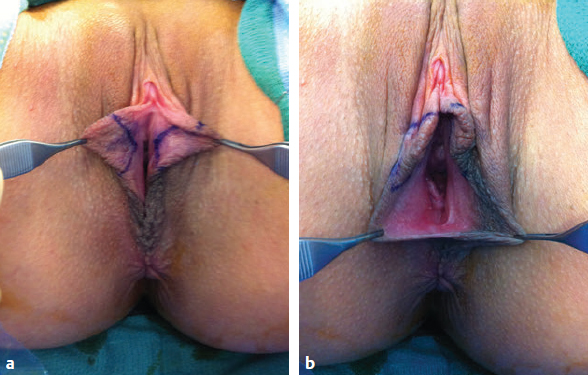
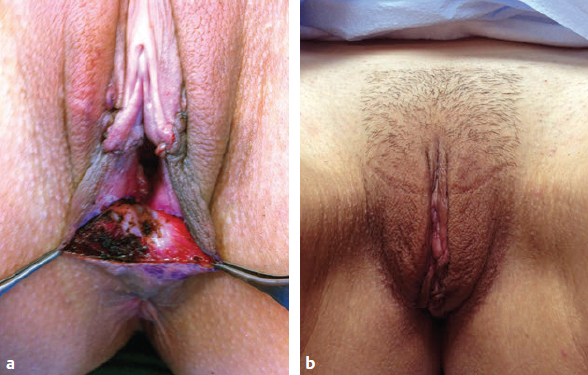
CHAPTER In recent years, women have been increasingly seeking aesthetic genital surgery.1,2 One possible explanation for this trend sources from the media highlighting an idealistic form of the female genitalia: hairless and symmetrical with non-visible labia minora. Although aesthetic modification is the most common motivation, women seek genital surgery for a variety reasons, including functionality, discomfort, chafing, and impaired sexual pleasure.3–6 Regardless of the reason, the increased demand in female aesthetic genital surgery warrants detailed attention to surgical techniques, complications, and prophylactic precautions. Thus far, outcomes have generally been favorable, with most series reporting high patient satisfaction and low rates of complications.6–9 Summary Box Common Complications When Performing Female Aesthetic Genital Procedures Preoperative patient counseling is essential in aesthetic genital surgery. Surgeons need to educate patients in the normal variations of female genitalia and discuss both the risks and benefits of each procedure to endorse informed decisions with realistic expectations. For example, a patient desiring complete amputation of the labia minora should be informed of these structures’ importance in normal micturition as well as lubrication and should be discouraged from pursuing such an extreme procedure. The physician also needs to oversee that the patient’s decisions are made autonomously and not through coercion. To ensure this, surgeons need to be cognizant of common “red flags,” such as friends and family members who display intrusive behavior and seem overly concerned with the surgical details and outcomes. Mothers to teenage patients are an exception and may display this level of involvement without warranted concern.9 Because patients with body dysmorphia tend to not benefit from cosmetic procedures, it is imperative to screen for this disorder before surgery. Any underlying pelvic floor or urinary conditions must also be screened for so that they are treated preoperatively and the increased risk of complications is avoided.10 Assessing preoperative sexual function should be a component of the preliminary consultation. Although some data suggest that aesthetic genital surgery can improve sexual function and satisfaction,6 it must be determined whether the underlying cause of dysfunction is psychological, hormonal, or anatomic. If a psychological cause is suspected, it is important to inform the patient that aesthetic surgical modifications have the potential to increase confidence and in turn improve one’s sexual experience.11 The patient must also be informed that the dissatisfaction is unlikely due to any anatomic abnormalities and that surgery may not be the solution to these needs. Counseling patients in this fashion allows them to make an informed decision and form more realistic expectations before surgical intervention. Standardized photographs of the patient should be taken in both standing and lithotomy positions during preoperative planning. These are useful to review with the patient before surgery to discuss any preexisting asymmetry and the anticipated scar location.11 Wound-healing complication rates are higher in those who smoke, are overweight, or have diabetes.11 Therefore smoking cessation, weight loss, and medical optimization of comorbidities are encouraged before surgery. It is imperative for patients not to smoke for at least 4 weeks before surgery. All patients should be counseled to rest for 3 to 5 days following surgery to prevent hematoma and postoperative swelling.11 In addition, patients should be discouraged from resumption of sexual intercourse until reevaluation at their postoperative visit. In general, complications related to female aesthetic genital surgery are low, with most studies reporting a prevalence of 5% or less.10,12 Specific procedures in genital aes thetic surgery are discussed in the following sections with a focus on their accompanying complications, ways to avoid these complications, and management strategies for when complications arise. A mons pubis lift corrects mons pubis ptosis by a low transverse suprapubic incision, similar to that used in abdominoplasty. The goal is to create a youthful contour to the junction between the mons and the lower abdomen. Therefore the incision must extend far enough laterally to give a natural triangular appearance to the mons. To achieve a successful mons lift, both excess pubic skin and fat must be removed. The fibrofatty tissue of the pubic skin flap should be resuspended to the anterior rectus sheath fascia as well.13 If the mons pubis lift is to be performed with concomitant abdominoplasty, any planned labia majora reduction should then be delayed, because a pubic lift can cause increased labia major swelling. To avoid complications and revisions, overresection of mons fat should be avoided, because it can cause an unnatural appearance such as contour irregularities, and the closure of the defect must be tension-free to avoid elevating the intervulvar cleft and clitoris.9,11 In addition, careful attention must be paid to the dorsal clitoral nerves so that they are not injured during the resection. The goal of labia majora resection is to eliminate excess skin or tissue from the outer labia while avoiding overreduction. Primary labia majora hypertrophy causing tissue excess must be distinguished from secondary labia major hypertrophy resulting from volume loss leading to skin excess. This delineation determines the appropriate technique for correction. Volume excess can be treated by full-thickness reduction with debulking, but care should be taken not to remove too much tissue, which can create sagging and excess skin.14,15 Excess skin can be removed using a longitudinal wedge excision. To avoid transfer of hair-bearing skin medially and secondary irritation, the incision should be placed on the lateral aspect of the labia majora skin and the smooth skin of the intervulvar cleft.16 Excessive resection can lead to exposure of the vagina and can be avoided by continuous reassessment of the labial flap in the position of inset. The scar in labia majora resection is long and visible, underscoring the importance of both appropriate incision planning and tension-free closure. In addition to overreduction causing scar hypertrophy, complications of this procedure are hematoma and transient hypersensitivity for 4 to 6 weeks.16 Hematomas tend to form because the large vessels of the labia majora retract into the fatty tissue during resection, making them difficult to cauterize. If a hematoma forms it must be drained quickly in the operating room under general anesthesia.16 Use of passive drainage may also be appropriate in select patients. The purpose of volume augmentation is to counteract the deflation of the mons pubis and labia majora that can occur after weight loss or hormonal changes. Facial fillers such as calcium hydroxyapatite and hyaluronic acid can be used, but large amounts are often required, which can be cost prohibitive. Fat transfer using lipoinjection or dermal fat grafts can be used as an alternative (Video 33.1).17 Fat can be harvested from the abdomen, flank, or thighs, and 10 to 50 cc can be injected in each labia majora, although the definitive end point ultimately relies on aesthetic judgment. Fat can also be injected into the mons pubis if this region appears deflated. It is important to overfill the areas by 20 to 30% to allow for fat resorption, which is a known consequence of fat grafting. Lipoinjection can cause palpable fatty cysts to form or create contour irregularities.18 Therefore it is reasonable to consider dermal fat grafting as an alternative, particularly if an abdominoplasty is performed concurrently, because the dermal fat can be harvested from the resected specimen and has been reported in the literature to have increased graft survival.19 Surgical reduction of the labia minora is the most common female aesthetic genital procedure and thus has the most options for surgical technique.1,2,16 The optimal technique should be selected based on the amount and anatomic location of tissue requiring resection as well as surgeon comfort. Edge-trim techniques, in which the labia minora are resected and the epithelial edges reapproximated, were the first techniques described and are useful for selectively trimming areas of tissue redundancy. Complications related to direct excision include scar contracture (potentially causing a tight introitus and suture dehiscence), wound infection, and stiff, painful scars