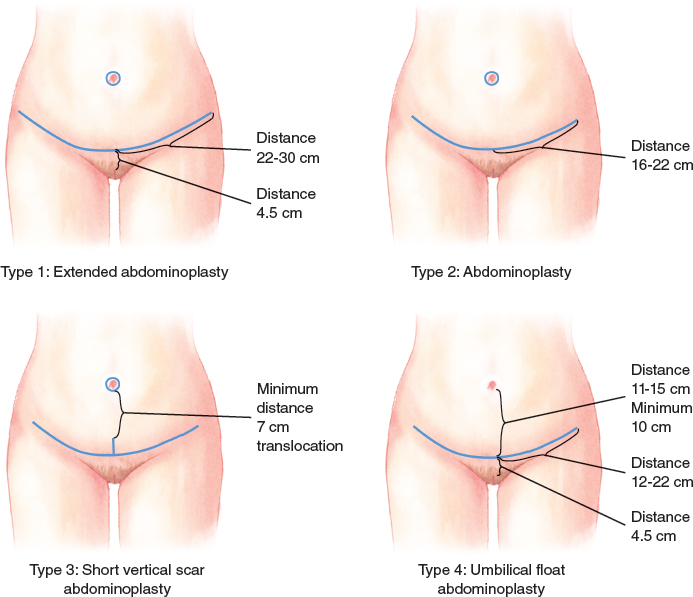
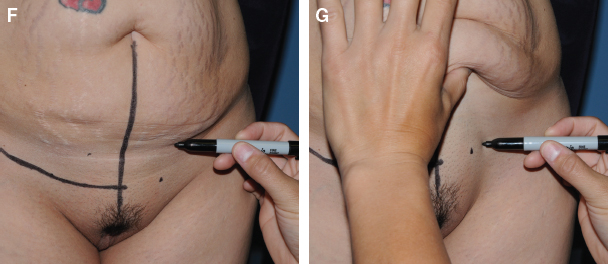
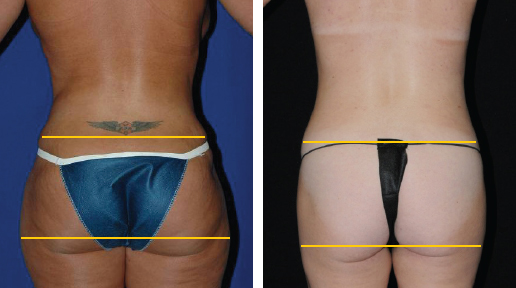
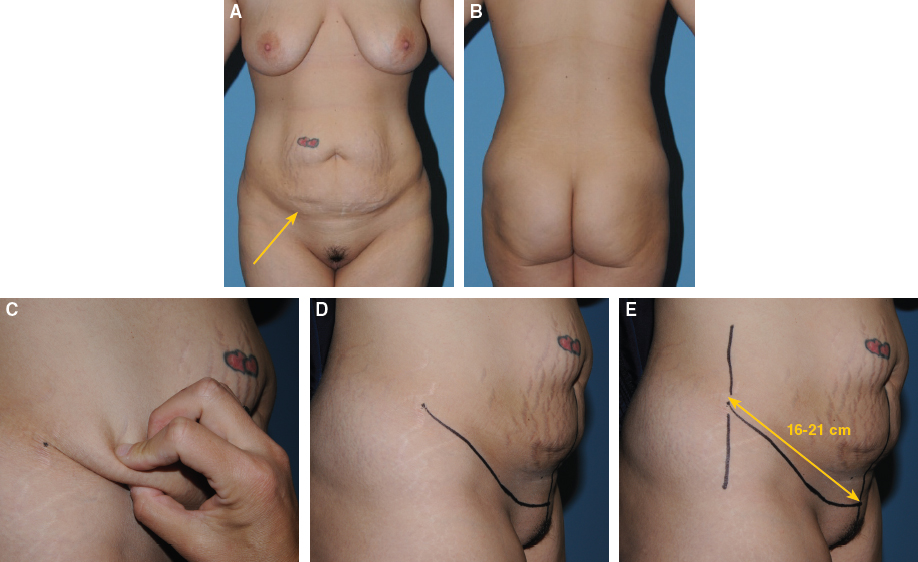
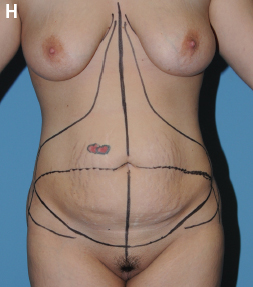
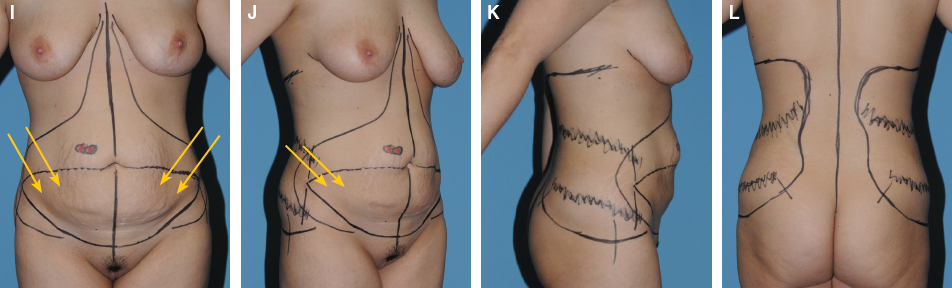
CHAPTER 6 Simeon Wall, Jr. There may be other surgeons, such as the senior author (S.W.), who have answered this question by developing their own successful approach. In particular, the work of Dr. Joseph Hunstad was a significant catalyst in furthering the premise that circumferential liposuction can indeed be performed safely and effectively with full abdominoplasty. We think that when indicated, comprehensive and circumferential liposuction concurrent with full abdominoplasty not only is safe and in the best interest of the patient, but also there is little doubt that it can provide results far superior to either liposuction or abdominoplasty alone or staged. The caveat with this statement is that not all methods of liposuction and abdominoplasty are equal, equivalent, or appropriately combined. In this chapter we present our pathway and techniques for creating dramatic, effective, comprehensive, and safe truncal contouring that fully treat the excess skin, abdominal wall laxity, and adiposity of the circumferential trunk. A common yet diminishing perception of performing liposuction with abdominoplasty has been that circumferential and/or comprehensive liposuction can diminish flap circulation and viability. The SAFELipo liposuction process, as described (see Chapter 15), does not damage the vascular supply of the flap, allowing full and safe use of the flap in abdominoplasty procedures. We have not had a single instance of significant flap necrosis in more than 1000 consecutive primary cases to date at our center. Three patients had minor flap necrosis; all three had undergone multiple abdominal surgeries previously, and two of them also had a history of multiple abdominal mesotherapy treatments. The addition of comprehensive SAFELipo and excising the subscarpal fat of the entire flap actually diminishes the risk of complications by decreasing the metabolic demands of the flap, effectively enhancing flap circulation. A thin, well-perfused, metabolically unloaded flap resists infection and ultimately heals better than a thick, fat-burdened flap with high metabolic demand. It is acknowledged that any abdominoplasty technique, including the one described here, can result in some degree of flap necrosis because of the variability in individual patient anatomy and conditions, previous surgeries or treatments, unknown or undiagnosable medical problems, and the like. Knowing that no surgery is risk free, our goal as practicing plastic surgeons is to offer what we think is the best solution with the lowest reasonable risk for the patient. The SAFELipo process allows comprehensive liposuction that does not damage flap blood supply, and can be easily taught to and reproduced by other surgeons. This three-step process can be used with all excisional procedures safely and effectively. The techniques are designed to minimize vascular injury and contour deformities, while maximizing fat removal and skin viability. The fat separation performed in the SAFELipo process is accomplished without suction by using specialized cannulas or probes that prevent suction-avulsion injuries to blood vessels. The blood vessels remain intact, while free separated fat is preferentially aspirated with smaller-diameter cannulas. Final contouring is maximized by performing fat equalization as a final step after aspiration, resulting in dramatic contouring of the area, tremendous skin retraction, and minimal risk of contour deformities or skin injury. Component anatomy of the abdominal wall and truncal soft tissue has been well documented. In an unoperated abdomen, the area of the flap is normally supplied by rectus abdominis perforator vessels. After the surgeon elevates the flap and removes the pannus, the blood supply to the abdominoplasty flap is predominantly from secondary sources, including deep subcostal and intercostal perforators that have already supplied the superolateral trunk and passed through watershed zones to supply the flap. Therefore most of the blood supply to the flap flows from superficial to deep, with the