Summary
Full-thickness skin grafting constitutes a large percentage of procedures for head and neck reconstruction.
For color-matched grafts, skin must be harvested from above the clavicles; there are few indications to not use color-matched full-thickness skin grafts in head and neck reconstruction.
Full-thickness skin grafting can be used in both upper two-thirds and lower one-third nasal reconstruction, provided careful selection guidelines are followed.
5.1 Algorithm
5.1.1 General Considerations
In many ways, color-matched full-thickness skin grafting is an ideal reconstructive modality for head and neck soft-tissue defects (▶ Fig. 5.1). For suitable patients, it is simple and reliable, and the majority can be performed under local or IV (intravenous) sedation anesthesia. From an oncologic standpoint skin grafting does not disturb venous or lymphatic outflow and allows easy postoperative surveillance for cancer recurrence. The absolute contraindications are few including exposed bone and an unsuitable recipient bed. Commonly mentioned contraindications of active smoking, current anticoagulation, and the requirement for postoperative radiation are in fact not true contraindications. For over a decade, University of Texas Southwestern Medical Center (UTSWMC) has been treating active smokers, fully anticoagulated patients, and patients requiring postoperative radiation with little difference in clinical outcomes.
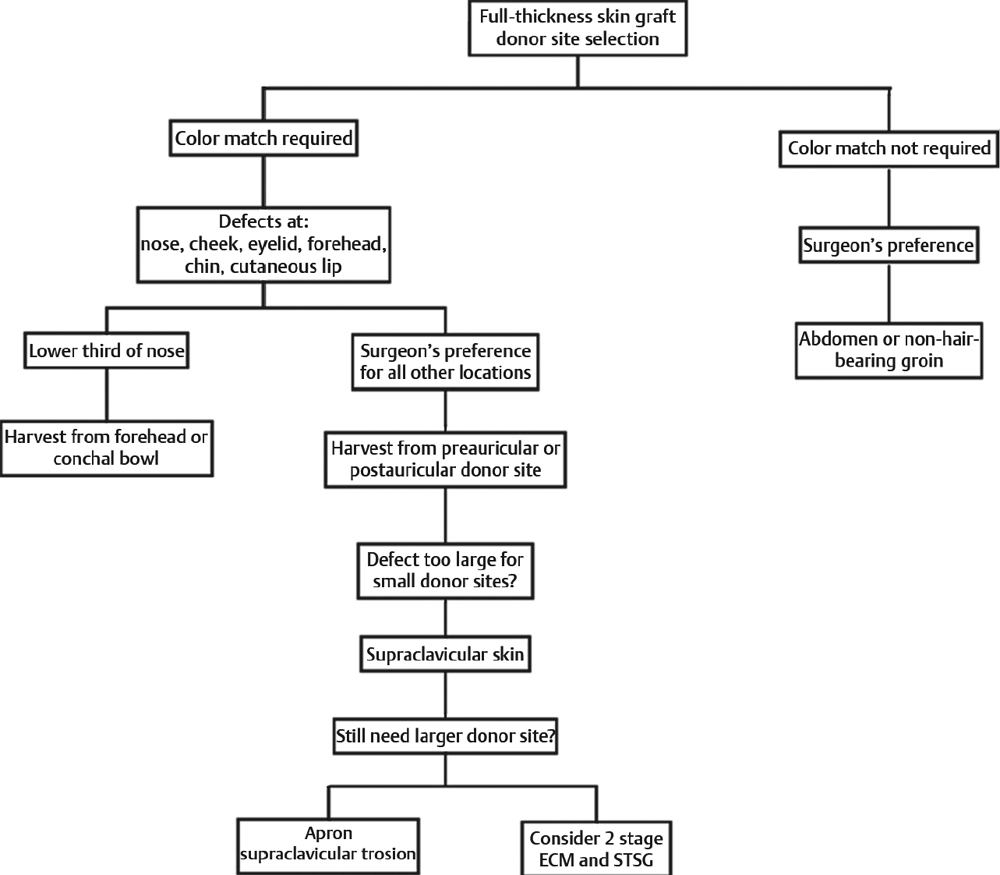
Fig. 5.1 Algorithm for appropriate donor site decision.
5.2 Selection of Donor Site
The selection of donor site for full-thickness grafting from the head and neck is mandated by the need or indications of color-matched result given there can be no color match on skin grafts harvested below the clavicle. 1 The other considerations regarding donor site include surgeon preference, as well as the size and thickness of the graft.
Color-matched skin grafting is harvested only above the clavicle and in the rare instance that the surgeon is performing skin grafting for head and neck defects where color-matched skin is not required it involves such large defects where a supraclavicular incision is not allowable or in patients where large posterior scalp defects or postauricular defects can be full-thickness grafting without consideration of color match. However, for large defects on the visible portions of the head and neck that are too large for full-thickness grafting, these can be treated initially with extracellular matrix (ECM) followed by split-thickness grafts harvested from the posterior scalp to achieve equivalence of full-thickness skin graft (FTSG) coverage. 2
For color-matched requirements, the decision regarding donor site is often surgeon preference. Although the most often cited, the postauricular donor site is not always an ideal donor site. Postauricular skin color match is not ideal given it is often not a sun-exposed area. The laxity behind the ear is not great and the skin is frequently very thin. During the skin graft harvest itself, an assistant is required to retract the ear and frequently the area can be contaminated by movement of the patient’s head onto a nonsterile drape. The one clear advantage of postauricular donor site is that there are no donor site scars on the patient’s face. The vast majority of full-thickness grafts done at UTSMC are from a preauricular incision, particularly on elderly patients. A posterior crease is easily found, the skin is slightly thicker, the color match is ideal, and the actual harvest of the graft is easier for a single surgeon to do without requiring the ear to be held out of the way. The chance of contamination during prep and harvest is much lower and the quality and quantity of the skin is superior to a postauricular donor site. The preference is for a planned dog-ear excision to be included in the relaxed skin tension lines. No undermining is performed. The defect is closed with single 3–0 Vicryl suture, followed by subcuticular Monocryl and Dermabond or Steri-Strips. This renders a donor site that is very easily cared for and heals without issue or significant scar.
For the special graft requirements of lower third nasal defects, the ideal skin type is from the forehead. 3, 4, 5 The color match and thickness are ideal. 5 However, the size of the graft is limited, and despite best efforts at closure, the donor site is visible. 5
For patients that do not require a thick graft for lower third nasal defects, conchal bowl skin is also an excellent option. 6 Conchal bowl skin has matching color and pore size to the skin of the nasal ala and tip, and the entire conchal bowl can be harvested.6, 7 The skin is excised through an anterior incision and the defect is allowed simply to heal secondarily or with placement of ECM and within 3 to 5 weeks it will heal completely with an essentially invisible donor site scar.7, 8
For defects too large to harvest, forehead, preauricular, or postauricular skin can be taken in significant quantities, particularly on the aging neck. The incisions are placed in relaxed skin tension lines and for larger skin requirements an apron-type incision can be made across the midline neck that will provide larger pieces of skin, although a seam within the final graft will be required. For all donor sites, meticulous attention at closure is made, particularly with regard to hemostasis.
5.3 Graft Elevation and Inset
Proper skin graft inset starts prior to graft harvest with careful attention to measuring accurate graft size. The size of the graft based on subunit or defect is largely based on a foil pattern template that is transposed from the defect to the donor site. The planned dog-ear incisions are marked out on the neck and then a no. 69 beaver blade is utilized to score the outline of the graft only. It should be understood that the neck donor site, as well as the preauricular cheek donor site, needs to be placed on stretch prior to graft design and graft harvest. If this is not done, the harvested graft will be greatly oversized and can impair graft take. Additionally, time spent now with appropriate graft sizing will result in a much faster inset procedure because no decision needs to be made during inset given there is assurance that the graft is of the correct size.
As the graft is elevated, no attempt is made to thin the graft; rather after the graft has been sharply elevated, it is left attached on one limb and then can be thinned with sharp facelift scissors to the deep dermal layer safely. When the graft is separated, it is still handled only by the soon-to-be-discarded dog-ears and these are excised and the graft is placed in the prepared wound bed. At this point, it is understood that it is unnecessary to place tacking sutures to determine the graft dimensions. The graft is the correct size because the appropriate size template was used prior to graft harvest. For smaller grafts (less than 1 cm), tacking sutures of 5–0 fast-absorbing gut are utilized in a clock face pattern to secure the graft; if the graft is larger than 1 cm, then two opposing sutures of 5–0 plain gut or fast-absorbing gut are utilized to sequentially inset it and then at the end they are both tied to each other 180 degrees opposite to the start. This results in the fastest inset possible without unnecessary “fussing” and manipulation of the graft during the inset.
5.3.1 Bolstering the Graft
Great attention needs to be paid after graft inset to bolster preparation. 9, 10
Although there are many descriptions of bolsters, the most commonly cited is a cotton ball wrapped in Xeroform. In many ways, this is an unsatisfactory bolster. It requires the opening of multiple surgical products and has no inherent stretch or give. If not properly cared for postoperatively, it will dry and can stick to and dislodge the graft on bolster removal. A much-improved bolster is a simple dry surgical sponge that is included in the prep set. 10 It is easily cut to size and vigorously coated on one side only with antibiotic ointment, and this can be simply sewn in with through-and-through 3–0 proline central bolster suture, as well as with interrupted 4–0 Nurolon pop off suture for the scalp or 5–0 silk for lesions on the face. No attempt is made to tie over sutures as the sponge itself has adequate resilience to hold the centripetally placed stitches.
5.3.2 Postoperative Care
The patient is allowed to shower the second postoperative day with a sponge in place provided he or she liberally coats it with ointment prior. The only activity restriction put on the patient at this point is against heavy lifting. From day 1, we allow them to cycle, run, sweat, and resume their daily activities; we, however, prefer that they do not swim or lift heavy objects. The sutures are removed on the fifth or sixth postoperative day and the patient is changed from antibiotic ointment to plain Vaseline for the duration of healing. On bolster removal at day 5 or 6, even a properly healing FTSG will go through a number of color changes that can be disconcerting to a beginning surgeon, as well as most patients. Even early discolored skin grafts can pink up and go on to near-normal healing. No matter the graft appearance, great care is put into postoperative care until the final determination of the graft outcome is made (▶ Fig. 5.2, ▶ Fig. 5.3, ▶ Fig. 5.4, ▶ Fig. 5.5, ▶ Fig. 5.6, ▶ Fig. 5.7, ▶ Fig. 5.8, ▶ Fig. 5.9).

Fig. 5.2 A 52-year-old female status post Mohs resection of basal cell carcinoma presenting with combined cheek and nasal defect. The majority of the defect is nasal sidewall.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


