FEMININE REJUVENATION
PART 3.8
FEMININE REJUVENATION
Susan F. Lin M.D.
448 N. San Mateo Drive
San Mateo CA 94401 USA
ABSTRACT
In this chapter we address head-on this rarely discussed substrate, in the best Harry’s Cosmeticology tradition.
As we have seen in many other chapters in this book, the perception of beauty and its relationship to well-being and skin health are intimately connected. Recent work in the cosmetic and personal care field has now extended beyond mere ingredients and formulations to other factors that provide an impact on beauty in the wider sense.
With the growing advent of dermatologists, OB-Gyn professionals, and other medical researchers formulating their own product lines, we deem it appropriate and timely for a detailed discussion of the anatomy, function, dysfunction, and approaches to improve the perception and well-being of individuals who want to feel and project beauty in their world.
While many may begin with the thought that this body substrate is more intended for medical/drug intervention, the reader will see there is much opportunity for the development of cosmetic-based over-the-counter, natural approaches that offer enhancement of this category and are both needed and wanted by the world’s female population.
3.8.2 Vulvar Innervations: Physiological and Analytical
3.8.3 Vulvar Atrophy: Causes and Physiology
a. Over-the-Counter Treatments
c. Novel stem-cell-derived peptides
Vulva includes female genital regions that are externally visible in the perineal region composed of mons veneris, labia majora, labia minora, and clitoris.
- ● Mons veneris, overlying the symphysis pubis, is the fatty prominence covered by curly hair.
- ● Labia majora are composed of two longitudinal folds of skin extending in elliptical fashion to enclose the vulvar cleft. Contain abundance of adipose tissue, sebaceous glands, and sweat glands. Embryologically analogous to penile shaft of male genitalia and the skin covered by hair on their upper outer surfaces.
- ● Labia minora are thin, firm, pigmented, redundant folds of skin, which split anteriorly to enclose the clitoris and meet posteriorly by the vestibules. Skin of labia minora does not contain hair follicles and is poor in sweat glands but rich in sebaceous glands.
- ● Clitoris is a small cylindrical erectile organ at lower border of symphysis. It is made up of two crura, body and glans. Crura lie deeply, in close apposition to peri-osteum of ischiopubic rami. They join to form the body of the clitoris, which extends downward beneath a loose prepuce to be capped by the acorn-shaped glans. Only the glans of the clitoris is visible externally between the two folds formed by bifurcation of labia minora. The visible clitoris is one to two inches in length. It is attached to the pubic bone and separates into two crura that are each about two to four inches in length. Clitoral hood acts as a shield for the clitoral glans. The role of the clitoral hood is to provide protection from too much stimulation.
3.8.2 VULVAR INNERVATIONS: PHYSIOLOGICAL AND ANALYTICAL
Vulva and perineum are innervated by femoral nerve posterior and lateral margins of vulva along leg crease. Genitofemoral and ilioinguinal nerve from L-1 and L-2 innervate the mons pubis upper labia majora to the level of urethra. Perineal branch of pudendal nerve (S-2–S-4) covers the lobes of labia majora. A rich plexus of over 8,000 nerve endings covers the dorsal aspect of the glans clitoris from the deeper pudendal nerve. The inferior cuneal nerve from S-1–S-3 also covers the vulva.
Assessing Sensory Perception on the Vulva and on Extragenital Sites
Sensory perception on the vulva as well as extragenital sites occurs by means of detection of transient light touch by Meissner corpuscles and transient deeper pressure by Pacini corpuscles. Slowly adapting receptors, such as Merkel cells and Ruffini receptors, are responsible in responding to more sustained touch, such as sensing texture or shape.
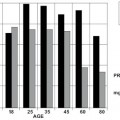
While perception of burning or itching appears to be unaffected with aging, vulvar sensitivity to mechanical stimuli declines after menopause.
However, of the various demographics (age, gender, ethnicity) and anthropometric variables (height, weight, size of the body), the most significant effect on sensory perception is advancing age. This is also true for sensitivity to vibration, thermal threshold, and mechanical stimuli. Ethnic differences in sensory perception also have been reported. For example, Japanese subjects were more sensitive to touch and pain on the cheeks and palm of hands than Caucasians. However, Japanese subjects rated pain as less severe on a subjective scale than Caucasians—despite being more sensitive at perceiving it. Cultural stoicism may have contributed to higher tolerance to pain (1).
