21 Follicular Unit Transplantation or Follicular Unit Excision: Planning and Decision-Making
Summary
For example, a young male may sport a short hairstyle and not want a linear scar (no matter how fine), while a female or middle-aged executive may not want to undergo the extensive donor shaving required for FUE. Although both techniques are acceptable in many cases, there are still some notable instances that FUE or FUT is the preferred technique.
Keywords: follicular unit quality donor supply transection rates complications hair transplant surgery hair growth
Key Points
•Both follicular unit transplantation (FUT) and follicular unit excision (FUE) are state-of-the art techniques depending on the patient’s preference and indication.
•FUE has become a good substitute for FUT, but in some cases FUT still remains the most indicated technique.
•For the benefit of the patient, a hair surgeon should be able to master both FUT and FUE.
21.1 Introduction
In the last two decades, there has been a tendency for aesthetic surgery to become as minimally invasive as possible. The same goes for hair transplant surgeries, involving as minimal an incision into the scalp as possible during the procedure.
In modern hair restoration surgery, follicular units can be harvested in one of two ways: strip-follicular unit transplantation (strip-FUT or FUT), which is the microsurgical dissection of follicular units out of a strip of donor material (FUT), and follicular unit excision (FUE), where the follicular units are extracted individually and directly from the donor area.1,2
Strip-FUT (generally referred to as FUT) has been the state-of-the-art technique for many years replacing outdated punch and mini grafting techniques. FUT produced unparalleled clinical results in the recipient area but involved the creation of a linear scar.1,2 Although in general this scar is thin and not an issue for patients, there is always a risk for an unaesthetic wide scar, and even a “good” scar could be an issue for patients who desire to have very short haircuts. Over the years, improvements have been made to minimize linear donor scars; however, they cannot be totally eliminated and the risk of a wide scar is always present.3
FUE primarily developed in response to the wide linear scars that could occur in FUT. Initially, FUE was not well accepted by the hair transplant community. FUE was technically difficult, labor intensive, and associated with high follicular transection rates. Only small cases could be done, and the aesthetic results for FUE were not as good as FUT. In addition, it became obvious that FUE produced its own type of donor scarring (multiple small white dot).4,5
However, FUE results improved dramatically with the passage of time, thanks to continual improvement in skill, technique, and instrumentation. Today both FUT and FUE are capable of producing excellent recipient area results.6,7,8 However, FUE has the additional benefits of not producing a linear incision in the back of the scalp, and a less traumatic postoperative period. These “less invasive” donor-area properties combined with equivalent recipient results are one of the reasons for the high patient demand and subsequent rapid growth of the FUE procedure. According to the International Society of Hair Restoration Surgery (ISHRS) census, FUE grew from only 7% of all procedures in 2006 to over 50% by 2017.9
21.2 Current Controversy between FUE and FUT
From the onset, there has been much debate about the relative benefits of FUT versus FUE. For a long time, physicians justifiably felt that FUE had limited application because aesthetic results were inferior to FUT. However, the debate has changed now that FUE can deliver aesthetic results equivalent to FUT. Today the debate is more about “when, where, and why” would you choose one technique over another. There is still dispute among proponents of each technique as to which technique is best in different situations.10,11,12,13 This decision to do one technique versus another should be based on the patient’s unique situation as well as the specific advantages and disadvantages afforded by each technique. However, the majority of new physicians entering the field are learning FUE only. FUT is being offered less and less and if this pace continues, there is a possibility that FUE could totally replace FUT. For this reason, it is more important now than ever to take a close look at the relative advantages and disadvantages of FUE and FUT in different situations.
21.3 Potential Advantages and Disadvantages of FUE and FUT
•In patients with good laxity and density, a greater number of grafts can be moved in a single surgery with FUT than with FUE.14 Hasson and Wong repeatedly demonstrated the ability to harvest more than 5,000 to 6,000 grafts in a single-session patient with good laxity and donor density.
•All grafts harvested with FUT come from “safest” donor area and therefore are at less risk of loss over time.13,14,15
•*Strip-FUT grafts have more perifollicular tissue and a lower risk of transection. They are therefore less fragile.15
•**The total lifetime donor supply that can be harvested from the scalp over the life of the patient is greater with FUT + FUE than with FUE alone.12 This could be important in the subpopulation of patients who need higher numbers of grafts to meet their goals.15
•**With FUT you are not required to shave the entire donor area.
*This advantage may become less significant with the recent development of newer FUE punches and technology.
** This advantage may be changing as unshaven FUE becomes more available.
Disadvantages of FUT:
•A linear scar makes a short or buzzed haircut difficult and sometimes even impossible. These are popular hair styles today.
•The width of the scar is unpredictable and not always a “pencil-thin” scar.3
•The recovery time is longer, more painful, and has physical limitations.
•A larger team of specially trained technicians is required to perform the strip dissection.
Advantages of FUE:
•There is high patient demand due to less invasive nature of surgery.9
•There is no linear scar, making a shorter haircut possible after surgery.
•Although, scarring does occur with FUE, if implemented correctly, this scarring will not be visible to the naked eye even with the hair cut very short.
•Very short and almost pain-free postoperative recovery time with minimal physical limitations.
•Can “cherry pick” larger grafts (3 and 4 hair/FU) to get a higher hair-to-graft ratio when needed. The same is true for finer grafts.
