Introduction
Achieving success in microvascular free tissue transfers requires more than the technical ability to proficiently perform microvascular anastomoses. Preoperative planning, choice of recipient vessels, intraoperative execution of dissection, elevation and insetting, along with postoperative monitoring are all equally important to a successful outcome. Although having a free flap survive may be a prerequisite for success, a truly successful outcome is being able to achieve the preconceived reconstructive goals of closing a wound or building a part. Most large series report a microvascular success rate of at least 90% and a salvage rate of the flaps that initially “went down” of about 50%. In most cases, salvage was predicated on a timely diagnosis of vascular compromise and prompt intervention.
The decision to surgically re-explore a flap suspected of vascular compromise may be clouded by significant psychological stress of the surgeon, patient, and the patient’s family. The surgeon’s initial response frequently is “denial.” All too often, precious time is wasted as the surgeon rationalizes early and sometimes not so subtle signs of vascular compromise. The personal fortitude in recognizing what may be perceived as one’s own impending “failure” is paramount. Overcoming this mental hurdle is the first step in proactive resolution of a problem. Recognizing that “even the masters” have failure rates of up to 10%, with re-exploration rates of up to 16%, may even venture one to state that re-exploration of some cases is part and parcel with the reconstructive effort. Recognizing this, it is important not to forget to discuss the possibility of the need to return to the OR in the postoperative period, with the patient and their family, preoperatively. We agree with Schwabegger’s approach of dealing with this, as he states: “Flap re-exploration should be approached with the attitude of ‘let’s take a look and see what is going on’ instead of ‘I have a disaster on my hands that I have to deal with and everybody around me, including the patient and his family, is disappointed in me.’ ”
Recognition that There is a Problem
Early recognition of the presence of a problem and rapid action to address it, are key to flap salvage. While Chapter 29 addresses the topic of postoperative flap monitoring, we will briefly underscore the importance of the clinical assessment. A multitude of devices present on the market definitely have a role in flap monitoring and, in many practices, have enabled tapering of strict and costly monitoring routines (i.e., hourly flap checks in the intensive care units) for flaps with exposed cutaneous paddles. Nevertheless, basic tenets of clinical assessment and monitoring should be second nature to all members of the operative and perioperative staff. Surgeons should take the lead in ensuring that the clinical diagnostic art is not lost on the technological science of the devices. Suspect changes in flap color, turgor, temperature, and capillary perfusion in flaps with an exposed cutaneous paddle, as well as drain output should alarm the surgical team to a potentially serious problem, even if ancillary monitoring modalities show no aberrancies. Similarly, one should recognize that all monitoring devices have a certain incidence of false-positive results and decisions on intervention should be correlated with clinical signs.
All patients who have undergone a microvasculature free tissue transfer, replant or revascularization should be monitored by nursing staff specifically trained in assessing tissue viability and flap monitoring. This entails being able to provide clinical surveillance at appropriate intervals, including hourly flap checks for the aforementioned clinical parameters, as well as hourly Doppler checks for at least the first 48 h in all complex reconstructions. All patients that undergo free tissue transfer are not comparable in their complexity or risk for failure and may require individualized strategies for the type and duration of monitoring. Although all our free tissue transfer patients go to the intensive care unit (ICU) postoperatively, straightforward autologous breast reconstruction in otherwise healthy patients is routinely monitored with a near-infrared tissue oximetry monitoring device, which can be monitored remotely with smartphones or tablets and typically leave the ICU 12–24 h postoperatively, after which clinical monitoring occurs on the surgical floor every 4 h (many centers continue to monitor every 1–2 h for the second 24 h period and every 2 h on the third day depending on the type of flap and the concern for problems). These healthy patients are generally discharged on postoperative day 3 or 4. Due to a number of factors, patients who undergo reconstruction for complex head and neck defects or lower extremity wounds usually have a longer ICU stay. In comparison with healthy breast reconstruction patients, head and neck patients as a group, tend to have more comorbidities; their nutritional status may be compromised due to their baseline pathology and/or history of radiation; the presence of recently dissected large, radiated vessels in fresh surgical field places the patient at risk for devastating bleeding in the case of vessel or anastomosis disruption; and potential airway issues all merit more intense ICU monitoring and care. In addition, although Kroll et al. observed that the majority (80%) of thrombi occurred within the first 2 postoperative days and that 90% of arterial thromboses occurred within the first 24 h, Bui et al. found head and neck patients were at risk for up to 5 days postoperatively. Patients undergoing lower extremity reconstruction are kept at strict bed rest for the initial 5–7 days after surgery, and thus may benefit from closer nursing vigilance that may not be available on a regular surgical ward. This is mainly to permit leg elevation to facilitate venous drainage, which can be a major source of problems in the early postoperative phase. In addition, these patients are more likely to have compromise of their flap if they had a chronic wound and or required vein grafts. Monitoring of patients with free flaps to the scalp, trunk, or genitalia is individualized depending on the complexity of the case and comorbidities of the patient. Buried flaps (without an exposed cutaneous paddle), muscle flaps covered with a skin graft, and skin flaps in very dark-skinned patients are all typically difficult or impossible to monitor clinically, and are therefore generally monitored using an implantable Doppler probe.
Preparing for a Re-Exploration
Preoperative Considerations
The following elements should be incorporated in the re-exploration process for a compromised flap:
- 1.
Exclusion of problems related to external effects (compression by dressings, positioning, etc.
- 2.
Decision to surgically intervene
- 3.
If anastomotic clotting is suspected, then consideration should be given to empirically heparinize the patient systemically at this point to try and stop propagation of any clot while preparing to go back to the OR.
- 4.
Informing the patient and family of the problem and the need for surgical intervention
- 5.
Obtaining informed consent, including informing the patient of the possibilities that the wound may need to be temporarily left open, other flaps may be required, and vein grafts, skin grafts, or local tissue harvest may be needed. They need to understand that new incisions and donor sites may be required and the possible need for more than one procedure to complete the reconstruction.
- 6.
Informing the operating room and anesthesia staff that urgent re-exploration is required. An operating room, microscope, microsurgical instruments, and specific pharmacological preparations need to be prepared. The team should be informed of the possibility that if salvage is not possible, the flap may need to be replaced by a new one, or an alternative reconstruction at that time, which will significantly increase operative time.
- 7.
Optimizing the medical condition and hemodynamic status of the patient within a reasonable timeframe
- 8.
Obtaining the necessary preoperative work-up, including discussion of other treatment options (second free flap, regional flaps, or other reconstructive options)
- 9.
Preparation of blood products that may be needed
- 10.
Expedient transport and preparation of the patient
- 11.
If the surgeon performing the re-exploration is different from the surgeon who performed the flap, they should communicate about the surgical anatomy, location of anastomoses, suggested sequence and approach to the anastomosis, and other important nuances that only the original team would know. In addition, the original microsurgeon may have intuitive suspicion about what might have gone wrong during the initial surgery, and may provide useful advice for the re-exploration.
- 12.
Operative intervention: exploration, diagnosis, and solution. The most experienced surgeon should lead the re-exploration process.
If executed in a timely manner, flap salvage can be achieved with a high rate of success. To facilitate an expeditious process, one should consider having a standard flap re-exploration protocol electively agreed on by the surgical team, anesthesiologists, and operating staff. This would include the understanding that flap exploration should be considered a surgical emergency with urgency on par with life- or limb-threatening emergencies.
Equipment
All of the standard equipment for free flap surgery must be available immediately from the start of revision, including an operating microscope (or at the very least loupes with sufficient magnification, as a temporary alternative). Ideally, one should have readily available a sterile surgical pack with essential instruments saved for these emergencies, as well as equipment (including mini-Fogarty catheters) and medications (heparin, lidocaine, thrombolytics) that may be needed.
Medications
There is no consensus among microsurgeons on the perioperative use of anticlotting agents. This is particularly true for elective straightforward microvascular transfers. In contradistinction, when an anastomosis fails and requires multiple revisions or a salvage procedure, most surgeons will use some medication to minimize the chances of recurrent thrombosis.