A Canadian study of 40 premenopausal women found that the labium minora and the mucosa of the vulvar vestibule were less sensitive than the forearm to filament touch and pressure. Although the labium minora was more sensitive to pain than forearm (2), similarly, a study of 13 premenopausal women found vulvar vestibule to be less sensitive to filament touch and pressure than deltoid muscle, forearm, or thigh (3).
A Swedish study found the clitoris to be less sensitive to perception of vibration than dorsum of hand but more sensitive than dorsum of the feet (4).
A Turkish study on vibratory threshold found vulvar sites (labia majora and minora, clitoris and vaginal introitus) were comparable in sensitivity to the first and second fingers and to the nipples. In this study, lips and ears were the least sensitive to vibratory stimuli (5).
A study conducted in the USA of both healthy and neurologically impaired women (6) noted significant loss of sensitivity to pressure/touch in postmenopausal women, hypo-estrogenic women, women with vulvar atrophy, neurologically impaired women, and women with impaired sexual function, all of whom showed clear effect of estrogen on vulvar sensitivity. Although vulva has lower density of estrogen receptors than vagina, the effect of estrogen on touch sensitivity appears profound (7). Estradiol treatment significantly increased sensitivity of vestibule to pressure/touch relative to placebo at four to six weeks. Although the mechanism of action is not known at this time, the potential sensor neural targets may be C fibers of Merkel cells (8).
In a Canadian study of premenopausal women aged 18–45, it was found that sexual arousal had no effect on extragenital sensations, suggesting dyspareunia is not due to lack of arousal (9).
Thresholds to touch averaged over all vulvar sites (clitoris, labium minus, perineum, and anal verge) were noted to be 4.6-fold lower in normoestrogenic compared to hypoestrogenic women (10).
Because of the importance of sensation to female sexual well-being and the perception and projection of beauty, in its broadest sense, an objective of an appropriate vulvar skin regimen should include the maintenance of vulvar sensorium by preserving nerve sensitivity functions.
3.8.3 VULVAR ATROPHY: CAUSES AND PHYSIOLOGY
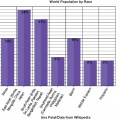
In the U.S., half of the population is expected to be over the age of 50 in the next 20 years. There is a misconception that skin disorder is only cosmetic. Because physiological changes occur with skin, if the causes are left untreated, such disorders can lead to a vicious cycle of chronic irritation and pruritis. These changes affect sexual function, comfort, and self-esteem.
Common physiological changes with age include:
lower elasticity and diminished tensile strength,
reduceda dermal thickness,
reduced vascularity and cellularity of dermis,
decreased sensory perception,
reduced hydration,
flattening of the dermal-epidermal junction,
reduced epidermal thickness,
increased permeability, and
slower wound healing.
An awareness of these facts will bring a new pathway to individuals and companies looking for new products, new categories, and a common wish to enhance all aspects of individual beauty. The intention here is to expedite work in this area beyond the medical/drug approaches already in existence and to include the development, use, and application of cosmeceuticals, natural products, etc. that are having a positive impact on beauty enhancement.
Skin changes can be slow and progressive with loss of subcutaneous fat beneath
Related posts:
 – AN OVERVIEW OF THE CHANGING REGULATORY LANDSCAPE IN THE U.S. AND THE E.U. AND HOW TO DEAL WITH THEM…
– AN OVERVIEW OF THE CHANGING REGULATORY LANDSCAPE IN THE U.S. AND THE E.U. AND HOW TO DEAL WITH THEM…
 3 – THE SUBSTRATES
3 – THE SUBSTRATES
 – AN OVERVIEW OF HAIR FOLLICLE ANATOMY AND BIOLOGY
– AN OVERVIEW OF HAIR FOLLICLE ANATOMY AND BIOLOGY
 – CLASSIFICATION SCALE FOR SKIN COMPLEXIONS AROUND THE WORLD
– CLASSIFICATION SCALE FOR SKIN COMPLEXIONS AROUND THE WORLD
 – HAIR AGING: FUNDAMENTALS, PROTECTION AND REPAIR
– HAIR AGING: FUNDAMENTALS, PROTECTION AND REPAIR
 – MECHANISMS OF CHANGES IN HAIR SHAPE
– MECHANISMS OF CHANGES IN HAIR SHAPE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


