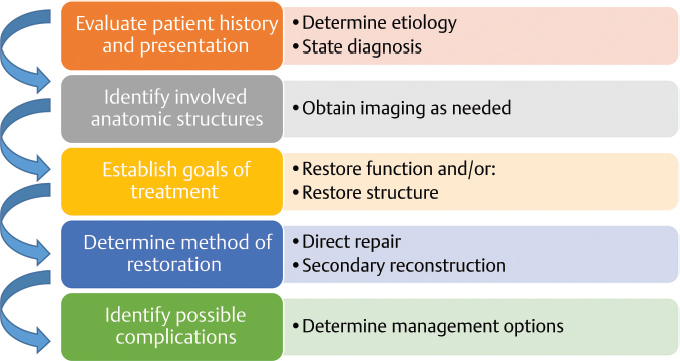
1 General Approach to the Oral Board Examination Abstract This chapter will provide an overview of the examination process, and an algorithm for a general approach to cases. It will also provide strategies for addressing un familiar cases, and for redirecting one’s answers when one makes an error during the examination. Keywords: plastic surgery, plastic surgery oral board examination Six Key Points • Approach difficult and unfamiliar cases with a stepwise approach. • Generate differential diagnoses. • Always clearly state the diagnosis. • Identify key points of diagnosis and management to communicate. • Rehearse answers for when you get stuck. • Plan and rehearse the flow of your answers for both straightforward and complex cases. The oral board examination is the final step in becoming a board-certified plastic surgeon. A knowledge base is essential, but a deficient knowledge base is not the only reason one may not be successful on the oral board examination. This book is designed to help you organize your knowledge to communicate it succinctly; it is a book about application of knowledge rather than mastery of knowledge. The first person is used in the answers, because in the oral board exam, as in practice, the answer to management questions is not what someone else would do, but what you would do. Many plastic surgeons who are not successful in passing the oral board examination are not deficient in their knowledge. They struggle, however, with recalling the information in a practical way. It is a helpful exercise to distill how the questions on the oral board examination may be asked, and they are, in the most general terms, as follows: (1) did you make the diagnosis correctly, (2) what are you going to do, (3) The algorithmic approach is useful for all to do it, and (4) what is your plan B when your plan A fails ? Many textbooks focus on pictures, specific cases, and core knowledge. These are necessary but not sufficient components of your preparation. Part of your study strategy should be to be able to communicate your answers to the above four questions for any given diagnosis quickly and without relying on pictures. You should be able to take a cue word (e.g., aesthetic face or breast reconstruction) and discuss diagnostic considerations and treatment strategies, as well as management of complications. This book is structured to help you do that. The stepwise approach is useful for all cases, but its utility becomes clear in the unfamiliar case. It provides a general structure to organize your thought process, and helps ensure you will not overlook significant findings. Most often, difficult cases are collections of smaller, manageable cases. Fig. 1.1 provides a general approach to the difficult case. Fig. 1.1 The stepwise approach to a case. These steps should be the anchors of diagnosis and decision-making. 1. The patient history and presentation is evaluated. A preliminary differential diagnosis is made. The etiology of the condition must be determined. The VINDICATE(M) mnemonic for the universal differential diagnosis can be helpful: Vascular, Infectious/Inflammatory, Neoplastic, Drugs/Degenerative, Iatrogenic/Idiopathic, Congenital, Autoimmune/Allergic, Trauma, Endocrine, (Metabolic). 2. If the etiology is unknown, one must determine the etiology of the condition. For example, suppose the case is a facial lesion in an adult. The etiology could be ectatic vessels (vascular), an injury (trauma), or it could be a squamous cell carcinoma or basal cell carcinoma (neoplastic.) You would determine the etiology by obtaining a tissue diagnosis. In the case of male gynecomastia, etiologies could be endocrine, idiopathic, or drugs. One would work up the patient to exclude endocrine abnormalities prior to intervention. Once the etiology has been identified, it is important to state the diagnosis explicitly. 3. Once the etiology is identified, one determines the involved anatomic structures. 4. After the diagnosis has been made and the involved anatomic structures have been identified, one establishes the goals of treatment. Goals of treatment are, in general, to restore function and to restore structure. Once the functional goals are identified, they should be prioritized and triaged to likelihood of success. For example, an elderly patient with severe carpal tunnel syndrome manifested by night pain, constant numbness, and thenar atrophy may have identified goals of pain reduction and improvement in sensation, as well as improved muscle function. The goal of night pain reduction can be achieved with a carpal tunnel release. The numbness may persist despite operative release. To restore function, one might consider a tendon transfer. In some cases, surgical intervention is not required to achieve the goals. 5. Once the functional goals are identified, one assesses whether there are structures that need to be restored. This is most apparent in trauma and tumor resection. Structural considerations are best approached with the what is present and what is missing, what is missing and needs to be replaced, and what cannot be replaced? model. 6. Finally, once one has an operative and nonoperative plan, one identifies potential complications. An important skill not only for the oral board examination, but also for general practice is being able to respond honestly and humbly while still projecting confidence and communicating your knowledge and content expertise. Planning how you will respond when you misspeak—and you will—helps make your answers concise, and helps avoid disorganized responses (Fig. 1.2). The ability to make a diagnosis is a key part of the oral board examination. Lead with your diagnosis. When describing radiographic imaging, the most succinct way of communicating the diagnosis is to use the formula as follows: “This [AP/PA/LATERAL/OBLIQUE/CORONAL/AXIAL/SAGITTAL] view of the [BODY PART] demonstrates [DIAGNOSIS].” Examples include the following: • “This posteroanterior radiograph of the right hand demonstrates a boxer’s fracture of the small finger metacarpal.” • “This coronal cut of a facial bone CT scan demonstrates a displaced right subcondylar mandibular fracture.”
General Approach
Addressing Unfamiliar and Difficult Cases
Annotated Steps
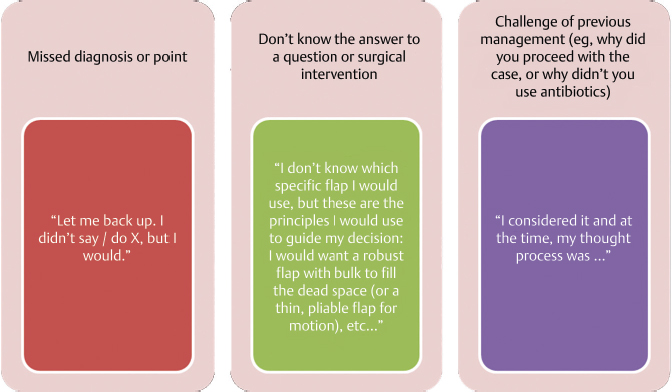
Redirecting One’s Answers
Describing the Diagnosis
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine