Foot and ankle injuries in baseball provide unique challenges to the provider. Most foot and ankle injuries (ie, ankle sprains and contusions) can be managed non-operatively using a similar approach as in other athletic populations, but a few unique mechanisms of injury in baseball are important to be aware of. While upper extremity injuries such as ulnar collateral ligament (UCL) tears and labral tears are extensively reported on in the literature, there is a need for further baseball-specific research on foot and ankle injuries, especially given the increasing prevalence of these injuries over the past few decades.
Key points
- •
Foot and ankle injuries in baseball occur relatively less frequently, and the existing literature on these injuries is fairly non-specific to anatomic regions of the foot and ankle.
- •
The majority of foot and ankle injuries in baseball can be managed using a similar approach as in other athletic populations, but a few unique mechanisms of injury such as hit by pitch and base running are important to be aware of.
- •
There is a need for further research on foot and ankle injuries in baseball, specifically regarding injury prevention.
Introduction
Injuries in baseball play a critical role in an athlete’s career, as well as a team’s success. While the diagnosis and management of baseball injuries in the upper extremity are well described in the literature, baseball injuries in the foot and ankle have been reported with much less frequency. As baseball poses unique challenges both with chronic overuse and acute injury mechanisms, characterizing these injuries and synthesizing relevant literature is worthwhile. While most of these injuries can be diagnosed and managed as they are in other sports, this article highlights a few unique factors and considerations relevant to baseball.
Epidemiology
Several studies have investigated rates and characteristics of injuries in baseball players over the past 3 decades. Conte and colleagues first reported trends in professional baseball injuries using Major League Baseball (MLB) disabled lists (DLs) between 1989 and 1999. They reported the 5 most commonly injured anatomic regions were shoulder, elbow, knee, wrist/hand, and back, but they did not include an analysis of foot and ankle injuries as these were noted to be less frequent. Posner and colleagues subsequently evaluated MLB DLs from 2002 to 2008 and found foot and ankle injuries accounted for 5.5% of all injuries during that timeframe. Notably, foot and ankle injuries accounted for 8.8% of all injuries among fielders and only 2.9% among pitchers.
Li and colleagues prospectively evaluated injury incidence as a function of position using the DL of 1 professional baseball organization (major and minor league players) for the entire 2010 season. Of 291 players included, 134 were injured and missed a total of 3209 days during the season. Of these, 13 injuries (9.7%) occurred to the ankle/foot with 326 total days missed (25 days missed per injured player). Pitchers were least affected by ankle/foot injuries compared to all other injuries – only 2 pitchers had ankle/foot injuries and no days were missed.
Camp and colleagues evaluated the MLB Health and Injury Tracking System (HITS) from the 2011 to 2016 seasons in both the MLB and Minor League Baseball (MiLB). The HITS database is an electronic medical record and injury tracking system developed by the MLB in 2010, in order to create a more efficient method of tracking player medical histories and identifying injury trends. Camp and colleagues reported a greater proportion of lower extremity injuries (35%) compared to prior studies, with foot/toes, ankle, and lower leg/Achilles tendon injuries accounting for 14% of all injuries, higher than previously reported. Importantly, they identified ankle and Achilles injuries as specific targets for future research given the increasing prevalence at the professional level but relative lack of baseball-specific studies in the literature.
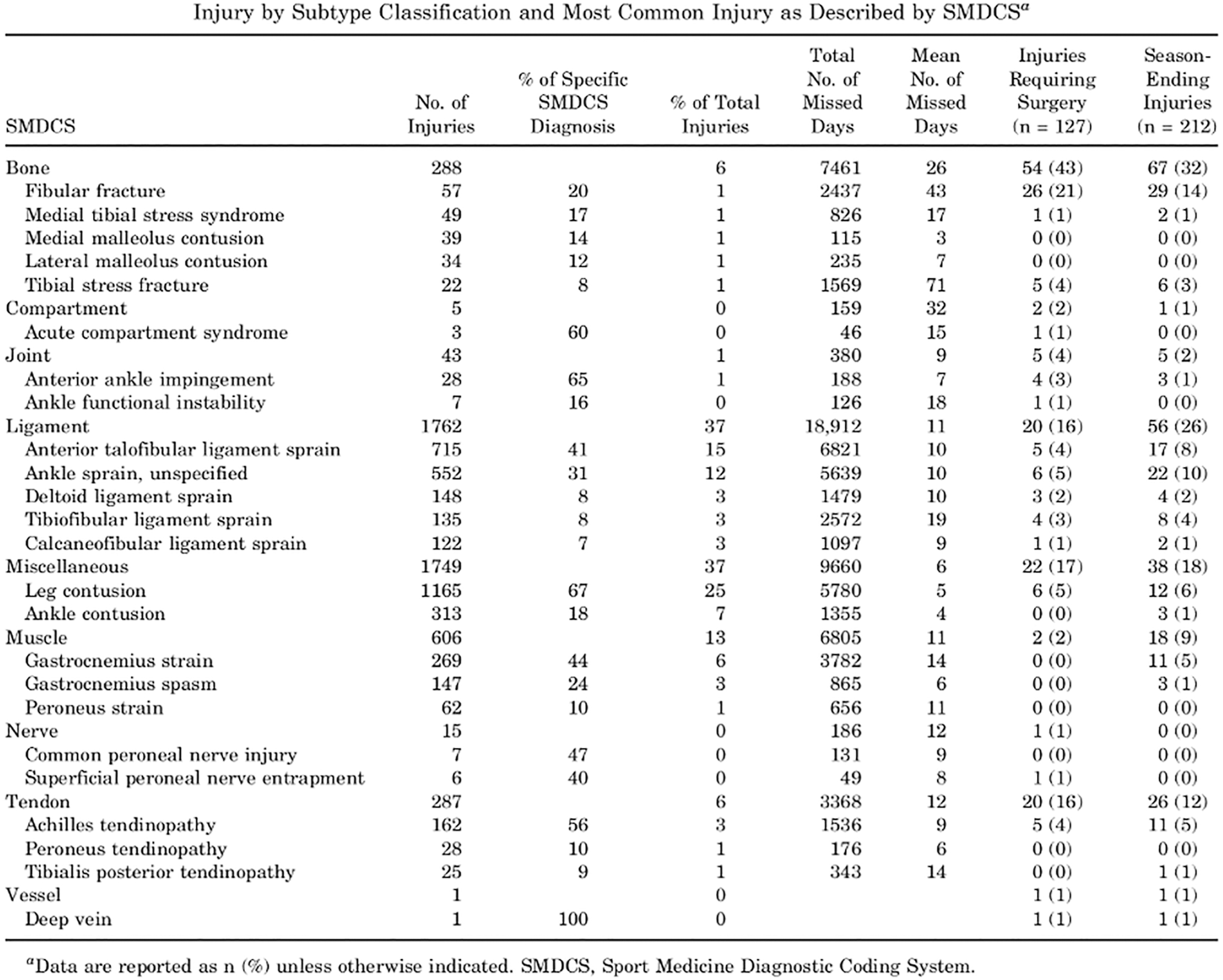
Lucasti and colleagues similarly evaluated the HITS database from 2011 to 2016, but isolated just ankle and lower leg/Achilles tendon injuries. There were 4756 of these injuries during that timeframe. The rate of injury in MiLB players was 1.4 times greater than the rate in MLB players, but MLB players were 1.7 times more likely to require surgery, although details of the surgeries were not reported. Infielders were 1.6 times more likely to experience injuries compared to any other position. The most common events during injury were base running, fielding, and batting, in order of decreasing frequency. The most common field location of injury was the home plate area. The most common mechanism of injury was noncontact in MLB and contact with the ball in MiLB. Finally, the most common injury subtypes were ankle sprain and leg/ankle contusion ( Fig. 1 ). Ankle sprains resulted in a mean of 11 days missed. The anterior talofibular ligament was the most commonly identified sprained ligament, accounting for 41% of ligamentous injuries. The most common injury requiring surgery was injury to bone (43%), with fibular fracture accounting for most of these injuries. Thirteen percent of injuries were muscular in nature, and gastrocnemius strain accounted for most of these injuries, which has been corroborated in the literature.
Salhab and colleagues evaluated the MLB DL for lower limb injuries between 2010 and 2016. They found 116 ankle injuries and 103 foot injuries with an average of 54.4 and 47.9 days spent on the DL, respectively. The most common ankle injury was a sprain (61/116), and the least common was fracture (4/116). In contrast, the most common foot injury was fracture (32/103) and the least common was muscle strain (6/103). The specific bones fractured were not reported.
Most recently, Carr and colleagues queried the HITS database from 2011 to 2019 specifically looking at location, frequency, and severity of injuries by position played. In the MLB, there were 2651 ankle/foot injuries (10.2% of all injuries). There were 681 in-game offensive ankle/foot injuries and 1162 defensive injuries. In terms of player position, 134 ankle/foot injuries occurred in infielders, 87 in outfielders, 83 in catchers, 252 in starting pitchers, and 125 in relief pitchers. The percentage of injuries affecting pitchers was notably higher than previous studies looking at the DL (updated nomenclature, injured list [IL]). This is likely because among pitchers, the percentage of severe injuries (defined as >5 days missed) was lowest for foot and ankle injuries compared to all other injuries in the HITS database. As a result, these athletes were probably less likely to be placed on the ILs, leading to a significant underreporting of foot and ankle injuries when simply looking at the IL.
Mechanisms of injury
While most foot and ankle injuries in baseball share similar mechanisms to other sports (running, cutting, twisting, or direct contact with another player), there are unique mechanisms specific to baseball. Two of these specific considerations are hit by pitch (HBP) and base running.
Hit by Pitch
Unlike most sports in which the offense controls the tempo, baseball is unique in that the defense, namely the pitcher, controls the action. Consequently, batters have little control over the location of an errant pitch, and its effects. As baseball has evolved over time, there have been various efforts to reduce injury from being hit by a pitch, from rules modifications to more widespread use of protective gear. Despite these efforts, HBP injuries still occur at a relatively high rate, and evidence suggests ball-player impacts account for 52% to 62% of baseball related injuries.
Camp and colleagues reviewed the HITS database and identified all MLB and MiLB players who sustained an HBP injury from 2011 to 2015. There were 2920 HBP injuries that resulted in at least 1 day out of play. The majority (88%) of these injuries occurred among MiLB batters. Twelve percent of all HBP injuries were to the lower leg/Achilles tendon, ankle, or foot/toes. While the injury rate, defined as the percentage of HBP events that required the player to miss at least 1 day of play, was relatively low ( Fig. 2 A), the mean days missed were relatively higher (15.5 days) for injuries to the lower leg ( Fig. 2 B). The most common injury type was a contusion. Of note, foot and ankle fractures were not reported in this article.
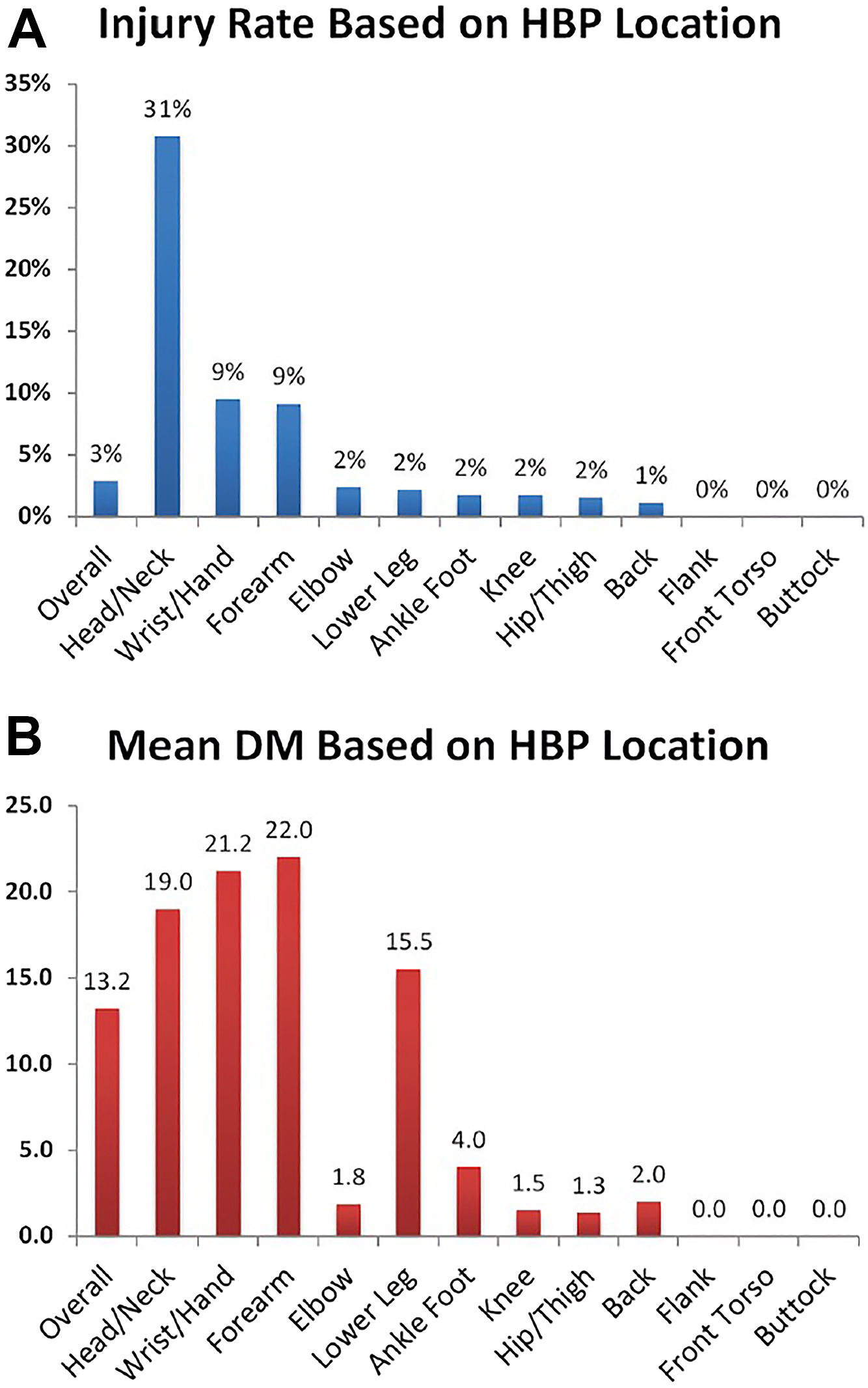
The annual number of all HBP injuries remained steady between 2011 and 2015, but trends in specifically foot and ankle injuries over time were not reported. As pitch velocity increased, the injury rate, as well as the mean days missed per injury, increased in a near linear fashion. The only significant predictor of injury was body region injured, with head/neck and distal upper extremity HBP events having a significantly higher risk of injury compared to all other body regions. While use of protective gear (helmets and elbow pads) was analyzed for HBP injuries to the head/neck and elbow, use of protective gear for the lower extremities was not analyzed.
Base Running
Another unique consideration relevant to foot and ankle injuries in baseball is base running. Base running can lead to unique mechanisms of injury including aberrant contact with the base while running, as well as sliding. Looking at the HITS database from 2011 to 2016, Lucasti and colleagues found the most common event during injury to the ankle or lower leg in professional baseball was base running. Of these base running injuries, 5% required surgery, but the surgeries specific to base running injuries were not reported. The mean days missed for injuries treated nonoperatively were 32, but again details of these injuries were not reported. Roughly two-thirds of injuries occurred while running and one-third while sliding. Running injuries most commonly occurred while running to first base, followed by second base in MLB players. Sliding injuries most commonly occurred at second base, followed by home plate.
To reduce the risk of base running injuries, the use of breakaway bases has been recommended. A traditional base is bolted to a metal post and planted in the ground, creating a rigid barrier to the sliding athlete. In contrast, a breakaway base is snapped onto grommets on an anchored rubber mat, and it can be dislodged during sliding. Several studies have evaluated the use of breakaway bases for injury risk reduction. Janda and colleagues found that the use of breakaway bases in recreational softball decreased sliding injury rate by 98%. In a subsequent biomechanical study, they found breakaway bases resulted in decreased force sustained to the foot and ankle during sliding, specifically the moments of inversion/eversion and dorsiflexion/plantarflexion upon impact. As a result of these studies, the American Academy of Orthopedic Surgeons (AAOS) has consistently recommended the use of breakaway bases at all levels of baseball and softball. The AAOS has also recommended adherence to the obstruction rule—the fielding player cannot obstruct the path of the runner—and even a “double bag,” separate bag for each team so that both the runner and first baseman have their own base.
While breakaway bases and double bags have been implemented in Little League Baseball, it has not yet been utilized on the professional level. A key factor in the hesitation to implement breakaway bases in the MLB has been concerns with officiating. The MLB has described the concern of breakaway bases becoming dislodged during the normal course of play, making it harder for umpires to make an accurate call. Further research is needed to assess the feasibility and impact of both breakaway bases and a double first base on injury risk reduction.
Fractures
Although rare, baseball players are at risk for foot fracture from direct contact with the ball at high velocity. This could be from HBP as previously discussed, during fielding, or from a foul tip while batting. While the majority of these injuries result in contusions, a few studies have evaluated mechanisms of foot fracture and return-to-sport outcomes after foot fractures in baseball players. Singh and colleagues performed a retrospective review of professional athletes undergoing operative fixation of foot fractures using archives of the public record between 1986 and 2016. They identified 9 professional baseball players who underwent operative management of foot fractures—4 fifth metatarsal, 3 navicular, 1 sesamoid, and 1 toe. Looking at on-base plus slugging for batters and walks plus hits per inning pitched for pitchers, there was no significant change in performance after foot fracture fixation.
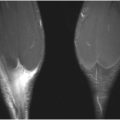
Bartz and Marymont reported 2 cases of MLB players with tarsal navicular fractures as a result of a foul tipped ball ricocheting off their lead foot. In both cases, the diagnosis was not made initially, as initial radiographs of the foot were read as negative for fracture. In 1 case, a computed tomography (CT) scan eventually revealed a fracture of the tarsal navicular with extension into the talonavicular joint. In the other case, MRI eventually revealed a non-displaced navicular fracture. Both athletes were treated with short-leg casting and returned to full activity. These cases highlight the high index of suspicion physicians and athletic trainers should have in baseball players with traumatic midfoot pain, as well as the need for routine weightbearing radiographs and advanced imaging, such as CT or MRI, of the foot when indicated. Treatment for these fractures is typically the same as for other elite level athletes.
Achilles tendon rupture
While not common in baseball, another foot and ankle injury that has been reported in the literature is Achilles tendon rupture. Achilles tendon rupture in professional and amateur athletics as a whole is increasing in incidence, and can have a significant impact on career trajectory. The risk of rupture is higher in older athletes who experience high tensile loads during sport. Some studies have suggested an association between tendinopathy and rupture, , but the history of a chronic process preceding rupture is controversial. As Achilles tendon ruptures are more common in sports involving repetitive jumping and cutting, the majority of literature has focused on management and outcomes of Achilles tendon rupture in sports such as football and basketball. , Nonetheless, baseball players are also required to perform these movements, as well as push-off and pivoting during hitting and throwing, both of which may be affected by the health of the Achilles tendon.
Saltzman and colleagues analyzed game performance metrics in MLB players before and after Achilles tendon repair using data from the MLB DLs, injury reports, game summaries, and public archives from the inception of the MLB until 2015. Of the 21 position players included in the analysis, only 13 (62%) returned to play for at least 81 games after Achilles tendon repair. Time to return -to-sport was not reported. In terms of injury timing, 69% occurred during the preseason or regular season, 12% in the playoffs, and 19% in the offseason. The players’ average age at time of injury was 31.6 ± 3.2 years at a median 9 years into their MLB careers. There were no significant differences in performance metrics before and after surgery. In terms of throwing and batting stance, 73% of injuries were sustained on the non-power (front) side, while 27% occurred on the power (rear) side. Athletes with injuries to the rear leg had significantly fewer plate appearances postoperatively. Trofa and colleagues found better results after Achilles tendon ruptures in MLB players, but in a much smaller and likely limited cohort. Five players were identified using public injury reports and press releases between 1989 and 2013. The average age of injury was 31 years. All players returned to play with no significant changes in performance. ,
The reported return-to-sport rate after Achilles tendon repair in MLB players (62%, Saltzman and colleagues) is lower than in other professional athletes. Using publicly available records until 2015, Jack and colleagues identified 95 National Football League (NFL) players who underwent Achilles tendon repair. They found 72% of these athletes were able to return-to-sport in the NFL at a mean 340 days after surgery. A third of repairs were performed during training camp or preseason. Postoperative performance metrics were significantly worse for running backs and linebackers compared to preoperative metrics. Using a similar methodology, Khalil and colleagues identified 47 National Basketball Association (NBA) players who underwent Achilles tendon repair between 1970 and 2019. Similar to the NFL data, 72% returned to play after repair. Players had shorter careers compared with uninjured controls and decreased performance metrics compared to their pre-injury baseline. In summary, the reported return-to-sport rate has been shown to be lower in MLB players compared to other professional athletes. However, in contrast to NFL and NBA players, performance metrics have been shown to remain unchanged in MLB players that return-to-sport.
Injury prevention
While systemic changes such as the implementation of breakaway bases can potentially reduce injury rate on a larger scale, there are several preventive measures baseball players can take to reduce the rate of foot and ankle injury. In their review of lower extremity injuries in professional baseball, Lucasti and colleagues suggested a few strategies, including increasing the number of days off per week, as well as implementing eccentric strengthening and stretching exercises. These eccentric exercises have been shown to be successful in hamstring injury prevention in baseball, as well as other sports such as soccer and ballet, , and could be particularly helpful in reducing the risk of gastrocnemius strain and Achilles tendon injury. Furthermore, balance and proprioceptive training could be beneficial in reducing the risk of ankle sprains, which has been substantiated in other athletic populations including professional basketball players. ,
In addition to injury prevention exercises, the timing of training and gameplay can play a critical role. A significant increase in injuries was observed in the 2020 MLB season, which was attributed to an increased acute to chronic workload ratio due to the interrupted preseason and compressed season during the coronavirus disease 2019 pandemic. , Platt and colleagues subsequently reviewed the 2021 season and found that foot and ankle injuries in particular increased further. They attributed these findings to the 2020 layoff and delayed effects of alterations in core strength and neuromuscular adaptation. From a preventive standpoint, they suggested focusing on core and posterior chain (trunk, pelvis, hamstring, and calf) strengthening, as well as neuromuscular control, which have been shown to be effective in other athletic populations. , Further research is needed to assess the impact of these preventive measures, as well as other measures such as protective gear, on foot and ankle injuries in baseball.
Clinics care points
- •
The majority of foot and ankle injuries in baseball can be managed using a similar approach as in other athletic populations.
- •
There should be a high index of suspicion for fracture in baseball players with traumatic midfoot pain, which should be evaluated with routine weightbearing radiographs and advanced imaging, such as CT or MRI, when indicated.
- •
Eccentric exercises, posterior chain strengthening, and proprioceptive training may be effective in reducing the risk of foot and ankle injuries in baseball.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


