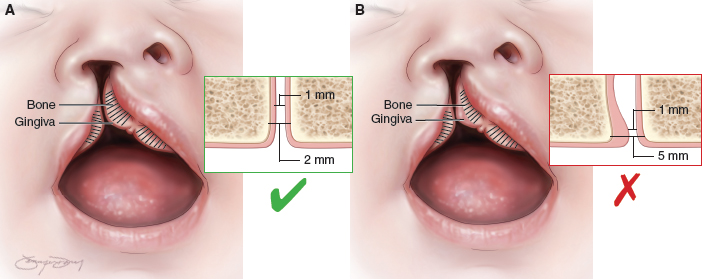
68 ○ Advocates of gingivoperiosteoplasty state that the primary benefit at initial cleft lip repair is to decrease the need for secondary alveolar bone grafting. ○ Critics of gingivoperiosteoplasty are concerned about the risk of iatrogenic restriction of facial growth and malocclusion resulting from early closure of the alveolar arch. ○ In a gingivoperiosteoplasty procedure the soft tissue barrier is surgically removed within the alveolar cleft and replaced with a gingivoperiosteal tunnel that facilitates bone healing through guided tissue regeneration. ○ The nasoalveolar molding–gingivoperiosteoplasty method differs not in the technical surgical details of the GPP but in the method of presurgical molding of the alveolar segments in preparation for the GPP and the criteria for selecting appropriate candidates. The primary goal of cleft care is to optimize function, appearance, and the patient’s self-image with a minimum of surgical intervention. However, the international cleft community continues to debate how best to attain this goal. One of the most controversial topics of debate in current cleft care is management of the alveolar cleft, specifically the indications for primary gingivoperiosteoplasty (GPP). The theory of GPP is consistent with the goal of minimizing the number of secondary surgeries by optimizing results of primary surgery. Advocates of GPP report that the primary benefit obtained at the time of initial cleft lip repair is the elimination of secondary alveolar bone grafting at the time of mixed dentition. This prevents the potential morbidity and cost of an additional surgery. Critics of GPP, in contrast, are concerned about the risk of iatrogenic restriction of facial growth and malocclusion resulting from early closure of the alveolar arch, which can lead to deteriorating facial projection with age, extensive orthodontics, and an increased risk of additional orthognathic surgeries at skeletal maturity. Thus the debate regarding GPP in infants with clefts centers on weighing the chance of preventing secondary bone grafting against the risk of increased treatment that is required when facial growth is restricted. Initially described as “boneless bone grafting,” the basic principle of GPP is to surgically remove the soft tissue barrier within the alveolar cleft and replace it with a gingivoperiosteal tunnel that facilitates bone healing through guided tissue regeneration (GTR). In contrast to more traditional surgical reconstructive techniques, which use similar tissues from other parts of the body to repair defects, GPP is a form of inductive surgery, similar to distraction osteogenesis, that creates a favorable environment for augmented local healing and tissue generation. The benefit of inductive surgery is the lack of donor morbidity. The importance of the periosteum in bony healing has been well documented by a number of authors, but Ollier is most often credited with first emphasizing the osteogenic potential of the periosteum.1–3 The application of GTR in the healing of mandibular bony defects was first reported by Dahlin et al.4 He demonstrated bony union of critical mandibular defects by creating a Teflon tunnel to guide bone regeneration while impairing soft tissue in-growth and fibrous nonunion. More recent research on GTR in calvarial defect healing indicates that not only is an intact tunnel important for bony bridging to occur, but the nature of the guiding tissue (periosteum versus dura versus alloplast) is equally important.5 Age also appears to have a major effect; tissues have augmented guiding regeneration capacity in immature compared with mature animals.6 Based on these principles, the potential of GTR after GPP is dependent on the integrity of the guiding tunnel to restrict fibrous in-growth, the presence of viable periosteum in the created flaps, and the age of the patient. References to the osteogenic properties of mucoperiosteum in healing a cleft palate date back to Langenbeck’s descriptions7 in the 1800s, but it was not until Tord Skoog’s descriptions of primary GPP in the 1960s that the technique became popular in cleft care.8 Skoog credited a case of unexpected maxillary regeneration for his interest in alveolar periosteoplasty. He performed a subperiosteal maxillectomy in a 4-month-old patient; the patient’s maxilla spontaneously regenerated without bone grafting. This case led him, and others, to consider the possibility that bone grafts are primarily conductive frameworks for bony regrowth rather than the traditional concept that they bring bone-healing cells to the area. In 1967 Skoog published his experience with what he termed boneless bone grafting in a series of 83 patients aged 3 to 6 months.8 In this paper he described the creation of local mucoperiosteal flaps to bridge unmolded alveolar clefts in a similar fashion to the flaps used for secondary bone grafting. Rather than adding bone graft to the bony defect, however, Skoog inserted oxidized regenerated cellulose and subsequently found bony bridge formation across the alveolar cleft. Although not every patient grew bone initially, with repeated periosteal flaps, all patients eventually formed a bony bridge.9 The bone formation was assessed by radiograph and confirmed by histochemical analysis, but Skoog did not provide any information on the amount of bone or the subsequent need for secondary bone graft. Because the Skoog method of GPP was performed on unmolded wide alveolar clefts, it required extensive undermining of mucoperiosteal flaps across the face of the maxilla and, in many cases, repeated surgical procedures. Skoog recognized the potential that repeated, wide subperiosteal maxillary dissection could threaten the viability of facial growth centers in developing infants. When he evaluated his patients’ maxillary growth at age 5 years by comparing dental models with those of patients with clefts who did not undergo GPP, he detected no facial growth disturbance.10 However, continuing concern for iatrogenic growth disturbance during pubertal growth and the viability of the large mucoperiosteal flaps led others to analyze and question the Skoog technique. In 1972 Ritsilä et al11 reported the use of free tibial periosteal grafts to achieve the formation of a bony bridge across an alveolar cleft. Seventeen years later, in 1989, Rintala and Ranta compared long-term results of this free grafting technique with the previously reported Skoog technique.12 Over 6 years, they had treated 67 patients with Skoog’s maxillary periosteal flap technique and 23 with free periosteal grafts. Analyzing both groups using occlusal radiographs taken between ages 12 and 17, they reported bony formation in 64% of the clefts treated with the Skoog technique and in 85% of those treated with the tibial periosteum graft technique. Secondary bone grafts, however, were required in 72% and 73% of each group, respectively. Using cephalometric analysis, they did not detect a deficiency in facial growth, but they did report a lateral crossbite in all patients. Their analysis led the surgeons to abandon the technique of early GPP using the Skoog technique. They summarized that secondary bone grafting was not prevented in almost three quarters of the patients, maxillary collapse still occurred, adolescent orthodontics was not facilitated, and maxillary growth was not improved. They were also concerned that any GPP technique would prolong the initial surgery and create more scar tissue and the potential for secondary problems. They concluded that “… the more conservative and less scar-producing the early primary repair is, the lesser is the secondary growth retardation.” A similar finding with the Skoog technique was reported by Renkielska et al.13 They used the Goslon yardstick to evaluate occlusion after GPP and found 50% of patients treated with Skoog’s GPP technique had Goslon scores of 4 or 5, which indicate the need for orthognathic surgery.14 About the same time as Rintala and Ranta’s criticism of the Skoog technique, the next evolution of GPP was taking place as presurgical orthopedics became popular in cleft care. Aligning the alveolar segments preoperatively reduced the width of the cleft and facilitated the closure of the lip and alveolus. The major criticism of the Skoog technique had been that the degree of dissection and the size of mucoperiosteal flaps necessary to achieve closure of the unmolded alveolar cleft were not optimal for bone formation and unnecessarily increased the risk of growth restriction. With approximation of the alveolar edges using presurgical orthopedics, less subperiosteal dissection was needed to achieve closure of the cleft, which would presumably increase the viability of the mucoperiosteal flaps and decrease the risk for facial growth restriction. In 1974 Georgiade and Latham introduced an intraoral appliance for preoperative alignment of the alveolar segments.15 Millard began to use this device in Miami as part of his treatment protocol for patients with clefts.16 His presurgical orthopedics, periosteoplasty, and lip adhesion (POPLA) approach involved presurgical orthopedics with the Latham device followed by lip adhesion and GPP at 3 to 4 months of age. The Millard GPP involved elevation of gingivoperiosteal flaps from the interior of the alveolar cleft, with no dissection over the face of the maxilla. In 1999, Millard et al17 reported good bone formation on dental radiographs but also found a higher rate of anterior-posterior crossbite in patients treated with this technique. They analyzed occlusal casts of 63 patients treated with the POPLA technique and compared them with those of 61 patients who had been treated with their previous conservative technique of lip adhesion alone. Facial growth did not seem to be affected, but the authors admitted that repeat evaluation at skeletal maturity would be needed for definitive conclusions.17 Critics of the POPLA technique included Berkowitz, the original orthodontist who worked with Latham and Millard, as well as others with access to the Miami records. Henkel and Gundlach18 analyzed occlusal casts and lateral cephalograms of 146 patients treated by Millard with either the POPLA or a conservative technique. They reported worse crossbite in patients treated with the Latham device and GPP. Moreover, they found vertical growth disturbance of the maxilla in 42% of patients with unilateral clefts and 40% of patients with bilateral clefts treated with Millard’s technique.18 Berkowitz et al19 analyzed the occlusion of these patients in a subsequent paper and found anterior and lateral crossbites in 100% of patients treated with GPP. His prime concern was that the crossbites were more difficult to correct orthodontically in patients treated with Millard’s POPLA