Femoral Bone Debridement
Robert J. Steffner
David W. Lowenberg
Sahitya K. Denduluri
DEFINITION
Femoral bone debridement is generally needed for osteomyelitis (acute or chronic), symptomatic nonunion, and open fracture.
ANATOMY
The femur contributes to the hip and knee joints and withstands significant stress in motion.
Vital structures around the femur include the sciatic and femoral nerves, the superficial and deep femoral artery and vein, and the extensor mechanism for knee extension.
PATHOGENESIS
Open fracture leads to gross contamination, soft tissue stripping, and avascular bone. Direct inoculation occurs, which will lead to infection in the absence of prompt surgical care.
Hematogenous spread of bacteria to the bone can create osteomyelitis. Acute infection tends to produce rapid symptoms and the accumulation of purulent fluid. Chronic infection is more indolent and produces waxing and waning symptoms. After a week or two of infection, bacteria form a protective avascular matrix called biofilm. Antibiotics cannot penetrate this layer.
Nonunion is a fractured bone that will not heal. Hypertrophic nonunion comes from too much fracture site motion. Atrophic nonunion is from poor blood supply and inadequate substrate for bone healing. Infection can also lead to nonhealing bone and sometimes creates a false joint known as a pseudarthrosis.
In all of these instances, surgical debridement is required to promote bone recovery and healing.
NATURAL HISTORY
Neglected open fractures and osteomyelitis can lead to systemic infection and sepsis, which is life threatening.
Chronic infection can produce a nonhealing wound with drainage. This limits quality of life and can also lead to squamous cell carcinoma at areas of long-standing skin ulceration.1
Nonunion in the femur limits weight bearing and mobilization. Pain is often present with activity. Quality of life is significantly diminished.
PATIENT HISTORY AND PHYSICAL FINDINGS
Ask about prior trauma, surgical procedures, and any complications or wound healing problems.
Specifically ask about cellulitis and draining sinus tracts.
Assume infection until proven otherwise.
Assess impact on the patient’s quality of life.
Inquire about recent antibiotic use.
Determine host factors such as nutrition, nicotine use, medical comorbidities, use of immunosuppressive and antiinflammatory medications, and any prior radiation exposure to the area of interest.
Visually inspect the patient’s thigh. Look for deformity, leg length discrepancy, and rotational change from the contralateral side.
Lab work including WBC, ESR, and CRP can help determine the presence of infection.
IMAGING
Plain radiographs can demonstrate nonhealing bone, erosive cortical changes seen in acute infection, and sclerotic thickening seen in chronic infection (FIG 1).
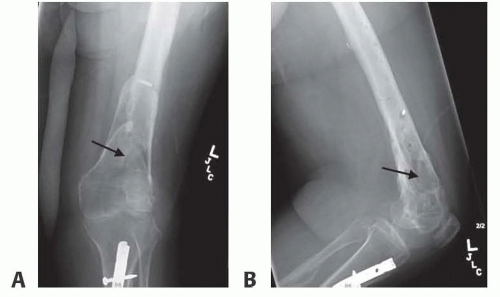
FIG 1 • A. AP and lateral (B) radiographs of a distal femur chronic osteomyelitis in the setting of prior internal fixation for an open distal femur fracture. Original hardware removed with exception of a broken screw. Radiolucent changes (arrows) seen in the metaphysis of a patient with clinical evidence of a draining sinus tract.
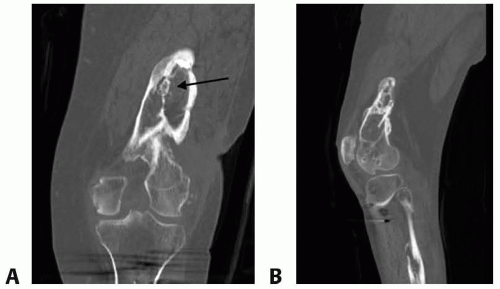
FIG 2 • A. Coronal and sagittal (B) CT scan of the distal femur with chronic osteomyelitis demonstrating sclerotic rim of the bone (involucrum) surrounding a spicule of the bone (sequestrum, arrow).
Full-length, weight-bearing radiographs of the lower extremities show deformity and leg length discrepancy.
CT scan is best for bony detail. It is the modality of choice to identify a nidus of dead bone (sequestrum) and surrounding sclerotic bone (involucrum) seen in chronic osteomyelitis (FIG 2).
MRI imaging assesses the level of intramedullary bone and soft tissue involvement with bone infections. This is crucial in determining the extent of surgical debridement.
NONOPERATIVE MANAGEMENT
Nonhealing bone and bone infection in the femur are almost always operative given the structural importance for weight bearing and ambulation.
Exceptions include low-demand patients with minimal symptoms, patients who adapt well with assist devices, and patients at high surgical risk due to medical comorbidities.
Nonunion patients without infection can try bracing and bone stimulation devices before surgery.
SURGICAL MANAGEMENT
It is important to set patient expectations. Several debridement procedures may be needed to create a favorable bone and soft tissue bed for reconstructing and healing. Persistent or recurrent nonunion or infection may happen despite aggressive surgical management.
Preoperative Planning
Address modifiable host factors including smoking cessation, nutrition, glycemic control, and medication use (antiinflammatories, corticosteroids, etc.).
In the lower extremity, quantify the degree of limb shortening, malalignment, and malrotation. Shortening greater than 2 cm and deformity greater than 10 degrees tend to limit a patient’s quality of life.Related posts:
 Fasciotomy of the Thigh, Lower Leg, and Foot
Fasciotomy of the Thigh, Lower Leg, and Foot
 Bony Reconstruction of Foot and Ankle (Bone Grafts)
Bony Reconstruction of Foot and Ankle (Bone Grafts)
 Vascular Reconstruction of Lower Extremity, Foot, and Ankle
Vascular Reconstruction of Lower Extremity, Foot, and Ankle
 Tibial Reconstruction
Tibial Reconstruction
 Reconstruction of Femur
Reconstruction of Femur
 Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation
Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