Aspirin
Although there is compelling evidence demonstrating the beneficial effect of aspirin on decreasing microvascular clotting in animal studies, there is no statistically significant clinical data in humans. Despite this, many surgeons use low-dose aspirin to decrease platelet aggregation beginning pre- or postoperatively and continue it for 2 weeks postoperatively when the endothelium has resurfaced the anastomosis. Our protocol includes insertion of a 325 mg aspirin suppository per rectum at the beginning of the case and continues 81 mg by mouth daily postoperatively.
Heparin
Heparin is a powerful antithrombotic that can be used intravenously as a bolus or continuous drip, topically, or via the subcutaneous route. Perioperative subcutaneous heparin is the only route that has been demonstrated to decrease thrombosis rates. The use of intravenous heparin in microsurgery is controversial and has been associated with an increased hematoma rate. Despite this, some authors recommend systemically heparinizing with 3000–7000 units intravenously at the time of anastomosis. Postoperative doses of 100–500 units/h have been advocated by some authors with or without titrating the dose up to a aPTT 2–2.5 times the normal. Our protocol includes heparin prophylaxis (5000 units subcutaneously) before induction of anesthesia, as routine DVT prophylaxis. Systemic heparinization is usually limited to situations in which patients are known or highly suspected of being hypercoagulable or ones that have demonstrated intraoperative or postoperative thrombosis of the vascular anastomosis. If multiple revisions of the anastomosis were performed (due to the increased risk of thrombosis secondary to intimal damage), we continue a heparin drip at a rate to 500 units/h without titrating the aPTT, for several days after re-exploration. Transient (one dose) systemic heparinization should be considered when a major extremity artery is cross-clamped, especially in patients with peripheral vasculopathy.
For both the initial procedure and the take-back, local irrigation with heparinized saline has been used with varying doses, ranging between 10 and 500 units/mL.
Irrigation with a concentration of at least 50 units/mL helps prevent thrombosis without systemic side effects, whereas topical solutions of 250 units/mL have been shown to alter the partial thromboplastin time.
In patients with known hypercoagulable states, intraoperative issues that may predispose to clot formation (such as suspected vessel injury), or if long vein grafts were used, an intravenous heparin drip at a rate of 500 units/h is used. Currently, there is no clinical evidence to suggest this practice has outcome benefits. While animal studies suggest that routine administration is beneficial for anastomotic patency, it entails an increase in hematoma rates. Despite this increased risk of hematomas, most surgeons heparinize patients that have required multiple anastomotic revisions, unless they are suspicious of the presence of heparin- induced thrombocytopenia (HIT) or have undergone a concurrent neurosurgical procedure in which anticoagulation is associated with increased mortality.
Dextran
This polysaccharide has been used in microsurgery due to the reported function related to inhibition of platelet aggregation, indirect pro-fibrinolytic activity, as well as rheological function. Some surgeons use the low-molecular-weight preparation as part of the perioperative protocol (dextran 40 at 25–50 mL/h). However, most seemed to have swayed from this practice due to reports of adverse effects in the form of anaphylactoid reactions and acute respiratory distress syndrome. Pretreatment with dextran 1 may avoid this.
Vasodilators
The most commonly used and reported smooth-muscle relaxing vasodilator preparations are lidocaine (2% or 4%), papaverine 0.25%, and verapamil (see Arterial Spasm , below). There is limited experimental evidence that topical administration of chlorpromazine has vasodilatory effects; some authors routinely use it systemically in the postoperative period.
Thrombolytics
As a class, all thrombolytics act by converting plasminogen to plasmin, an enzyme that degrades fibrin. None of the three main thrombolytics (streptokinase, urokinase, or tissue plasminogen activator) commonly available have been shown to have superiority to their counterparts. At the time of writing this chapter, according to the FDA registry, urokinase has been discontinued from availability in the United States. Different authors report equivalent success rates with varying dosages of the same drugs. It seems that the main determinant for drug selection is surgeon’s preference and institutional availability. Since the re-exploration “event” can be stressful on the surgical and ancillary team due to the high acuity, the shortened timeframes, and the need for equipment not routinely used, it is imperative that the lead surgeon be familiar with what is available and how it should be prepared and used (see Vascular Thrombosis , for details on use).
Operative Set-Up
Once the decision to take the patient back for exploration has been made, the entire team should be notified and made aware that the revision could be anything from a brief inspection, to a prolonged revisional reconstruction (revising the initial flap or performing an alternate reconstruction). In managing personnel, factors such as fatigue and extra surgical tasks should be accounted for. If available, additional staff should be called in to facilitate the revision (to simultaneously dissect an alternate flap, or harvest vein grafts) or relieve fatigued members of the team.
Considerations in patient positioning should include preventing any further damage to the flap, permit stepwise exploration that will reveal the compromise culprit, allow optimal ergonomics for the operator, and concomitantly permit secondary maneuvers (i.e., a second flap, and vein, or skin grafts). Notwithstanding the urgency of the case, standard surgical preparation and safe positioning steps should not be overlooked.
Preparing the surgical field should be performed carefully, particularly in the presence of an open wound from suture release, dehiscence, or necrosis. Aggressive detergents and alcohol-based preps should be avoided in open wounds, as they will chemically harm the pedicle or open wound. If Betadine (povidone-iodine) solution is used, it may be washed off after it dries, so as not to interfere with the flap color assessment.
Although not commonly performed, catheter – directed thrombolysis under angiography has been advocated by a few authors, following techniques similar to primary coronary angioplasty.
Approach to a Compromised Flap
Timing of impending flap failure can be divided into four time periods:
- 1.
Immediate (intraoperatively)
- 2.
Early (0–12 h)
- 3.
Delayed (12–48 h)
- 4.
Late (beyond 48 h)
Diagnosis of flap compromise in each phase is discussed here, along with the primary causes of each phase, and the highlights of the authors’ approach to treating each particular issue.
Intraoperatively: Immediately After Completion of the Anastomoses
Technically, this time period would not be categorized as a “re-exploration.” A brief outline is given here of our intraoperative maneuvering, that adheres to principles that would later guide a re-exploration, and serve as a reminder of how to avoid the need for a take-back.
Initial Inspection
Following release of the microvascular clamps, flow should be noted across the anastomoses and the flap is inspected for perfusion. If the anastomoses appear to be open, the surgeon should avoid early manipulation of the vessels, particularly around the area of the anastomosis for 10–20 min. This may interfere with the vessels accommodating to reperfusion, and cause undue early trauma and thrombosis. If there is any question about the flow, a distal milking test can be performed to establish if there is flow (see Stripping the Pedicle , below).
If no vascular inflow to the flap is detected, or if venous outflow is inadequate, the vascular pedicle and recipient vessels should be inspected for kinking, compression, or twisting along its course. If kinking, compression, or twisting is encountered and cannot be alleviated by manipulation of the flap or its pedicle, then the anastomosis should be divided and redone without kinking, compression, or twisting. Flaps with small-caliber vessels (<1 mm) may be prone to spasm. In this situation, consideration should be given to irrigating the pedicle with warm fluid and smooth muscle relaxants (such as lidocaine or papaverine). If there is no kinking, compression, twisting, or spasm, the anastomosis should be redone.
Most flaps are inset or at least tacked in place before the microvascular anastomoses are completed. Periodic checking of flap perfusion during the final insetting is important, as tissue swelling or inaccurate flap design may preclude safe wound closure. In this situation, the inset is undone and the pedicle inspected; if flow improves and no direct pedicle issues are found, the insetting is revised. Flaps that do not tolerate insetting without compromise need to be left partially open. The exposed soft tissue may be closed with a skin graft, biologic dressing, or negative-pressure wound therapy device.
Medical Optimization
Even the best-done microanastomosis with delicately placed microvascular clamps will cause some intimal damage subject to platelet adherence and aggregation. Low flow in an injured vessel is more prone to clotting. High perfusion pressures seem to mitigate these small, localized hypercoagulable regions around microvascular anastomoses. One of the best ways to minimize clotting is to maintain high perfusion pressure. Therefore, concomitant to the operative exercises, external reasons for low perfusion need to be excluded. Some may be as obvious as neglecting to release microvascular clamps that may be obscured in the operative field or as mentioned above, a kink or twist of the vessels either proximal or distal to the anastomosis. Extremity tourniquets should be completely released or removed. Patient hemodynamics should ensure a strong perfusing pressure head. Low perfusion pressure may be due to hypotension, inadequate volume, and hypothermia, and rarely from the administration of sympathomimetic drugs by the anesthesiologist. Communication with the anesthesiologist throughout the case is of paramount importance, as low perfusion pressure from any of the above causes will not only jeopardize the flap but will make flap monitoring difficult. This communication should reveal whether intravascular fluid status is optimized and if any vasoactive medications were given, which ones, and at what point. Recognizing that except for flaps with small pedicle diameters (<1 mm), most vasopressors seem to have little effect on pedicle flow and perfusion pressure tends to be more important than any vasoconstriction caused by pressors. Hypothermia is a frequent cause of decreased perfusion to the microcirculation, either through spasm of the vascular pedicle or through decreased perfusion to the peripheral vascular system. Therefore, the temperature of the patient should be continuously monitored throughout the case. If the patient becomes cold, arrangements should be made to warm the patient (see Intrinsic Flap Compromise , below.) We advocate judicious administration of warmed crystalloid fluids during the case, titrated to urine output, heart rate and blood pressure, with colloid supplementation to limit swelling. Excess swelling can compromise flap perfusion and insetting.
ReAssessment
After the above steps have been taken, the pedicle is reinspected. If no cause for the compromise is identified, evaluation of the anastomosis should be performed. Whereas a milking test proximal or distal to anastomoses is safe and will show if there is flow across the anastomosis, the presence of a small thrombus at the anastomotic site might be sufficient to compromise flap perfusion due to a “stenosing” effect, even though a milking test still suggests patency. A milking test across an anastomosis can be dangerous. Having said that, occasionally, when done, flow may be reestablished. If flow decreases again, the most likely diagnosis is a clot that was temporarily dislodged by the milking test. In this situation, the anastomosis should be redone. A ring resection of the anastomosis should be performed, excising the thrombogenic culprit (e.g., intimal flap, back-wall stitch, or a platelet clot in the lumen). Although it is prudent to resect the minimal length necessary to avoid shortening of the vessels thus hindering reanastomosis, the new cut end of the vessel should be pristine. To avoid tension, one should not hesitate to use arterial or venous grafts to bridge any potential gaps. To avoid prolonged warm ischemia time, consideration should be given to cooling the flap, while preparation and harvesting of vessels grafts is being done.
On completion of the anastomotic revision, the assessment is repeated. If there still is no perfusion or drainage, anatomic anomalies of the recipient vessels should be considered. Such anomalies may include unrecognized prior surgical alterations (i.e., previous ligations or bypasses), post-traumatic vascular strictures, prior thrombosis, or congenital variances. Whereas arterial adequacy of the recipient vessel is readily evaluated prior to the anastomosis, venous drainage insufficiency is more difficult to ascertain. If it is concluded that the arterial inflow or venous outflow problems originate proximal to the anastomosis site, the anastomoses are reopened, and micro-Fogarty catheters are introduced into each recipient vessel, inflated and retracted to remove clots. Intubating the vein in particular should be done with exquisite delicacy due to the venous wall fragility; any forceful insertion may preclude future utility of the vein due to iatrogenic intimal damage. If a recipient vessel patency cannot be confirmed, alternate vessels should be selected, and the use of vessel grafts considered. If the recipient vessels are patent, and the vessels of the pedicle are clotted distal to the anastomoses, the thrombus should be extracted from the vessels. Grabbing the thrombus with microforceps and gently pulling it out of the vessel while it is being gently irrigated with heparinized saline can be successful in fresh thrombi. If the entire thrombus cannot be removed, then considerations of using a Fogarty catheter in the flap vessels should be considered. If the possibility of embolization into flap is entertained, thrombolytic agents should be employed into the flap. Once flow is established, heparinizing the patient should be considered. If blood flow through the pedicle is reestablished but the flap tissue is not perfused, this is called a “no-reflow phenomenon.” If flap perfusion cannot be reestablished, the flap will not survive. If no technical or mechanical cause of repeated thrombosis can be established, then the diagnosis of thrombophilia should be considered (see below).
After Leaving the Operating Room: Within the First 12 Hours
If a problem is to occur, it will most likely manifest within this first few postoperative hours. Anticipated “normal” swelling of the flap may obscure the diagnosis of early flap failure, and color changes in the flap are a relatively late sign of vascular compromise. The diagnostic challenge seems to be greater in patients of color, in which the natural skin pigment further masks subtle color changes that would signal the presence of a problem in lighter-skin patients. External monitoring devices such as near-infrared tissue oximetry may be useful in early detection. Emphasizing once more that clinical acumen is the basis of problem recognition and solving, the Achilles’ heel of clinical flap monitoring exists in the change of shifts. This is of particular importance when less experienced staff are charged with the clinical surveillance during the initial postoperative period, in which the majority of problems arise. Accurate bedside communication and information transfer are crucial. To decrease observer error and shorten the time to address flap issues, digital photography has been utilized in flap monitoring. Some surgeons have further ventured to normalize the image interpretation with the use of standardized color cards photographed in the frame capturing the flap to provide a reference for assessment and compensate for variations in lighting, exposure, white balancing, etc.
The issue of diagnosis can be more complex in non-skin flaps. Color, volume, and turgor are all difficult to assess and seem to occur relatively late in the failure of muscle flaps. Other forms of monitoring should be employed such as implantable Doppler probes. Recognizing the problems of false-positive results of implantable Dopplers, one should also consider incorporating an external skin or tissue paddles for monitoring purposes. Similar issues exist with buried adipofascial, bowel, and bone flaps.
Extrinsic Factors of Flap Compromise
This includes factors associated with the anatomy of the wound bed, implanted devices, insetting, dressings, and hematomas. These elements might cause problems that manifest during the early postoperative period, and, to a lesser extent, at other time points.
Wound Bed Anatomy
Ideally, this should be a non-issue if properly planned for before, and executed during surgery. Failure to provide an adequate geometric environment for flap inset can lead to problems that manifest in the early postoperative phase. Bone and cartilage ledges, as well as prominent muscle can become the foci of kinking, stretch, or torsion compression of the pedicle. Bone prominences or edges should be excised or smoothed out; troughs in muscle or bone can be created to accommodate a more direct lie of the pedicle. Providing appropriate vessel length should accommodate for dynamic structures such as tendons and joints.
Implanted Materials
These may cause issues arising early on related to placement, or at the later timeframe on device extraction.
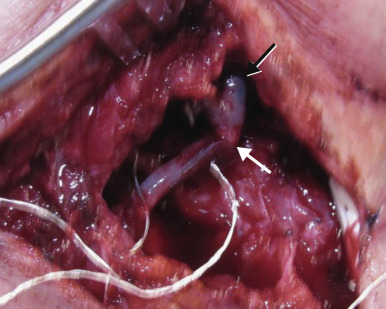
Placement of devices such as drains and implantable flow Doppler monitors, may seem adequate intraoperatively, but postoperative tissue changes, such as tissue edema, application of external suction, and patient movement may cause unfavorable alterations in the geometry of the surgical field and result in kinking or pressure on the pedicle ( Fig. 28.1 ). These changes should be accounted for, and the task of placing these devices should not be relegated to a junior member of the surgical team. Correspondingly, planning of device placement should also allow for safe removal, so as to not disrupt critical elements of the procedure. Poorly placed sutures for flap inset or skin closure can unintentionally distort the pedicle anatomy.