technique. He felt that “in most cases, LeFort I surgery or maxillary advancement with distraction osteogenesis is necessary.”19 More recently, Matic and Power20 also reported decreased maxillary anteroposterior development and height at an average of 14.7 years when GPP was performed after alveolar molding with the Latham device (without lip adhesion) in patients with unilateral clefts, regardless of palatoplasty technique. More than 90% of these patients required subsequent bone grafting.21 The results were even more unfavorable in patients with bilateral clefts undergoing such treatment.22 The most recent evolution of GPP has developed to address the potential negative effect of the Latham device on dentofacial growth by using it in combination with nasoalveolar molding (NAM) as described by Grayson et al.23 This is the technique I (R.A.H.) currently use. Unlike the POPLA technique described by Millard, the NAM-GPP differs not in the technical surgical details of the GPP but in the method of presurgical molding of the alveolar segments in preparation for the GPP and the criteria for selecting appropriate candidates. Unlike the Latham device, which actively molds the alveolar segments, NAM is a passive process that directs the rapid growth of the alveolar segments during the initial months of an infant’s life (see Chapter 64). From the perspective of GPP success—bony union without impaired facial growth—advocates of the passive molding process of NAM believe it to be a more accurate means of molding the leading edges of the alveolar cleft to optimize flap design and osteogenesis while being less invasive and compressive to the growth centers of the immature face. The history and evolution of GPP from Skoog, to Rintala, to Millard, teaches us that it can take 15 to 20 years before the risks and benefits of a surgical technique to address a cleft can be fully appreciated. As the NAM-GPP technique is practiced by more centers and as more long-term outcomes become available, it will undergo objective external critical evaluation to find its appropriate place in the arsenal of cleft surgical care. Prerequisites for GPP are an informed consenting family, appropriate cleft anatomy to allow alveolar bony approximation, an optimally molded alveolar cleft, intact mucosa, and no dental eruption. GPP can be scheduled at the time of the primary lip repair for patients who meet these criteria. Before GPP, the patient must be evaluated by the practitioner coordinating the NAM and the surgeon who will be performing the GPP. The patient’s guardians should be introduced to the concept of a GPP, the risks and benefits reported in earlier GPP techniques, and the current data on NAM-GPP before NAM begins. Not all infants are candidates for NAM because of individual compliance; likewise, not all infants are candidates for GPP because of individual variations of anatomy. Some infants with particularly wide unilateral clefts can be mesenchymal deficient: Alveolar arch anatomy would unnaturally constrict the arch form were the segments to be presurgically approximated. The NAM team should identify these patients early in the process so that the parents can be notified that a GPP will likely not be possible. Isolated clefts of the primary palate make it difficult to predict whether a GPP is possible. Because of the bony fusion of the secondary palate, the alveolar segments of the primary palate are more resistant to presurgical molding and, in many cases, cannot be adequately aligned for a successful GPP. In bilateral complete clefts, aligning both sides of the premaxilla with the lateral alveolar segments is not always possible. In these cases, one alveolar cleft can undergo a GPP to convert the arch form to a lesser and greater segment similar to a complete unilateral cleft. Although the contralateral cleft will need to be secondarily grafted, the premaxilla will be stabilized by the GPP to facilitate incisor mastication during early childhood; as well, the increased morbidity and failure associated with bilateral secondary bone grafting may be avoided. During the NAM process, the critical assessment of alveolar ridge alignment and parallel alveolar molding is subjective and benefits from a team presurgical evaluation. The optimal alignment of the alveolar segments is based on the underlying bone, not on the visible gingival mucosa (Fig. 68-1). In some cases the gingival tissue can be hypertrophied in the area of the cleft, mimicking close approximation and alignment of the cleft, but the underlying bone gap is misaligned and wide. In other cases, the alveolar cleft is compressed, but the bony arch forms are not in alignment, with the lesser segment posterior to the greater (Fig. 68-2) or the premaxilla wedged anterior to collapsed lesser segments. If a GPP is performed in these situations, the mucoperiosteal tunnel between the exposed bone edges will be “kinked” and create a soft tissue barrier instead of guided tissue regeneration.
Gingivoperiosteoplasty
Richard A. Hopper, Faisal Al-Mufarrej
KEY POINTS
GUIDED TISSUE REGENERATION
BACKGROUND
Skoog’s Technique
Rintala and Ranta Experience
Presurgical Orthopedics, Periosteoplasty, and Lip Adhesion Approach
Evolution of Nasoalveolar Molding and Gingivoperiosteoplasty
PATIENT SELECTION AND EVALUATION
PREOPERATIVE MANAGEMENT WITH NASOALVEOLAR MOLDING
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine