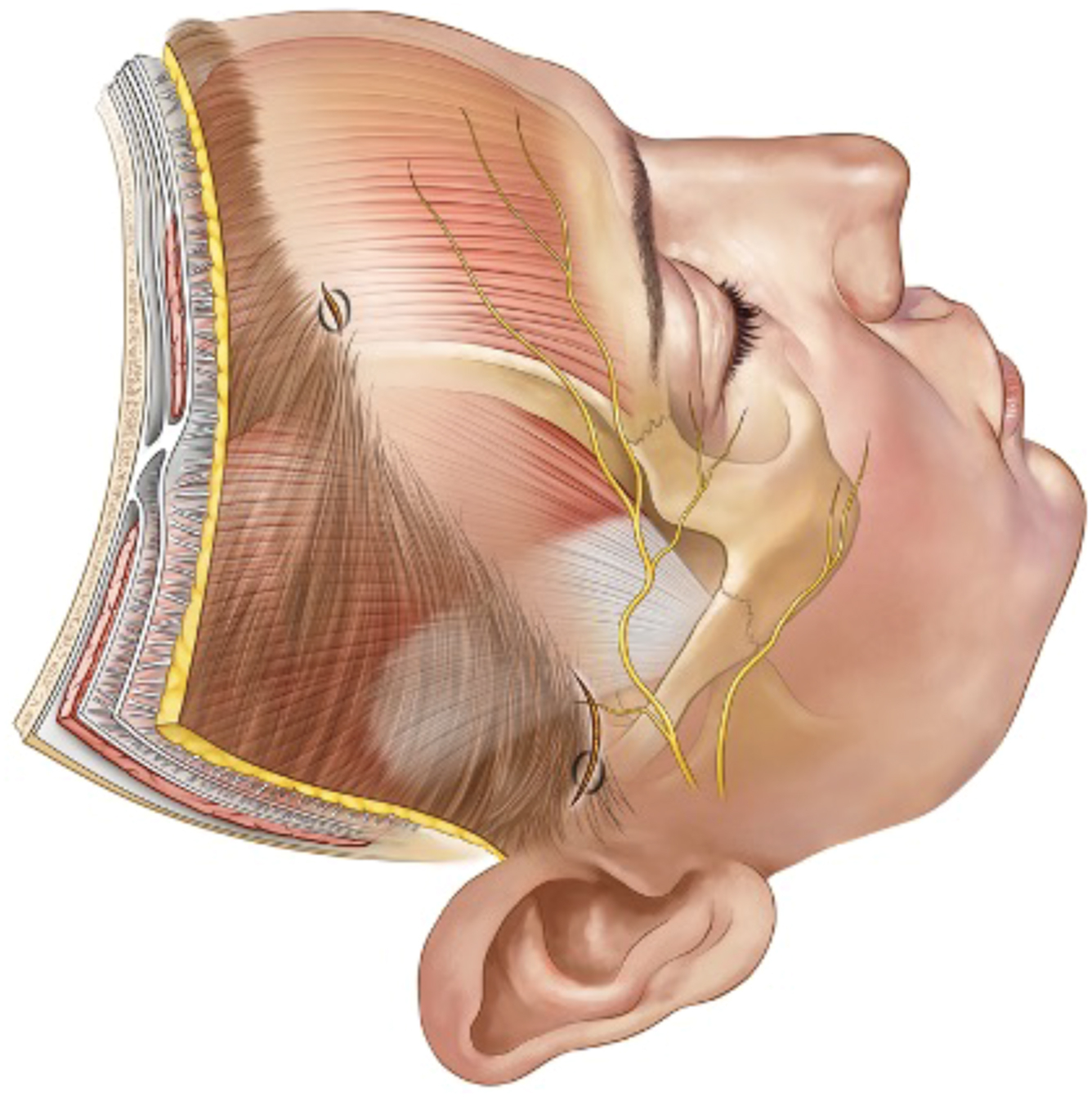
A crucial consideration throughout the Glidelift is the pathway of the frontal branch of the facial nerve. Pitanguy’s line, which is defined as a line drawn from 0.5 cm below the tragus to 1.5 cm above the lateral eyebrow, represents a key anatomic landmark in facial plastic surgery as it approximates the course of the frontal branch of the facial nerve and thus provides a vital reference for safe suture placement ( Fig. 3 ). Any suture placement should respect this anatomic path to minimize the risk of potential injury to the facial nerve [ ].
Indications and contraindications
The patient selection criteria for the Glidelift procedure primarily involve patients who fall into the age range of 35 to 50 year. These are typically individuals who are suitable for a facelift, yet without excessive skin and are averse to the scarring associated with conventional facelifts. Conversely, those who need skin removal or have significant lower facial aging, such as pronounced jowls or marionette lines, do not fit the criteria for this procedure.
An essential part of the patient consultation involves explaining that if better results could be obtained with a traditional facelift that should be the preferred treatment plan. Patients who are borderline, often around the age of 50 year, should be informed that they might require a conversion to a traditional facelift for optimal results.
Moreover, as with all surgical procedures, the wishes of the patient must be acknowledged. Even though the Glidelift encompasses both periorbital shaping and a midface lift, it can be executed solely as a midface lift if the patient prefers no alterations around the eye. It is frequently performed in conjunction with a short scar neck lift, but various other supplementary procedures can also be incorporated if desired, such as rhinoplasty, micro fat grafting, and upper and lower blepharoplasty, enabling a comprehensive approach to facial rejuvenation.
Perioperative considerations necessitate a comprehensive review of the patient’s past medical history to identify potential complications. Factors such as blood pressure, coagulation, smoking habits, healing tendencies, scarring, and autoimmune diseases, which might complicate either the surgical procedure or the recovery, should be thoroughly examined.
Although the Glidelift can offer substantial benefits in certain cases, the complexity of the procedure highlights the need for detailed patient counseling and a comprehensive understanding of the associated risks and limitations.
Preoperative markings and incision placement
Markings for the Glidelift are determined by assessing the face preoperatively. Areas lacking volume are marked for potential fat grafting, as well as areas with excess fat that might be suitable for micro-liposuction. The planned dissection over the midface is marked to ensure adequate release and the extent of the forehead dissection is also marked, which depends on the type of brow lift required.
The Glidelift procedure then begins with the creation of two strategically placed access incisions. The first incision is made in the lateral forehead, concealed within the hairline, and the second is positioned just below the hair in the sideburn area (see Fig. 3 ). These incisions serve as gateways for the formation of small tunnels in distinct anatomic planes that are subsequently interconnected. This connection enhances visibility through the minimal incision, permits the repositioning of excess skin in the temporal scalp without excising it, and thereby sets the foundation for the Glidelift.
After these initial tunnels have been established, the procedure continues with the extension of the sideburn incision by approximately 3 cm into the temporal hairline ( Fig. 4 ). This extension provides the necessary access and visualization for the remainder of the dissection while maintaining a focus on minimizing visible scarring.
Intraoperative management
Anesthesia
All procedures are typically performed under general anesthesia, although occasionally conscious sedation combined with local anesthesia may be used based on individual patient factors and surgeon preference.
Before making incisions, local anesthesia is applied to the specific operative sites. Once the incisions are established, a tumescent solution is introduced to further facilitate the surgical procedure. This solution comprises a balanced mixture of normal saline, lidocaine, epinephrine, hyaluronidase, and tranexamic acid ( Table 1 ). This tumescent solution is infiltrated into the operative areas including the forehead and face, with a typical volume of approximately 400 mL in total. The administration of this solution aids in creating the appropriate dissection plane and helps to control bleeding throughout the procedure.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