exception of the contributions from any preserved rectus abdominis lateral row perforators. Consequently, the subscarpal fat of the flap is the last tissue to be supplied by these sources—acting parasitically on the blood supply. Excision of the subscarpal fat from the undermined area decreases the oxygen demand of the flap, essentially unloading the metabolic needs of the flap. Brink showed the safety and efficacy of subscarpal fat resection in abdominoplasty, and others have shown excellent results while maintaining excellent flap viability with a prescarpal flap dissection. ■ Zone I: The continuously undermined area of the final abdominoplasty flap extends inferiorly in a triangular fashion from the xiphoid inferolaterally to preserve the first three to five lateral perforators, and further inferolaterally and around the inferior portion of the flap. Extensive fat separation is undertaken just deep to the Scarpa fascia in this zone to facilitate quick and easy excision of all the subscarpal fat in this zone during the abdominoplasty. In addition, SAFELipo may be performed superficially in this zone, depending on the patient’s abdominal fat thickness and the desired results. Care must be taken to avoid treatment in the most superficial aspect of the superficial abdominal fat compartment to avoid devascularizing or damaging the subdermal plexus, which is the dominant blood supply of the most distal aspects of the abdominoplasty flap. ■ Zone II: The discontinuously undermined area of the thoracoabdominal area lateral to the flap—extending superiorly over the anterior aspect of the rib cage to the inframammary fold, laterally to the anterior axillary line, and inferiorly to beyond the lateral edge of the abdominoplasty incision. This zone is treated with extensive SAFELipo. ■ Zone III: The remaining circumferential trunk—anteriorly to include the mons pubis and anterior thighs, extending around the trunk to the back, limited superiorly by the inferior aspect of the axilla and the lower aspect of the scapula, and limited inferiorly by the lowermost aspect of the hip mound and sacrum. This zone is treated with extensive SAFELipo. ■ Zone IV: The abdominal pannus, to be excised. This area is treated with extensive SAFELipo only if additional fat is needed to complete a concurrent fat grafting procedure; otherwise, it is discarded. Ideal candidates for a comprehensive approach to circumferential contouring of the trunk are healthy, normal-weight men and women with some degree of three key components: (1) excess skin of the abdominal region, (2) diastasis recti, and (3) excess truncal fat. All three of these components are usually addressed fully to maximize improvement; most of the variability in the procedure involves the pattern of skin resection and resultant scars. The diastasis repair and removal of excess fat are usually only varied in their degree, not in their technical execution, which simplifies the overall approach while maintaining nearly universal applicability. Fig. 6-1 Zone I: Undermined area of the flap All zones except zone IV are treated with SAFELipo, with treatment of zone I limited to fat separation just deep to Scarpa fascia as well as superficial SAFELipo, if indicated, depending on the desired fat reduction and thickness of this zone. As with most aesthetic surgery procedures, patients who are of normal weight or who are only slightly overweight are the best candidates for comprehensive truncal contouring. Certain presenting body characteristics will uniformly allow more dramatic results, whether the patient is of normal weight or not. In an overweight patient with favorable skeletal anatomy and excess fat in “all the right places,” the limitations of surgery are less about concern for the final result and more about the higher risk of operating on an overweight patient. Almost universally, patients with high concentrations of subcutaneous fat in the circumferential trunk (abdomen, flanks, hips, and back) will obtain more dramatic results than those with more evenly distributed fat or minimal excess fat. This is not to say that all individuals with apple-shaped bodies are excellent candidates for this procedure. To the contrary, the more that a patient’s truncal excess is caused by his or her intraabdominal fat content