•FUE allows the harvesting of grafts from areas other than the traditional safe donor area (SDA), which could not be harvested with strip-FUT in the past due to risk of visible scarring. This has significantly increased the available donor supply for transplantation . Although this was not the primary reason that FUE was developed, it has turned out to be a major benefit of FUE. New areas that can be harvested include the following:
–The area above and below the “safe donor area.”
–The temporal or nape area of the scalp.
–Beard and body hair from the chest, back, legs, pubic area, etc.
It should be mentioned that hair taken from outside the SDA may be lost in the future and that body hair does not give the same impact as scalp hair.
21.3.4 Disadvantages of FUE:
•* FUE grafts usually have less perifollicular tissue and are therefore at a greater risk of trauma and poor survival.
•* The risk of graft transection is higher with FUE than with FUT.
•Follicular unit grafts harvested outside of the “safe donor area” may not be permanent.
•Sometimes FUE procedures cannot get as many grafts in a single session.
•The lifetime supply of available grafts from the scalp may be less if FUE technique is used “alone” or exclusively, especially considering potential loss of grafts taken outside of the SDA. This has as yet unknown implications for the ability to meet density goals in some patients as hair loss progresses.14,15
•Significant scarring, a moth-eaten look, and donor depletion can occur with FUE in inexperienced hands who do not follow good donor management techniques. The risk is greater if punches greater than 1.0 mm are used or if the extraction density is pushed past a safe limit.
•To achieve maximum number of grafts safely via FUE, acceptance of a lower final donor density (homogenization) is needed.
•There is a risk of damaged or buried grafts.
*This advantage may become less significant with the recent development of newer FUE punches and technology.
21.4 Indications for FUT versus FUE
Based on the above advantages and disadvantages, there are certain situations that may be better suited for one technique or the other.
Situations where FUT may be preferable are the following:
•Patients who already have a linear scar as a result of previous FUT procedures but still have good laxity. Since they already have a linear scar, they have loss the primary advantage of FUE.
•Male or female patients with a longer hairstyle who do not care about a linear scar.
•** Male or female patients who do not want (or cannot cut) their donor hair short for the FUE procedure due to social situations. For example, older men (executives, TV personalities, etc.) may simply not want such a drastic change in hair style, even if temporary. Women who have long hair do not like the idea that it could take years for the donor hair to regrow to its old length.
•Older patients (preferably type 4–5+) with an advanced hair loss pattern (Norwood pattern V–VI) whose goals indicate a need of a high number of follicular units.
•Eyebrow transplantation to have a better perception of the patient’s hair curvature.
•A first attempt at repairing a wide scar in a patient who has had past strip surgery if he has good laxity. If the repair is even partially successful, you get immediate results and will save FUE grafts for other areas.3
•Patients with hair and skin characteristics that make FUE very difficult to perform such as black patients with extremely curly hair and splay.
** This advantage may be changing, as unshaven or long hair FUE becomes more available.
•Patients who have already had extensive FUE whereby further extractions will result in a visible area of donor thinning and are willing to wear longer hair to accommodate a linear scar.
Situations where FUE may be preferable are the following:
•Patients who simply do not want a linear scar.
•Patients with a short or military hairstyle where a strip scar would be noticeable. This would include women with modern short hair styles.
•Younger patients who need initial small procedures but have a lot of anxiety about the future. This gives young patients the option to stop the process and change to shorter hairstyles without having to worry about a linear scar.
•Repair of scalp donor scars from previous strip surgery, older large punch graft surgery, or other forms of trauma (Fig. 21.1a, b).
•Patients at risk of wide donor scarring due to an excessively tight scalp. FUE can be performed on a tight scalp.
•Patients who have had multiple previous strip surgeries and now are at greater risk of both poor yield and scarring due to a tight scalp.
•Small recipient areas such as temporal peaks, eyebrows, beard or mustache, or eyelashes. With FUE you can get the exact number and size of grafts needed as well as pick better matching hair for eyebrows, eyelashes, etc.
•FUE is useful for repairing hairlines by punching out and redistributing poorly placed grafts.
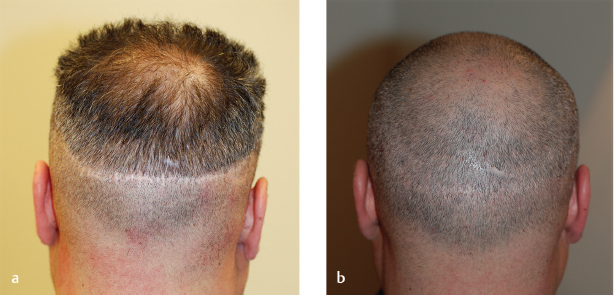
Fig. 21.1 (a) Old strip scar, (b) strip scar after repair by follicular unit excision.
Related posts:
 Methods and Techniques to Study Hair Cell Survival
Methods and Techniques to Study Hair Cell Survival
 The Patient with Minimal Hair Loss: Planning and Decision-Making
The Patient with Minimal Hair Loss: Planning and Decision-Making
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 East,West, and Southern Asian Hair Transplant Specifics
Contact Management Software and Its Utilization as a Marketing Tool
Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
East,West, and Southern Asian Hair Transplant Specifics
Contact Management Software and Its Utilization as a Marketing Tool
Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


