Flap |
|
Tissue |
Skin |
Course of the vessels |
Runs with the fascia of the first dorsal interosseous muscle |
Dimensions |
2 × 4–6 cm; pedicle or free flap located on the proximal phalanx of the index finger |
Extensions and combinations |
Rarely tendon strips from the proper extensor indicis; terminal branch from the superficial radial nerve |
Anatomy |
|
Neurovascular pedicle |
— |
Artery |
DMCA nourished from the princeps pollicis artery |
Veins |
Small venae comitantes; larger subcutaneous vein |
Length and arc of rotation |
Artery, 3–3.5 cm; vein, 3–6 cm |
Diameter |
Artery at the level of princeps pollicis, 2–3 mm; vein, 3–5 mm |
Nerve |
Terminal branch of superficial radial nerve |
Surgical technique |
|
Preoperative examinations and markings |
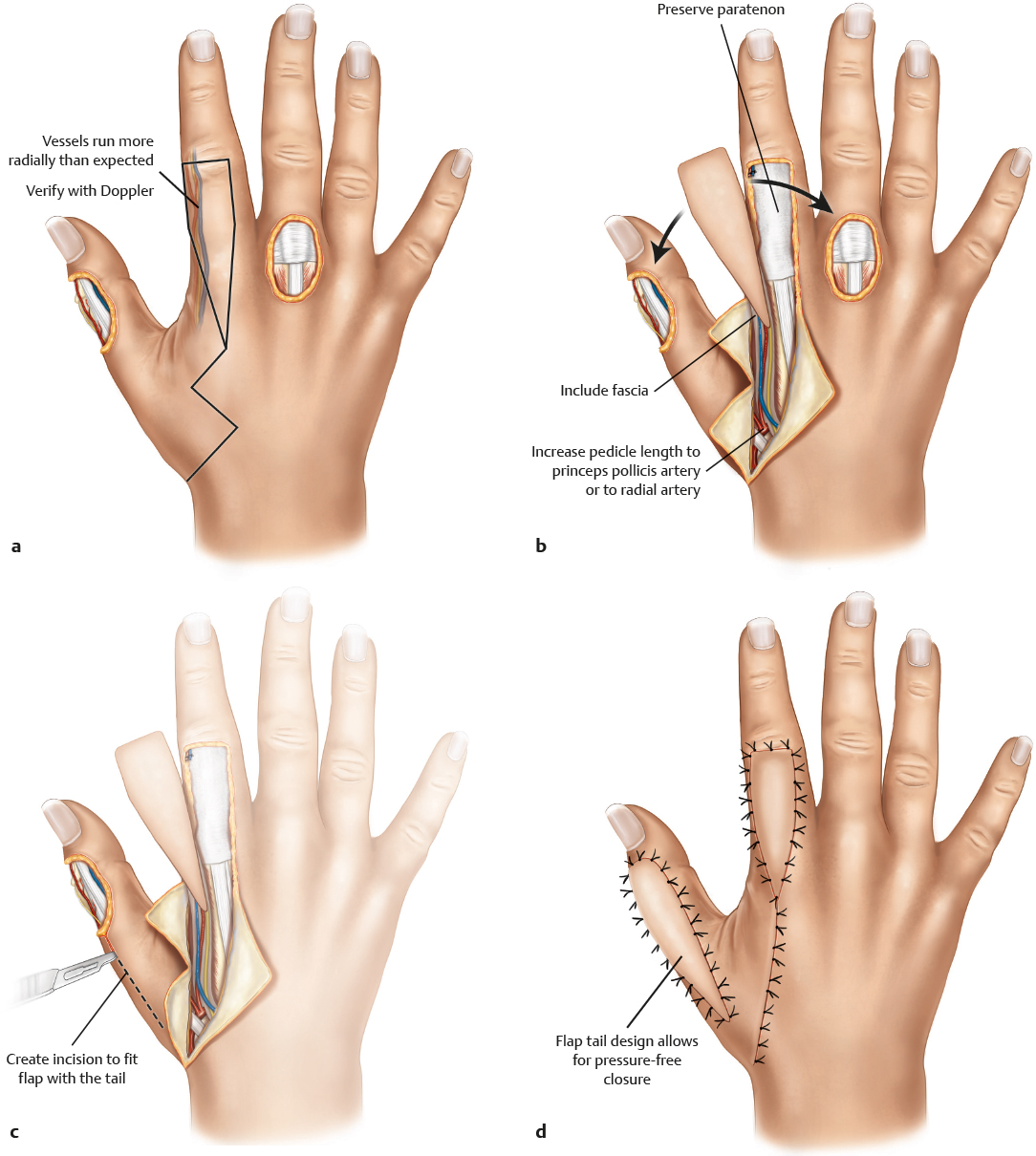
Preoperative Doppler examination for the presence of vessels is mandatory; mark the course of the vessels on the skin, because they are always located more radially than presumed |
Patient position |
Supine with arm on arm table; tourniquet use during harvest |
Dissection |
Incise skin along the markings along the second metacarpal; incise the interosseous muscle fascia; preserve the intermuscular septum and raise the fasciocutaneous flap, including the fascia; take care to include the nerve; create a de-epithelialized pedicle; leave approximately 0.5–1 cm of fatty tissue around the artery; preserve the paratenon above the extensor hood; open the tourniquet and check for perfusion; inset the flap at the recipient site; wait for normal perfusion to occur; treat the skin graft donor site with a medium- or full-thickness skin graft; be careful when tunneling |
Advantages |
|
Tissue |
Sensate thin and pliable flap |
Vascular pedicle |
Reliable pedicle with a wide arc of rotation; large-caliber vessel when used as a free flap |
Flap size and shape |
Can cover large defects without sacrificing a proper digital artery |
Combinations |
Possible to include a tendon strip of the extensor indicis muscle; a bony segment of the second metacarpal may be a future option |
Disadvantages |
|
Pedicle |
Flap is often white during the first few minutes after opening the tourniquet; venous congestion may occur if the flap is passed through a tunnel to the recipient site |
Donor site morbidity |
Donor site is conspicuous at first but improves significantly over time |
Pearls and pitfalls |
|
Dissection |
Do not make arc of rotation too narrow, because venous congestion may occur; preserve the paratenon of the extensor tendons for perfect skin graft take at the donor site; when the tunnel for the flap seems too narrow, create a skin graft pedicle; apply leeches early when venous congestion occurs; avoid any tension on the pedicle; when the flap does not show adequate reperfusion after the opening of the tourniquet, rinse with warm saline; it may take 20 minutes to re-establish flow; include part of the sagittal band across the MP joint to protect the pedicle attached to the skin |
Extensions and combinations |
Bony segment from the metacarpal may be possible |
Contouring and correction |
Rarely required; flap shrinks with time |
Clinical applications |
Pedicle flap: small and medium-sized dorsal defects of the thumb; restoration of sensation of the pulp of the thumb
Free flap: small and medium-sized defects wherever local flaps are not possible or appropriate |