Summary
Borders define the forehead.
Heals very well secondarily.
Can close under moderate tension.
Heals well regardless of vertical or horizontal closure orientation.
11.1 Algorithm for Closure
11.1.1 General Considerations
The forehead is a featureless, but prominent aesthetic unit (▶ Fig. 11.1). Its defining characteristics are its borders, the eyebrows, and hairline, and maintaining symmetry of these features is imperative. 1 The forehead lends itself to successful reconstruction with its robust vascular supply and inherent ability to heal well secondarily. 1, 2 It is also able to tolerate a significant amount of tension on closure and will heal well even when closed perpendicular to traditional relaxed skin tension lines. 1
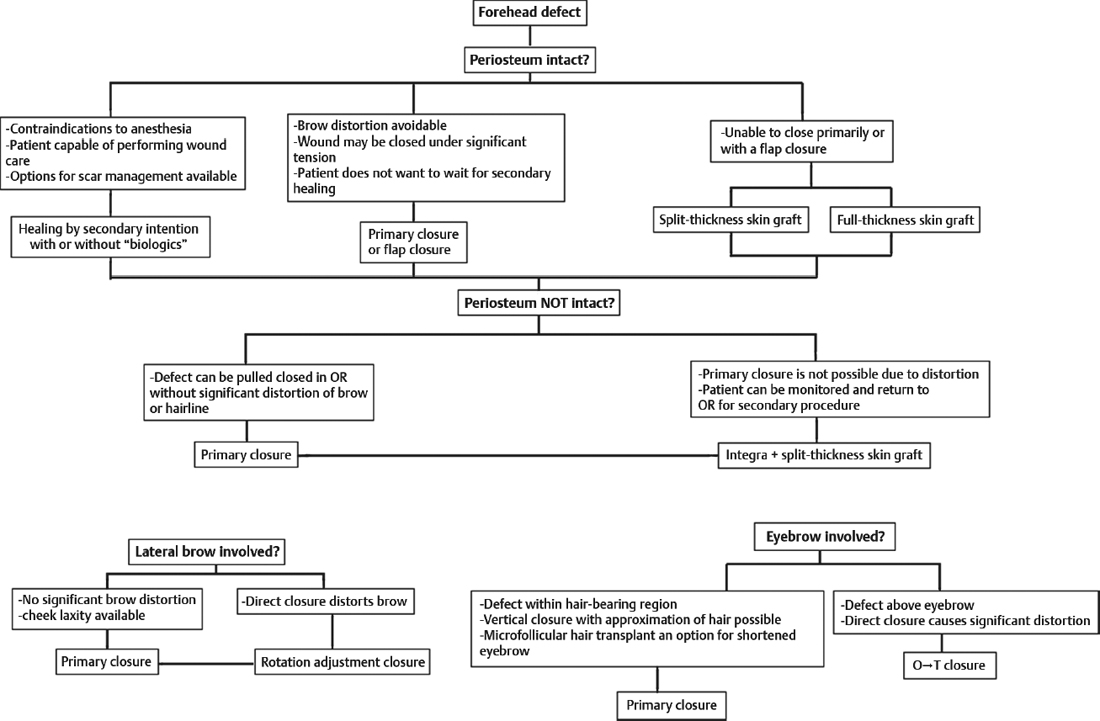
Fig. 11.1 Algorithm for forehead defect closure.
Improper management resulting in distortion of the hairline and/or eyebrows causes significant cosmetic deformity that can be difficult or even impossible to secondarily revise. When approaching a patient with a forehead defect, it is wise to at least consider the result if no surgery is done because this may well provide the best cosmetic result. This is well demonstrated by the results of foreheads allowed to heal secondarily after paramidline forehead flap elevation. 3
11.2 Commonly Applied Methods of Closure
Delayed healing with or without assisted wound healing agents (i.e., ACell or Integra).
Primary closure in either the vertical or the horizontal plane.
Full- or split-thickness skin-graft coverage either directly or preceded by Integra placement.
For defects that involve the eyebrow, use either direct closure or O to T closure.
Lateral temporal defects are quite common and merit special management, namely either direct closure taking advantage of the cheek laxity or simple rotation advancement flap with the incision placed in the anterior hairline.
11.2.1 Delayed Healing/Acellular Adjuncts
In general, defects allowed to secondarily heal will do well. With appropriate scar management, including dermabrasion, pulsed-dye laser, or late secondary scar revision, if necessary, can have an optimal cosmetic outcome. 4 The forehead is well supported by bone and allows secondary healing to take place with minimal scar contracture, the exceptions being the more mobile elements directly above the eyebrows. 5 Secondary healing must be carefully monitored and interventions made if significant eyebrow distortion is inevitable. The use of acellular dermis products (ACell, Integra, etc.) have provided a useful adjunct in this area and will result in improved healing time and improved final outcome 6 (▶ Fig. 11.2 and ▶ Fig. 11.3).

Fig. 11.2 A 65-year-old male status post wide local excision of melanoma on right temple. Wound was allowed to heal secondarily. Final result pictured 4 months after Mohs resection.

Fig. 11.3 (a,b) A 59-year-old male status post wide local excision of melanoma. Wound was allowed to heal secondarily. Final results shown at 3 months. (b) Planned scar revision with rotation flap performed 3 months after initial melanoma resection.
Large areas of exposed bone deserve special management. Earlier, large rotation advancement flaps or even free tissue transfers were required; however, the final results were often disfiguring and under all circumstances, significant surgical intervention was required. Management and placement of Integra wound healing products, ideally with a mesh bilayer product, is a preferable alternative. 6, 7 It is placed as a skin graft with no significant burring of the bone for defects of 6 cm or less. No vacuum-assisted closure is required. It is simply bolstered as a full-thickness graft for a week, at which point the bolster is removed and the patient may shower. Integra is monitored as the vascular ingrowth occurs over 4 to 5 weeks, at which point it serves as a robust base for either a color-matched full-thickness skin graft from the supraclavicular region or a split-thickness color-matched skin graft to be placed for final closure. 6 For an aesthetic result with split-thickness graft coverage, it is important to harvest color-matched skin, which can only be provided above the clavicle. Current surgical preference is to shave a small area of posterior scalp and harvest skin with a Zimmer dermatome or equivalent and use this for final coverage. In many ways, a scalp donor site is ideal. It heals very rapidly and, for hair-bearing patients, will be completely covered with no noticeable final scars (▶ Fig. 11.4 and ▶ Fig. 11.5).

Fig. 11.4 A 62-year-old white female patient with multifocal SCC (squamous cell carcinoma). Mohs excision left scattered exposed cranium. Wound was treated with Integra and subsequent color-matched full-thickness skin grafting to the forehead and split-thickness skin grafting to the scalp. Final postoperative results shown at 8 months.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