rather than excess subcutaneous fat, the less effective any truncal contouring procedure will be, regardless of how well the skin, muscles, and fat are addressed. In practice, the best candidates for truncal contouring have a body mass index (BMI; weight in kilograms divided by height in meters squared) of less than 28, or are within 10% of their ideal body weight. For women, the ideal body weight is calculated by assessing height, with the first 5 feet counting for 100 pounds, and each successive inch adding 5 pounds to the total. Ten percent is added to the total, for a benchmark weight that can be used to guide both appropriateness for surgery and expectations for final appearance (example of a 5 foot 6 inch woman, 130 pounds plus 13 pounds equals 143 pounds). A female patient who stands 5 feet 6 inches and weighs 190 pounds should not expect to look as visually attractive after surgery as the same woman undergoing surgery at 140 pounds, keeping in mind that she also cannot expect to lose 50 pounds from the surgery. Many candidates with BMIs between 28 and 30 can also benefit greatly from this procedure, depending on their specific body habitus, as outlined previously. In general, potential patients with a BMI more than 32 will not realize the full benefits of the limited amount of liposuction that can be performed safely with abdominoplasty, and diastasis repair does not produce enough change proportionally in their truncal girth to be of clinical significance. Both of these factors serve to limit the absolute or apparent reduction of the waistline, diminishing the dramatic change in body contour that this approach is designed to deliver. In these patients postponing any type of body contouring surgery may be more appropriate. We have found that less comprehensive approaches to truncal contouring, such as panniculectomy, simple abdominoplasty, or liposuction alone, are not appropriate or satisfying options for most patients seeking elective aesthetic surgery. Accordingly, we do not offer any surgery until a candidate can lose weight, rather than performing a procedure that cannot produce the changes with which either the surgeon or the patient will ultimately be happy. A variety of proven, safe, and lasting weight-loss options are made available to these patients for them to eventually become candidates for circumferential truncal contouring surgery as previously described. Patients who can benefit significantly from the skin resection and skin-tightening effects of circumferential SAFELipo are those with moderate weight loss, generally less than approximately 40% of their starting weight and less than 60 pounds, and who have significant abdominal skin laxity that extends posteriorly but is not so severe as to require a circumferential body-lift procedure. The amount of circumferential truncal skin tightening achieved through this procedure allows an anterior-only abdominoplasty approach in all patients except for patients with severe skin laxity that extends to other body areas. Massive-weight-loss patients will usually benefit more from a circumferential skin reduction procedure incorporating elevation of the buttocks and lower extremity skin, as originally described by Lockwood and later refined and improved by Aly, Capella, Rubin, and others. These techniques are described in detail elsewhere in this textbook and can easily be incorporated into an abdominoplasty/SAFELipo procedure to produce a harmonious circumferential improvement in the trunk and lower body. In any abdominoplasty procedure, the presence of an abdominal scar that cannot be removed with excision of the pannus may pose a serious risk to the vascularity of the abdominoplasty flap, depending on the length and location of the pannus and the extent of previous dissection. Scars such as these can be classified according to their impact on the surgeon’s ability to fully treat the patient’s excess skin, diastasis, and excess fat with the appropriate abdominoplasty procedure. Existing abdominal scars can be thought of as low-impact scars (such as short laparoscopic incisions), high-impact scars (such as long subcostal incisions, paramedian incisions, anterior-approach retroperitoneal incisions), and scars of variable impact, such as LAP-BAND incisions and umbilical hernia