that can cause local irritation and pain with ambulation.20,21 Keeping the incision out of the posterior fourchette can prevent postoperative dyspareunia caused by scar contracture in the introitus.22 Asymmetry and scalloping of the labial edges are also potential concerns.21 To prevent scar contraction, a nonlinear incision such as the “lazy S” introduced by Felicio or the W modification developed by Maas and Hage can be used.22 Avoiding interrupted sutures at the labial edge can also help to preserve a natural appearance.23 Running, absorbable suture is a good choice for the closure.11 Felicio’s lazy S incision is intended to maintain the natural asymmetry of women’s labia.24 However, many women desire symmetry when seeking genital surgery, and if this technique is to be used, it should be discussed with the patient in advance. The edge-trim technique may also not be ideal for patients who are interested in preserving the natural color of the labial edge. Fig. 33.1 Overreduced labia minora after labiaplasty. Documented complications of direct excision techniques include hematoma, wound dehiscence, and overexcision24 (Fig. 33.1). Small hematomas will likely drain spontaneously, but if they do not they should be drained in the operating room promptly. Wound dehiscence can often be managed by allowing for secondary intention. Overexcision is often irreversible because of resultant tissue deficit. However, an island clitoral hood flap that is vascularized randomly based on dartos muliebris fascia of the lower clitoral hood and medial labium majus can be transposed to the labial defect.23 Avoiding lateral tension during reduction is imperative to prevent overresection. Patient selection is also important. Other deformities that do not involve overresection can often be reconstructed with wedge excisions, labial Y-V advancements, and touch-up trimming.23 In general, individuals with prominent clitoral hoods are not ideal candidates for the direct excision technique, and another method should be undertaken.11 Alter22 first described the wedge resection technique in 1998 as an alternative to direct excision to preserve the labial edge and avoid chronic scar tenderness. The original technique involved a V-shaped central wedge resection. One modification of the technique added two z-plasties to reduce the deformity at the free border and create a tensionless suture line by interdigitating two rectangular flaps. This serves to avoid wound dehiscence and potential tightening of the introitus.25 To minimize introital constriction, the vagina should accommodate two fingers, without excessive tension on the incision closure.9 Alter eventually updated his technique to include the addition of an anterior, hockey-stick resection to excise lateral clitoral hood excess.9 Other variations include the star labiaplasty, which includes a vertical V resection with horizontal wedge resection, and the inferior wedge resection with superior pedicle flap.26 Fig. 33.2 (a) Markings for wedge resection labiaplasty. (b) Resection includes the posterior fourchette with perineoplasty to prevent entry dyspareunia postoperatively. Intraoperative use of local anesthesia (1% lidocaine with 1:100,000 epinephrine) is beneficial for vasoconstriction and hydrodissection of the subcutaneous space between the lateral and medial skin layers of the labia. This facilitates tissue resection and placement of skin sutures. It is important to mark the proposed site of surgical incisions before the injection of the anesthetic. Proper closure of the wedge defect, which is often created centrally, is important for an optimal aesthetic result. Monofilament absorbable sutures on a tapered needle should be used to close the defect followed by interrupted or running absorbable Vicryl or monofilament sutures for the mucosal layer. To avoid notching of the free edge of the labia minora, the edges of the mucosa can be everted distally and closed with a 5–0 Monocryl suture using the vertical mattress technique. If a patient has thin, atrophic labia minora, the wedge should be demucosalized rather than resected in a full-thickness fashion.11 The main complication of wedge labiaplasty is wound dehiscence, particularly when taken from the inferior edge.9,22,26–28 The blood supply of the labia is variable, and the tension imposed on the outwardly pulled edges can result in improper healing. To prevent wound dehiscence and fistula formation it is important to preserve as much subcutaneous tissue as possible and precisely reapproximate the wound edges. The subcutaneous tissue should be closed in one or two layers and the labium reapproximated and closed in three layers with 4–0 and 5–0 absorbable sutures. Using an atraumatic, noncutting needle is also helpful in preventing tissue damage during reapproximation. Other complications, albeit rare, include labium fistula, hematoma, dyspareunia, and clitoral hood “dog-ears.” Dog-ear deformities can be avoided by incorporating the hockey-stick resection described by Alter.23,26,29 To avoid dyspareunia, the labial resection should not be extended to the posterior fourchette, and labial width should be kept to at least 1 cm so that the labia will protrude past the introitus (Fig. 33.2).17 Fig. 33.3 Vulvar agglutination after wedge resection labiaplasty. Loss of a smooth pigment transition zone is another possible complication, but unfortunately this may be unavoidable in some patients. Discussing this preoperatively with patients is important. If an aesthetic pigment transition is not possible with a wedge technique, an edge-trim technique may be a better option.11 Another postoperative complication of labiaplasty is vulvar agglutination, which can be treated with an estrogen-derived cream (Fig. 33.3). Fig. 33.4 (a) Diamond-shaped wedge excision. (b) One year after diamond-shaped perineoplasty and central wedge resection labiaplasty. Labiaplasties performed using the inferior wedge resection technique in conjunction with transposition of a superiorly based flap are particularly susceptible to skin tip necrosis, as previously stated.27,29 This will typically heal secondarily, but it is important to avoid aggressive undermining and hemostasis that can compromise the vascular supply of the flap.29 The inferior wedge technique is used less often in the United States because of the increased wound dehiscence rates. The only technique that completely respects the labial edge and avoids violation is the deepithelialization technique described by Choi and Kim.29 In this method, both the medial and lateral sides of the labia are marked to identify areas of hypertrophy located centrally and are subsequently deepithelialized with either a scalpel or laser. This technique is best for patients with very little hypertrophy (approximately 2–3 cm from baseline).29 Otherwise the surgeon runs the risk of leaving behind too much tissue, resulting in a bulky labium and poor aesthetic outcome. In addition to residual tissue redundancy, poor outcomes can result from wound dehiscence and abrupt color change at the suture line.17 The primary goal of clitoral hoodectomy is to remove redundant or hypertrophic clitoral hood tissue.6 The location of excess tissue determines the ideal technique for resection. Excess tissue in the sagittal plane, appearing as a wrinkled clitoral hood, can be resected with an inverted-V curvilinear approach. Widened clitoral hoods with excess lateral tissue can be reduced with triangular excisions along the lateral borders of the clitoral hood. With these excisional techniques, the primary concern is the depth of the excision, which must be kept superficial to avoid the dorsal clitoral nerve located deep to the investing fascia of the clitoris.11 If labial hypertrophy is also present, the clitoral hood resection can be combined with a wedge resection labiaplasty. This technique also protects the dorsal nerve of the clitoris. Alter’s hockey stick modification to his central wedge resection technique23 addresses redundant clitoral tissue. If the hypertrophic tissue is more medial, a vertical medial ellipse resection can be used instead of the lateral hockey stick. Clitoral hood tissue can be closed with 5–0 Monocryl in the subcutaneous tissue and a subcuticular Monocryl skin closure.8 Some suggest using Vicryl sutures, instead of monofilament, in the areas closest to the clitoris to minimize postoperative irritation and pain.30 Complications associated with clitoral hood resection are wound dehiscence, clitoral hood dog-ears, clitoral hypersensitivity, and suture granuloma.9,32 Care should also be taken to limit scar formation that may cause hypersensitivity, in addition to vigorous closure resulting in damage to the clitoris.14 It is also important to make the patient aware that in the case of combined procedures, healing time is prolonged and swelling and discomfort may persist for several weeks.11,24 The goal of perineoplasty is to reconstruct the vaginal introitus with a minor low-posterior compartment repair. Reapproximation of the levator ani muscles is also performed and is important to strengthen the resulting perineal body and elevate the perineum. A diamond-shaped wedge technique is used (Fig. 33.4). The primary complication of perineoplasty is overcorrection resulting in perineal constriction.17 To avoid this, a dilator can be inserted into the vagina intraoperatively to ensure that it can be inserted distal to the introitus without much resistance. Vaginal dilators can also be used postoperatively to resolve perineal constriction with stretching. Perineoplasty will only be successful if the underlying pelvic floor’s muscle strength and function are intact. Training by a pelvic floor physical therapist has been associated with improved long-term outcomes of perineoplasty.6 The goal of vaginoplasty is to tighten the vagina by reconstructing the lateral wall segment. This is generally performed by excising and primarily closing mucosa and muscle at each vaginal fornix. Lateral colporrhaphy is the most commonly used technique when reducing the size of the vagina is the primary operative goal. This technique avoids placing scars in areas of high sensitivity, which causes less postoperative dyspareunia.17 In addition to lateral colporrhaphy, posterior vaginal epithelium can be dissected and trimmed to an appropriate diameter and rectovaginal muscles can be plicated. Occasionally levator ani muscles may be plicated, but this may cause significant dyspareunia and is not recommended in isolated aesthetic cases.10 Reported complications of vaginoplasty by colporrhaphy include wound dehiscence, local infection, de novo in continence, postoperative vaginal bleeding, and dyspareunia resulting from vaginal apex stricture. There has been one reported case of rectal entry when performing combined vaginoplasty and perineoplasty. If this occurs, immediate identification and closure of the defect should be performed.6,10 Other methods of vaginal tightening have recently emerged, including the use of autologous fat grafting or bulking agents such as hyaluronic acid. These have their limitations, however, because hyaluronic acids get resorbed and only provide temporary improvement, whereas the long-term viability of grafted fat is variable.17 Occasionally foreign body injections to the proposed G-spot are also performed, despite poorly demonstrated safety and efficacy, and these have led to significant complications.31 The growing popularity of female aesthetic genital surgery has been accompanied by the advent of many procedures and techniques. To achieve optimal aesthetic outcomes, it is imperative that the surgeon be able to determine the most appropriate procedure given the patient’s anatomy and to approach each in a manner to minimize complications and manage any that should arise. 2 American Society of Aesthetic Plastic Surgery. Labiaplasty and buttock augmentation show marked increase in popularity, 2014, http://www.surgery.org/media/news-releases/labiaplasty-and-buttock-augmentation-show-marked-increase-in-popularity 12 Guo S, Dipietro LA. Factors affecting wound healing. J Dent Res 2010;89(3):219–229 13 Goodman MP. Female genital cosmetic and plastic surgery: a review. J Sex Med 2011;8(6):1813–1825 21 Alter GJ. A new technique for aesthetic labia minora reduction. Ann Plast Surg 1998;40(3):287–290 23 Felicio YdeA. Labial surgery. Aesthet Surg J 2007;27(3):322–328 31 Gress S. Composite reduction labiaplasty. Aesthetic Plast Surg 2013;37(4):674–683
33
Female Aesthetic Genital Surgery
Avoiding and Managing Unfavorable Results and Complications in Female Aesthetic Genital Surgery
Preoperative Planning and Patient Selection
Surgical Techniques
Mons Pubis Lift
Labia Majora
Labia Majora Resection
Labia Majora Augmentation
Labia Minora
Edge-Trim Labiaplasty

Wedge Resection Labiaplasty

Deepithelialization Labiaplasty
Clitoral Hood Resection
Perineoplasty
Vaginoplasty
Conclusion
References
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


