Flap |
|
Tissue |
Bone and skin paddle; bone, skin, and muscle flap |
Course of the vessels |
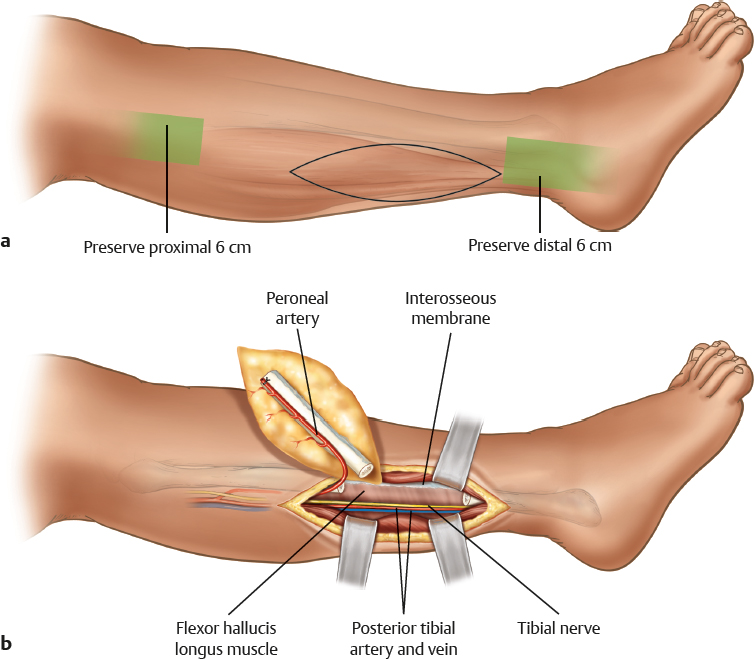
Posterior to the fibula, through or beneath the flexor hallucis muscle |
Dimensions |
Bone length, ≤ 26 cm; skin paddle 8 × 15 cm |
Extensions and combinations |
Parts of the soleus muscle can be included |
Anatomy |
|
Neurovascular pedicle |
– |
Artery |
Peroneal artery |
Veins |
Peroneal veins |
Length and arc of rotation |
2–4 cm |
Diameter |
Artery, 1.5–2.5 mm; vein, 2–4 mm |
Nerve |
– |
Surgical technique |
|
Preoperative examination and markings |
Draw a line from the fibula head to the lateral malleolus posterior to the peroneal tendons; mark the midpoint approximately 15.17 cm from the fibula head; identify skin perforators |
Patient position |
Supine, with a tourniquet on the thigh |
Dissection |
Lateral approach is preferred for both flaps; create the anterior incision of the designed skin paddle through the crural fascia to the peroneus muscles; make a subfascial dissection toward the posterior intermuscular septum; incise through the posterior margin of the skin paddle; make a subfascial dissection of the soleus muscle to the posterior intermuscular septum; the septum is traced to the fibula; the dissection proceeds anteriorly to detach the anterior septum from the fibula; the posterior dissection moves toward the flexor hallucis muscle; identify the vessels (a cuff of the flexor hallucis muscle may have to be incorporated); create a distal osteotomy (insert retractors close to the fibula to protect the vessels); the distal end of the fibula is distracted cephalad with a clamp; divide the interosseous membrane; expose the peroneal vessels; create a proximal osteotomy; trace the vessels back to the origin; open the tourniquet and check for perfusion |
Advantages |
|
Vascular pedicle |
Reliable, large-caliber vessels; loss of donor vessels is usually tolerable |
Flap size and shape |
Skin paddle is mobile; many defect variations can be reconstructed with a combined osteocutaneous flap; the fibula provides ideal bone for the replacement of the radius, ulna, and humerus |
Combinations |
Soleus muscle can be included to fill larger dead spaces |
Donor site |
Despite a slight torsion instability, donor morbidity is minimal if taken as a bone flap only |
Disadvantages |
|
Donor site morbidity |
Donor scar is conspicuous; risk of nerve injury to peroneal nerve or motor nerve of the flexor hallucis muscle; possible exposure of peroneal tendons |
Dissection |
Dissection is tedious and technically difficult; pedicle is short |
Flap |
Skin island may be too small in complex injuries with major soft tissue loss |
Pearls and pitfalls |
|
Dissection |
Do not confuse peroneal vessels with posterior tibial vessels; take a muscle cuff (1–2 mm) to ensure bone perfusion; preserve the proximal and distal 6 cm of the fibula to maintain stability; in children, the distal 10 cm should be preserved |
Extensions and combinations |
When part of the soleus muscle is included, be sure to include a muscle perforator, otherwise risk of muscle necrosis is high |
Contouring and correction |
Rarely required |
Clinical applications |
Complex segmental defects of the wrist, forearm, humerus, and shoulder (arthrodesis) |