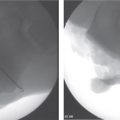
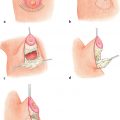
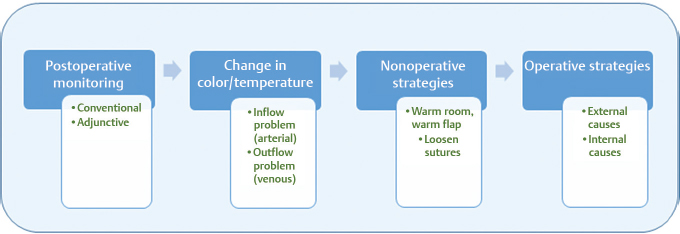
5 Free Flap Failure Abstract This chapter will review postoperative monitoring of the free flap patient and management of free flap failure. The reader will be able to discriminate between arterial and venous free flap failure, and explain operative and nonoperative interventions for free flap failure. Keywords: free flap failure, arterial compromise, venous compromise, free flap salvage, free flap monitoring Six Key Points • Postoperative monitoring should include conventional methods of color, turgor, and warmth. • Signs of failure are a purple flap or a white flap. • Conservative measures first. • Operative intervention to rule out extrinsic causes or intrinsic causes. • Heparinize ± thrombectomy for early clot, heparin/thrombectomy/thrombolytics for established clot. • Salvage options include second free flap, local flap, or delayed flap. All free flaps—whether in breast reconstruction, lower extremity reconstruction, or other reconstruction—have the potential for failure. The key is being able to identify cause quickly and have a management plan. A systematic approach will be outlined here. 1. What is your postoperative monitoring protocol? Flap checks should occur at prescribed intervals, such as every hour for 24 hours, then every 2 hours after that. Flap checks should include bedside assessment of color, temperature, turgor, capillary refill, and Doppler monitoring. Flap checks also include assessment of the signal from an implantable Doppler. Color is assessed by visual inspection, and a picture of the flap immediately after surgery can be hung at the bedside to allow comparison. The temperature can be measured from a skin paddle, and in some cases of buried flaps, a component may be externalized to allow monitoring. Temperature can be measured from palpation on physical examination, probes, and temperature tape. Capillary refill is described as either normal, brisk, or slow, and Doppler monitoring should be performed at the same spot, marked with a stitch (Fig. 5.1). Patients should also receive aspirin every day, and subcutaneous heparin 5,000 units twice daily. RATIONALE: Adjunctive techniques incl ude implantable Doppler systems, color duplex sonography, near-infrared spectroscopy, laser Doppler flowmetry (LDF), and microdialysis. Though expensive, adjunctive techniques identify free flap compromise earlier than conventional methods alone, and a review suggested that despite limitations of studies comparing methods, some adjunctive methods should be used. Implantable Doppler systems have the advantage of being the least expensive of these, and are strai ghtforward, which makes them useful for novices. Near-infrared spectroscopy was thought to be reliable with a 100% positive and negative predictive value, and is noninvasive, and was thought to be promising as an “ideal monitoring system.”1 Fig. 5.1 Postoperative monitoring and intervention algorithm of free flaps. 2. What are an implantable Doppler, color duplex sonography, near-infrared spectroscopy, LDF, and microdialysis? • Implantable Doppler: An implantable Doppler (or internal Doppler) is a device that wraps around a microvascu lar anastomosis, typically the vein because the vein is considered more rapid and accurate.2 Implantable Doppler systems, though accurate, can fail, and should not be the sole source of assessment of a flap. • Color Duplex Sonography: Color duplex sonography is a noninvasive monitoring technique that evaluates blood flow velocity and direction. It is not a continuous monitoring system, and provides information only at the time of analysis. Though accurate and precise, it requires an ultrasound technician and intimate knowledge of the flap anatomy, which may mean that both the microsurgeon and the ultrasonographer must be present for the evaluation. It is most often used for buried flaps. • Near-Infrared Spectroscopy: Near-infrared spectroscopy is a noninvasive technique that uses optical spectroscopy to measure oxygenated and deoxygenated hemoglobin through absorption spectra. The tissue penetration of the light has been reported to be up to 20 mm, and can be used for most flaps.3 • LDF is a noninvasive technique that uses coherent, collimated, monochromatic laser light transmitted through fiberoptic cables. The probe collects backscattered light, which fluctuates in intensity, and creates a function of low. The limitations of LDF are that one must follow trends rather than absolute readings, and it is very prone to artifacts, including positioning. • Microdialysis is an invasive technique in which a double-lumen catheter is placed in the tissues and dialysate is infused into the tissues; as it equilibrates with the extracellular matrix, it is sampled in microvials and analyzed for glucose, lactate, pyruvate, and glycerol. In arterial compromise, the glucose levels decrease and lactate: pyruvate ratio increases. Glycerol is a nonspecific sign of cell membrane damage and is seen in both arterial and venous compromise. While this has the advantage of identifying compromise before clinical signs appear, it only measures the tissue physiology at the sampling site.4 3. An implantable Doppler is not available. What do you do? If an implantable Doppler is not available, conventional methods are used to evaluate the flap at the same intervals as above. 4. How long do you monitor your free flaps? At least 3 days for breast free flaps, and at least 5 days for head and neck free flaps. RATIONALE: Studies have shown that most breast complications occur within 48 hours, but most head and neck complications occur within 5 days. Therefore, one has to monitor head and neck reconstructions longer.5 Ninety percent of arterial thromboses occur within the first 24 hours. 5. A nurse calls to tell you that the flap looks white and cool. What do you do? A pale and cool flap has an inflow (arterial) problem, and arterial thrombus must be ruled out. One must evaluate the flap, and ensure that the environment is appropriate, including a warm room, warm blankets around the flap, and sufficient resuscitation of the patient. The flap should be evaluated for bleeding, and a pinprick test should elicit bleeding; however, the likely cause of a pale flap is a thrombus, and as nonoperative strategies are being undertaken, operative planning for re-exploration should begin. RATIONALE: Intraoperative hypothermia, volume depl etion, and blood loss can lead to peripheral vasoconstriction. These patient-specific factors must be assessed and corrected prior to final evaluation of the flap.6 However, re-exploration should not be delayed as volume is being replaced. 6. A nurse calls you to tell you the flap looks purple and has brisk capillary refill. What do you do? A congested flap has an outflow (venous) problem, and one must evaluate for venous obstruction. One can try initial maneuvers such as release of sutures, but one should be prepared for emergent return to the operating room. RATIONALE: Salvage rates are higher for venous obst ruction, but venous obstruction will lead to overall flap failure and death more quickly than arterial insufficiency.2,6,7 7. Your nonoperative strategies are not successful. What is your operative plan? Consent the patient for re-exploration, revision of the flap, and possible salvage procedures. First evaluate for external causes of compression, which can be kinking of the vessels, adjacent tissues, hematoma, or proximity of a drain. Once extrinsic causes are excluded, evaluate for intrinsic causes, which include vasospasm. If there is vasospasm, use lidocaine 2% or papaverine 0.25% as an external wash, and then proceed to perform a second anastomosis if possible; if needed, a vein graft can provide a tension-free anastomosis and can bypass injured vessels. Once extrinsic causes and vasospasm are excluded, evaluate for internal causes, which include early thrombosis (fresh clot) and late thrombosis (established clot). For early thrombosis, it is treated by a heparin flush at a concentration of 100 units/mL with or without a thrombectomy, using a no. 2 or 3 Fogarty catheter. For a late thrombosis (established clot), first heparinize, then perform a thrombectomy, and then use thrombolytics, which include streptokinase and tissue plasminogen activator (TPA). Streptokinase is used at 50,000 to 250,000 units in NS at a concentration of 5,000 units/mL, and TPA is used at 2 to 20 mg at a concentration of 1 mg/mL. The vessel is clamped with an atraumatic clamp proximal to opening, and the vessel is opened. The thrombolytics are infused into an open branch of the artery, left in for 5 to 10 minutes, and allowed to flow out. One then waits for 10 to 15 minutes, and performs the infusion once more (Fig. 5.2). RATIONALE: Authors differ in their dosages of TPA. Rinker et al8 use 2.5 mg, Casey et al9 use 2.0 mg, and Bui et al5 use 5 to 20 mg. 8. When do you decide the free flap will not work? If one has revised the flap and has been unsuccessful after 6 hours, one aborts the procedure. 9. The flap fails after all of your efforts. What do you do? There are three options: perform a second free flap, a local flap, or delayed reconstruction. If the patient is medically stable and has exposed vital structures and no local options, a second free flap is performed. If the patient is medically unstable for a second free flap, has exposed vital structures, and does not have recipient vessels, a local flap is performed. If the patient is medically unstable, has no local options, no recipient vessels, and no exposed vital structures, a delayed reconstruction is performed.
Overview
Questions
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine