Forehead Region
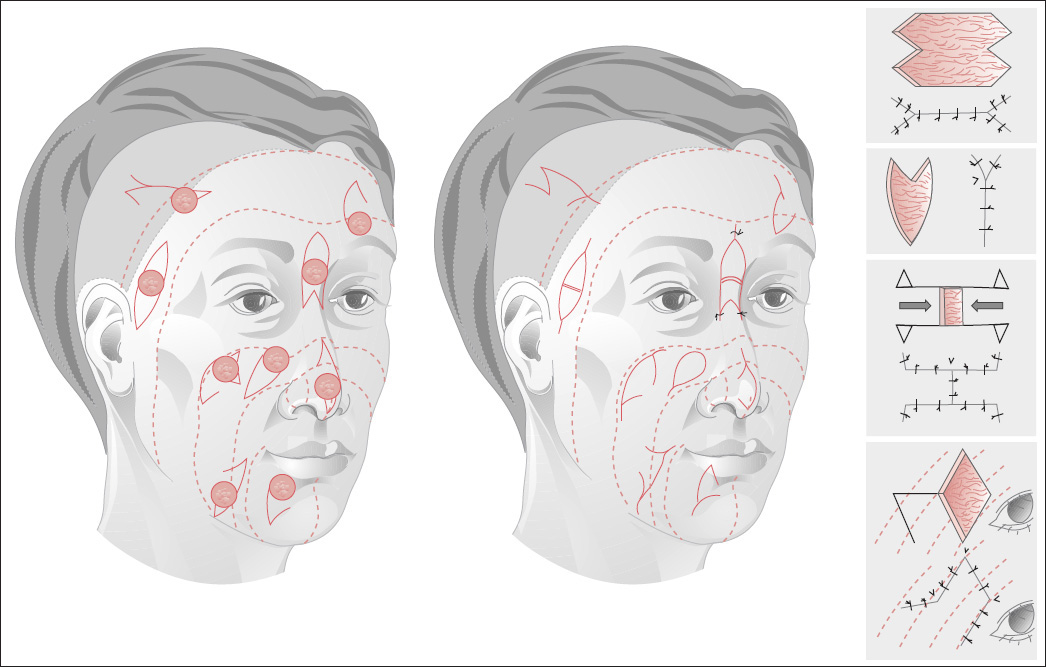
For smaller facial defects, an attempt is made to achieve coverage by means of flap advancement or local flaps ( Plate 1 ). Keep in mind that these flaps should be placed in RSTLs whenever possible (see p. 9).
If flaps cannot be obtained from the immediate vicinity of the primary defect, regional flaps are used. These are larger flaps involving the movement of tissue somewhat more distant from the recipient site.
The classic “regional flaps” from the neck and chest are no longer in common use. For the most part they have been replaced by myocutaneous island flaps (see p. 213) and free flaps. Even the classic “distant flaps,” transferred as tubed flaps from the chest or abdomen over a period of weeks or months, are very rarely used today and have been replaced by myocutaneous flaps and free tissue transfers with microvascular anastomosis (see pp. 221 and 227).
Small facial defects can be excised and reconstructed with small flaps using a technique that will place the scars as close to the RSTLs as possible (see Fig. 2.8a and Plate 1 ).
Median Forehead Region
The RSTLs run along the forehead and are perpendicular to the frown lines in the glabellar area (see Fig. 2.8a ). Forehead defects up to 3.5 cm in size, especially when near the midline, can be closed by mobilizing the surrounding tissue. Primary closure can be facilitated by making parallel or perpendicular incisions in the galea. Small defects can be managed with various advancement, rotation, and transposition flaps (see Figs. 3.1–3.27 ) and Z-plasties (see Figs. 2.15–2.18 ).
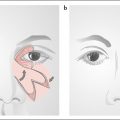
Wedge-Shaped Defects
( Fig. 4.1 )
Wedge-shaped midline defects that are based on the glabella ( Fig. 4.1a ) or frontal hairline ( Fig. 4.1b ) can be closed primarily by making an incision above the eyebrow or along the hairline and mobilizing the forehead skin.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