incisions. With scars of variable impact, the vascularity of the flap is subject to the extent of the dissection that was undertaken during the previous procedure, and should be carefully considered preoperatively. The patient’s previous operative reports (if available) should be reviewed to determine the presence of mesh and whether multiple surgeries were performed through the scar; this can provide valuable information regarding the risk that the scar has to the abdominoplasty flap. In the presence of a scar that is determined to be of high or indeterminate impact and that will remain in the flap, the surgeon should attempt to maintain as much vascular redundancy in the flap as is practical to minimize the effects of the previous vascular interruption from the scar. In this case a more conservative skin undermining is performed, usually limiting the continuous undermining to the area of diastasis repair, with conservative discontinuous undermining to minimize skin redundancy and irregularities, with care being taken not to dissect beyond the scar. As a result of the minimal impact on flap vascularity unique to the SAFELipo technique, circumferential liposuction of the trunk in these patients is unaltered. In certain patients with high-impact scars, it may not be prudent or appropriate to perform an abdominoplasty procedure; unique or alternative approaches such as midline, fleur-de-lis, or reverse abdominoplasty should be explored. Rarely, patients with high-impact scars may not be candidates for any form of a body contouring procedure that includes truncal skin resection. Patients with a history of mesotherapy or various forms of injection lipolysis of the abdomen and/or flanks may have a significant risk of vascular compromise to the abdominoplasty flap. These treatments have been shown to cause fibrosis of the superficial vascular network, the main blood supply to the abdominoplasty flap. Similarly, patients who have previously undergone disruptive and/or thermal methods of liposuction, such as laser-assisted liposuction of the trunk, may have a compromised blood supply as a result of coagulation of the treatment area and vascular fibrosis. Caution should be exercised when performing abdominoplasty in these patients, with or without associated liposuction. Other general contraindications to circumferential liposuction of the trunk with abdominoplasty are the same as those in any abdominoplasty procedure, including serious medical conditions and potential future pregnancy. Most women who request truncal contouring desire a more curvaceous and proportional outline of the waist and hip region. The surgical plan must give careful consideration to the ratio of the width from the hip to the lateral thigh, as described extensively by Mendieta. In addition to a patient’s anatomic limitations for waist reduction and proportionality, his or her excess fat, loose skin, and aponeurotic laxity must be given due consideration as the surgeon determines the best procedure for that patient. First, one considers the amount of excess subcutaneous fat of the circumferential trunk to be treated by SAFELipo. Although visual inspection is essential, tactile evaluation of skin pinch thickness throughout the various zones of the trunk is the most important assessment tool in determining areas to be treated. Skeletal and muscular anatomy dictate to a large degree the surgeon’s ability to change the truncal shape and outline. However, unlike simple abdominoplasty procedures, the addition of circumferential SAFELipo dramatically increases the total amount of change that can be produced in most patients. Use of the SAFELipo technique allows maximal removal of excess fat without creating contour deformities or disrupting the vascular and stromal network that is commonly seen with standard and thermal forms of suction-assisted lipectomy. After determining fat excess of the desired treatment areas, skin excess and abdominal wall laxity are assessed. In contrast to the common practice of performing partial or incomplete diastasis recti repair in selected patients, we perform a full plication of the midline abdominal fascia, from the xiphoid to the pubis, in every patient. Additional aponeurotic repair away from the midline is rarely indicated, but undertaken when necessary. Generally, patients with more than a minimal amount of skin laxity (7 cm of skin laxity or more) will ultimately do better long term with an abdominoplasty as opposed to liposuction alone; therefore the first choice of procedure in patients with any degree of diastasis who are not planning any future pregnancies is to include abdominoplasty with circumferential liposuction. Regardless of how well a liposuctiononly procedure is performed, or how thin the abdominal skin can be contoured, the longer-term problem with abdominal contouring is that the abdominal area is one large flexion crease. Unless the abdominal skin is completely tight, there always appears to be “excess” skin with any abdominal flexion. The presence of these skin “rolls”, frequently with an accompanying bulging abdominal wall, will remain a problem for most patients, and will frequently require additional surgery later. With time and experience, we have moved away from performing abdominoplasty only when absolutely necessary to complement circumferential SAFELipo, and have embraced performing an abdominoplasty if at all possible. Correction of skin, muscle, and excess fat is far superior to treating excess fat alone. Additionally, controlling the skin contour of the abdomen with excision allows more thorough fat contouring without the worry of creating the flexion crease deformities sometimes seen with thorough liposuction alone. To that end, the evaluation of a patient with any degree of abdominal skin laxity should be geared toward performing the most complete correction of the laxity. Often the most challenging aspect of patient evaluation is determining whether there is enough skin laxity for an abdominoplasty procedure, and further, what type of skin resection pattern the skin laxity will allow. The challenge is in the ability and desire to transpose the umbilical skin to bring about maximal skin tightening of the upper abdomen, while also maintaining a very low position of the final abdominoplasty scar. We recommend always maintaining a very low scar position, thereby making the skin resection pattern fall into one of the general categories, depending on whether the umbilical skin is transposed or not, and if so, whether the umbilical skin defect is excised completely. In practice, patients can be categorized preoperatively into one of four abdominoplasty types based on the resultant scar: extended abdominoplasty (type 1), abdominoplasty (type 2), short vertical scar abdominoplasty (type 3), or umbilical float abdominoplasty (type 4). In types 1 and 2, the umbilical skin is transposed completely, and the resultant scar remains low and transverse. In type 3, skin is transposed incompletely, and the resultant scar may include a short vertical component (inverted-T incision) of up to a few centimeters, in addition to the low transverse scar. In type 4, the umbilical skin is not transposed, and the umbilicus has usually “floated” 1 to 4 cm, leaving only a low, shortened transverse scar. A thorough and comprehensive medical history and physical examination is performed, with careful consideration given to previous surgeries, medical conditions, and ingested substances. Any and all prescribed and nonprescribed medications, herbal supplements, and vitamins are reviewed to minimize the risk of adverse events with surgery, with particular emphasis placed on identifying and discontinuing substances that increase bleeding, impact healing, or are stimulants. Many of these substances should be discontinued several weeks before surgery if at all possible to minimize the risk of adverse events. Smoking or any other form of nicotine ingestion dramatically increases the risk of tissue necrosis and should be discontinued at least 4 weeks before surgery. The patient’s nicotine status is determined preoperatively by urine cotinine testing to exclude positive patients from surgery. A history of bleeding or clotting disorders in the patient or his or her family is evaluated fully, and a Caprini risk assessment is done. Patients with a high risk of venous thromboembolism (VTE) may not be acceptable candidates for an extensive body contouring procedure, to be determined on a case-by-case basis by the surgeon, patient, and any recommendations from specialists. The usual protocol is to obtain clearance for general anesthesia from the patient’s primary care physician and any indicated specialists 1 month before surgery, which will allow enough time for intervention or substitution to the operative schedule. Surgical packets with all of the preoperative, perioperative, and postoperative care instructions and information are sent to the patient when surgery is scheduled. Then the patient is called 2 weeks before surgery to answer any of his or her questions, verify compliance with the instructions, and remind the patient not to take any contraindicated substances such as aspirin, NSAIDs, stimulants, and so on. The results of appropriate labwork and any indicated tests are reviewed before surgery, usually at a preoperative appointment 1 or more days before surgery. A preoperative appointment facilitates a more thorough informed consent, gives the patient another opportunity to have questions answered, and gives the surgeon another opportunity to assess the patient and confirm the operative plan. Additionally, preoperative markings can be performed if the preoperative appointment is the day before surgery. The patient is asked to arrive 1 hour before surgery and is placed on a warmed bed that also functions as the operating table and recovery bed, and a forced air blanket is used on the bed. Warmed intravenous fluids are given, with a goal of administering 1 L of Ringer’s lactate before surgery. Sequential compression devices, either calf-high or foot-only, are placed and functioning when the patient is brought to the operative holding room. Preoperative medications are given, including intravenous antibiotics, famotidine (Pepcid), metoclopramide (Reglan), celecoxib (Celebrex), aprepitant (Emend), and clonidine. A multimodal antiemetic protocol is administered for all patients. While still in the preoperative holding room, the patient is marked in the standing position. The anterior midline is marked from the xiphoid process down to the anterior labial commissure. Using the top edge of the pubis as an underlying reference, the surgeon assesses the amount of mons pubis skin ptosis so that the final scar will be located centrally at the top edge of the pubis or lower. Fig. 6-3, A-E The lower abdominoplasty markings are made with the central point approximately 4.5 cm superior to the anterior labial commissure on full upward lifting of the skin (range of 4 to 7 cm), to elevate the ptotic mons pubis skin while allowing full pannus excision. In a typical abdominoplasty, the pannus will include all of the excess skin to above the level of the umbilicus. If all of this skin cannot be excised to allow closure, a small vertical closure will result. If a vertical closure is unavoidable, the lower markings are placed as low as possible to allow the final scar to lie over the top edge of the pubis. Continuing laterally from the mons pubis, the markings are made with strong superomedial traction on the skin, using the desired location of the scar as a reference point, as first described by Lockwood. The desired location is at, or just below, the top edge of the pubis centrally, and just above (1 or 2 cm) the groin creases laterally. In this manner the anterior thigh skin is lifted in concert with the mons pubis skin, allowing a far more comprehensive rejuvenation of the anterior trunk, groin, and anterior thighs compared with traditional abdominoplasty. Fig. 6-3, H The lower incision markings are continued laterally, with the lateralmost aspect of the markings turning upward for the final 3 cm, stopping where no skin will overhang with light downward traction on the anterior abdominal skin. The upturned ends (2 or 3 cm) of the markings are necessary when performing a medially advancing abdominoplasty closure such as this, to prevent downturned ends of the final scar location. If performed properly, the final scar runs parallel to the skin tension lines, in line with current low-cut swimwear bottoms and without a conspicuous upturn or downturn of the ends of the scar. At the lateral extent of the markings, a reference mark drawn straight inferiorly is made to maintain orientation of the skin on closure. The strong medial advancement of the abdominoplasty flap on closure can obscure the ends of the incision, and these reference marks help maintain proper orientation of the closure. Typically, the lower abdominoplasty incision markings are not adjusted intraoperatively. Fig. 6-3, I-L Markings for the planned upper incision line arc upward and medially to above the umbilicus, or higher, depending on skin laxity with skin pinch, with the patient standing, bent forward with relaxed abdominal muscles. The markings for the upper incision line are guides only, and are checked and verified intraoperatively with the patient in the flexed position at the time of closure, with full downward tension on the abdominoplasty flap, just before excision of the pannus. The costal margins and xiphoid are marked as general reference points. Excluding the pannus to be excised, areas of excess fat are targeted throughout the anterior abdomen, keeping in mind that all of the subscarpal fat of zone I will be directly excised. Often the excess fat of the anterior thighs is also marked. The most prominent areas of excess in the flanks are marked, with concentric circles leading out from the prominent areas. The midline of the back is marked. Areas of excess fat are identified by skin pinch, with the most prominent areas of the hips and any back rolls marked. Frequently there is midline lower back and sacral fat excess, which is also taken into consideration. The back marks are matched with the flank and abdominal markings, usually extending up to the inframammary folds and lower axillary areas in many patients. Obvious attention has been given to the shaping and contour of the circumferential trunk, but this does not occur in a vacuum. Thoughtful assessment of the entire silhouette should be undertaken, taking into account patient preferences, anatomic variations, and surgical limitations. Inclusion of buttock and thigh contouring is common in our practice and is typically focused on the interplay of the waist, hip, midbuttock, and lateral thigh. A direct comparison of the midface to the midbuttock has allowed for the application of our techniques to achieve the targeted volume redistribution and shaping that is needed to address the loss or absence of the ogee curve of the buttock. Specifically, the combination of SAFELipo, fat shifting, and targeted expansion vibration lipofilling (EVL) of the buttock can provide a high degree of shaping control that can neither be achieved through other described liposuction and fat grafting methods, nor be seen with the use of buttock implants. This approach has allowed for the incorporation of individual patient preferences into buttock and body shaping. These individual preferences are usually exhibited by their likes and dislikes of various ratios of many body landmark widths. Specifically, the waist-to-hip (WTH) ratio of 0.7 is widely acknowledged as having the most aesthetically pleasing appearance across age and ethnic differences in women. In our experience, and unlike the uniformity in preference seen in the WTH ratio, there is a wide variance in buttock shape preferences among women, most of which can be explained by ethnic preferences in what is generally considered the ideal body shape. The patient’s preferred hip-to-thigh (HTT) ratio is utilized extensively in planning for truncal and buttock shaping, and is also helpful in determining if a patient’s expectations can be met. Most black and Hispanic patients find 0.7 to be the most pleasing HTT ratio, whereas most Asian and white patients view a HTT ratio closer to 1 as ideal, with the caveat that the midlateral buttock appear full, resulting in a rounded buttock appearance.
Full Abdominoplasty With Circumferential Truncal SAFELipo and Subscarpal Fat Excision
 Michael R. Lee
Michael R. Lee
Surgical Anatomy and Physiologic Considerations
Indications and Contraindications
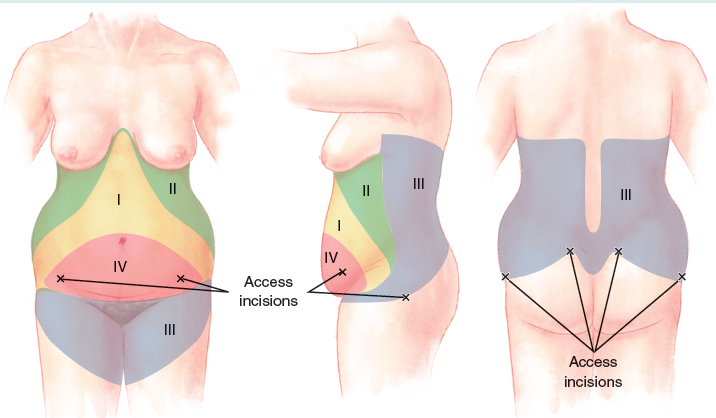
Zone II: Discontinuously undermined area superolateral to the flap
Zone III: Remaining circumferential trunk and anterior thighs
Zone IV: Abdominal pannus, to be discarded
FAT DISTRIBUTION
BODY MASS INDEX
SKIN LAXITY
EXISTING SCARS
EXISTING TISSUE INJURY
Patient Evaluation
FAT DISTRIBUTION
ABDOMINAL WALL AND SKIN LAXITY
Preoperative Planning and Preparation
Surgical Technique
MARKINGS
Abdominoplasty
Liposuction
ADDRESSING THE ENTIRE SILHOUETTE
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine