4
Felons
Sam Moghtaderi and Kevin D. Plancher
History and Clinical Presentation
A 15-year-old, left-hand dominant boy with insulin-dependent diabetes mellitus who monitors his blood glucose via multiple daily finger sticks presented to his physician complaining of extreme throbbing pain of his right middle fingertip for the past 24 hours.
Physical Examination
Examination of the affected finger demonstrated the volar aspect of the tip to be swollen, hard, and erythematous. The distal phalanx was extremely tender and somewhat fluctuant, but there was no pain in the distal interphalangeal joint or the more proximal regions of the finger. The dorsum of the phalanx, including the nail and periungual areas, appeared normal.
Diagnostic Studies
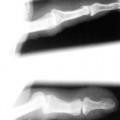
Anteroposterior and lateral plain film radiographs of the finger were obtained and demonstrated no abnormal findings.
PEARLS
- Often history of skin-penetrating injury
- “Throbbing pain” keeps patient from sleeping
- Conservative therapy effective for cellulitis—before the onset of pain
- Gram-negative coverage is essential in empiric antibiotic treatment of diabetics and immunocompromised patients
- Immobilization for first 48 hours, then active ROM exercises at dressing changes
PITFALLS
- Best routine incision is controversial
- In subcutaneous dissection, must avoid approaching the flexor tendon sheath
- Multitude of complications for neglected felon
Differential Diagnosis
Cellulitis
Flexor tenosynovitis
Herpetic whitlow
Metastatic tumor
Diagnosis
Felon of the Right Middle Finger
A felon is a bacterial infection of the distal pulp space of the fingers or thumb. As first described by Kanavel, the anatomy of the distal phalanx is unique, with the volar pulp space a confined sac, and fine fibrous septa connecting the subcutaneous layer to the bone (Fig. 4–1). An abscess in this region can lead to tensioning of the fibrous strands, increased pressure within the pulp space, and essentially a compartment syndrome with neurovascular compromise. In this way, a felon is distinguished from a simple superficial cellulitis, which may precede it. The patient with a felon presents with a swollen, hard, fluctuant, and erythematous fingertip, typically complaining of a throbbing pain so severe that it has kept him from sleeping.
There is usually a history of some penetrating trauma to the fingertip, which served as the inoculating event (splinter, broken glass, etc.), although it may have been rather inconsequential and forgotten by the patient. It is also possible that the organisms entered in retrograde fashion via the eccrine or sebaceous glands in the finger pad. Although diabetics and immunocompromised patients are generally at higher risk for hand infections, those who require routine blood monitoring via finger sticks have an additional risk for inoculating so-called finger stick felons. Skin flora comprises the organisms commonly seen in felons, and most often it is Staphylococcus aureus or other gram-positive organisms.

Figure 4–1
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


