CHAPTER 26 Fat Injections
Key Points
Introduction
Autologous fat transplantation is one of the promising cosmetic treatments for facial rejuvenation and soft-tissue augmentation due to the lack of an incisional scar and complications associated with foreign materials. However, certain problems remain, such as unpredictability and a low rate of graft survival due to partial necrosis. It has also been used in breast augmentation by a limited number of plastic surgeons,1 although the use of autologous fat for breast augmentation has been controversial due to the lack of consensus on whether it is safe and appropriate because of microcalcifications that may cause confusion in the evaluation of mammograms.
Implantation of prostheses has been a gold standard for breast augmentation, but complications with artificial materials such as capsular contracture remain to be resolved. The presence of the implant and capsules induced by implants could also affect breast tissue visualization in the mammogram.2 Furthermore, there is potential for rupture when pressure is exerted on the implant during mammography, and for this reason, hospitals in Japan reject women with breast implants to undergo mammography as a part of the annual social health examinations. Recently, autologous fat injection has been re-evaluated as a potential alternative to artificial implants for breast augmentation.1,3 This re-evaluation may reflect recent advances in autologous fat transfer and the radiological detection of breast cancer.
In this chapter, potentials of fat injection for breast augmentation or reconstruction are discussed as well as our novel approach of autologous fat grafting called cell-assisted lipotransfer (CAL);3,4 this is the concurrent transplantation of aspirated fat tissue and adipose progenitor cells.
Patient Selection
There are several patient factors that may affect the clinical result of conventional lipoinjection or CAL: skin redundancy of the breasts, age, body mass index (BMI), individual quality or character of the fat tissue, adhesive scars, breast implant and its capsule, systemic disease such as autoimmune disease, oral corticosteroids, etc.3,5 Good candidates are those who have sufficient fat at donor sites and redundant breast skin with healthy vascularity and without any scars.
Indications
Graft tissue preparations
As for lipoinjection, we use conventional lipoinjection (micro-fat grafting) and a new technique; grafting of progenitor-enriched adipose tissue. We call the latter CAL; the concept and details of CAL are described later. There are two types of CAL: mini-CAL and full-CAL; only the fluid portion of liposuction aspirates are used for harvesting adipose progenitor cells in mini-CAL, while another similar volume of liposuction aspirates to graft tissues are used for the cell isolation in full-CAL (Fig. 26.1). Thus, full-CAL requires twice the volume of adipose tissue as the conventional lipoinjection or mini-CAL; approximately 700–800 ml of lipoaspirate are needed for conventional lipoinjection or mini-CAL for both breasts, while 1200–1500 ml lipoaspirate are required for the full-CAL procedure.
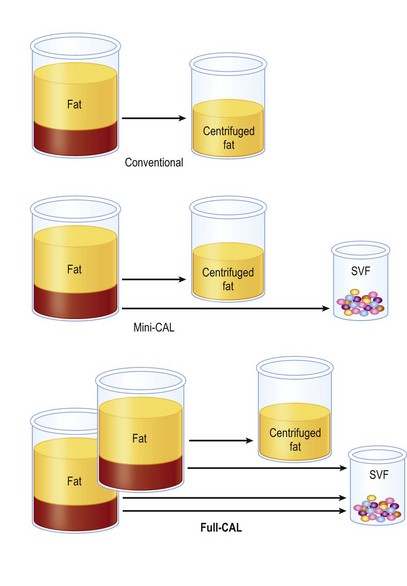
Fig. 26.1 Scheme of conventional lipoinjection and cell-assisted lipotransfer (CAL).
The adipose portion (yellow) of liposuction aspirates is centrifuged and used as injection material in conventional lipoinjection. In mini-CAL, the fluid portion (pink) of the liposuction aspirate is used for the isolation of the stromal vascular fraction (SVF) containing adipose progenitor cells. In full-CAL, another volume of liposuction aspirate is additionally harvested for SVF isolation. Freshly isolated SVF are used for supplementation of adipose progenitor cells to grafting tissues. (For the supplementation of SVF, see also Figure 26.5.)
Operative purposes
Injection of progenitor-enriched fat tissue: principles and therapeutic concepts of CAL
Cell components of adipose tissue
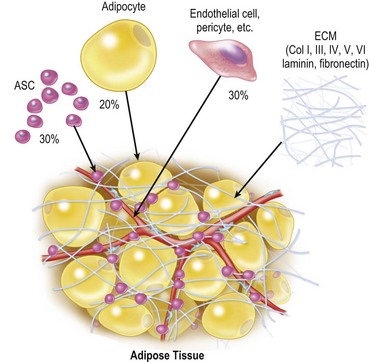
Adipose tissue consists predominantly of adipocytes, adipose stromal cells (ASC), vascular endothelial cells, pericytes, fibroblasts and extracellular matrix.6 Adipocytes constitute more than 90% of tissue volume, but they are much larger in size than the other cells and the number of adipocytes is estimated to be less than 50%7 (Fig. 26.2). ASC are considered to be adipose tissue-specific progenitor cells (adipogenic and angiogenic progenitors), some of which have been shown to differentiate into multiple lineages and are now called adipose-derived stem cells.8 ASC contribute to adipose tissue turnover (adipose tissue is thought to turn over every 2–10 years9,10) and provide cells for the next generation. ASC are currently being used in various clinical trials, including treatments for rectovaginal fistula (autologous cultured ASC)11 and graft-versus-host disease (non-autologous ASC).12 If ASC are harvested from a large volume (e.g., 500 ml) of liposuction aspirates, ASC can be used clinically without cell expansion because a sufficient number of cells can be obtained. The use of minimally manipulated fresh cells may lead to higher safety and efficacy in actual treatments.
Aspirated fat tissue versus intact fat tissue
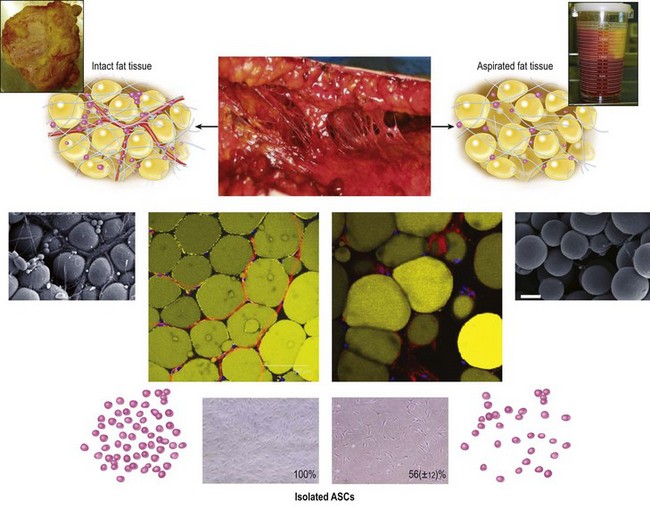
We can use aspirated fat tissue as lipoinjection material but not excised fat tissue. Aspirated fat is fragile parts of the adipose tissue taken with negative pressure. Our research revealed that aspirated fat tissue contains only half the number of ASC compared to intact fat tissue4 (Fig. 26.3). The two main reasons for this relative deficiency of ASC contained in aspirated fat tissue are: (1) a major portion of ASC are located around large vessels (within the tunica adventitia) and left in the donor tissue, and (2) some ASC are released into the fluid portion of liposuction aspirates.6 Our histological study indicated that ASC are located not only between adipocytes but also around vessels. Large-sized vessels are located in the fibrous part of the tissue, which contains intact fat tissue but not aspirated fat tissue. Thus, aspirated fat tissue is regarded as relatively progenitor-poor fat tissue compared to intact fat tissue.4
Stromal vascular fraction
Through collagenase digestion a heterogeneous cell mixture, which contains cell types other than adipocytes, can be extracted from adipose tissue as a cell pellet. This cell fraction is called the stromal vascular fraction (SVF) (Fig. 26.4), because they are basically stromal cells and contain vascular endothelial and mural cells. In the clinical setting SVF contains a substantial amount of blood-derived cells, such as leukocytes and erythrocytes, as well as adipose-derived cells such as ASC and vascular endothelial cells.6 Our study revealed that nucleate cells contained in the SVF are composed of 37% leukocytes, 35% ASC, 15% endothelial cells and other cells, though the percentage of blood-derived cells strongly depends on individual hemorrhage volume.7
Related posts:
 Gluteal Flap Breast Reconstruction
Gluteal Flap Breast Reconstruction
 The Central Septum in Breast Reduction and Mastopexy
The Central Septum in Breast Reduction and Mastopexy
 Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
Superior and Medial Pedicle Breast Reduction Using a Vertical Pattern
 Autologous Flap Use in Breast Reshaping after Massive Weight Loss
Autologous Flap Use in Breast Reshaping after Massive Weight Loss
 Fat Injections to the Breast: The Lipomodeling Technique
Fat Injections to the Breast: The Lipomodeling Technique
 Subfascial Breast Augmentation
Subfascial Breast Augmentation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


