14 Fat Grafting Abstract Fat grafting is an excellent approach as a natural filler in aesthetic and reconstructive surgery, with the advantage of producing a permanent, natural-looking result. The main downside of fat grafting however is the unpredictability of the final volume due to resorption of the fat graft. The surgical technique for fat harvesting, processing and injecting should be standardized as stated by Coleman, and the fat graft should be handled with delicacy at every step of the process in order to improve the final result. In reconstructive surgery, fat grafting has been used to improve contour and symmetry after trauma or tumor resection, among others, while in aesthetic surgery it has been widely used to correct the loss of facial volume due to aging as well as for breast and gluteal augmentation. Keywords: Fat, grafting, lipofilling, lipografting, Coleman technique Autologous fat grafting is the transfer of adipose tissue to a recipient site without its vascular support. It is widely used as natural filler in both reconstructive and aesthetic surgery, due to its versatility, availability, and natural results, in contrast with alloplastic fillers. Autologous fat grafting has proven that is the best method with which to increase subcutaneous tissue and to permanently correct contour deformities. However, the main problem with this method is the variability of the results due to the unpredictable loss of graft volume. Neuber described the first autologous fat graft in humans in 1893 when he first used it to reconstruct a tuberculous osteitis sequelae of the face with small grafts of subcutaneous tissue from the patient’s upper arm. In 1895 Czerny reported the first case of breast reconstruction utilizing a fat graft. Thereafter, surgeons used autologous fat grafting for many purposes; however, because of the variability and unpredictability of the initial results, the technique was largely abandoned until Illouz introduced liposuction, which opened the gate to modern fat grafting. In the mid-1990s, and thanks to the renewed interest in fat grafting, Coleman standardized the technique and proved the long-term stability of the graft. Recent advances in fat grafting indicate not only its capability for volume augmentation but also a potential regenerative effect due to the transfer of stem cells within the graft. According to the American Society of Plastic Surgery’s report in 2016 a total of 79.208 grafts were made in the United States, representing a 21% increase with respect to the year 2000. Adipose tissue is composed of three main elements: (1) the adipose cell, or adipocyte; (2) its precursor, the preadipocyte; and (3) the stromal vascular cells, including fibroblasts, immune cells, collagen fibers, and blood vessels. The extracellular matrix forms the fat lobules in adipose tissue. There are mainly two types of adipose tissue: brown fat and white fat. The fat in the adult human body is mainly white fat, which is the focus of this chapter. Adipocytes are cells with a single large vacuole filled with lipids inside and a peripherally located nucleus. In contrast, preadipocytes resemble fibroblasts. As they differentiate into adipocytes, the expression of collagen I and III decreases, and the production of collagen IV, glycosaminoglycans, and other compounds increases. As the harvested fat is transplanted to the recipient site, it survives by diffusion until approximately day 4, when the process of neovascularization begins. During the process, and because of mechanisms not fully elucidated, some adipocytes undergo apoptosis, which partly determines the unpredictable graft loss ( Also, adipose tissue contains a reservoir of mesenchymal stem cells within the stroma of the tissue. These stem cells are transplanted to the recipient site along with the rest of the fat graft’s cells. In 1997, Rigotti reported successful outcomes for managing radiodermatitis with fat grafting, explained by the regenerative potential of the stem cell population contained within the transplanted adipose tissue. Fig. 14.1 Evolution of two adipose cells after lipoinjection. For unknown reasons some fat cells activate an apoptotic mechanism and degenerate around the fourth day. Common donor sites for fat harvesting include the abdomen, flanks, lumbar area, dorsum, and thighs. Because donor sites are similar to one another in terms of fat viability and long-term stability, donor site selection depends on accessibility, the patient’s position on the operating table, the patient’s fat deposits, and the patient’s desires. Harvesting approaches include syringe aspiration and lipoaspiration. There is no difference in fat viability with either technique as reported in a recent literature review by Sinno et al. In our practice, adipose tissue is harvested through small, easily concealed incisions. We use infiltration with a tumescent technique, with 1:1,000,000 epinephrine. If general anesthesia is used, we avoid adding lidocaine or other local anesthetic into the infiltration solution, mainly because of its marginal benefits in comparison to the risk of adverse effects. When harvesting fat for microinjection, we prefer low-pressure syringe aspiration as described by Coleman. Conversely, when macroinjection is needed, we use the traditional liposuction technique with a recollection recipient. It is of the utmost importance that a favorable body contour be achieved at the donor site, with careful attention paid to avoid wrinkling and contour deformities. Following harvest, the fat needs processing in order to separate the viable adipose cells from the oil, cell debris, blood, and infiltration solution, with three main techniques having been described for this purpose: centrifugation, washing, and sedimentation and straining. There is no evidence of superiority of any one technique, but the graft must be handled with the least possible trauma and ischemic time. Centrifugation of the lipoaspirate is usually done in a centrifuge at 1,500–3,000 rpm for 2–3 minutes. This yields a three-layered solution composed of oil and cell debris on top, viable adipose cells in the middle, and blood and infiltration solution on the bottom. Washing consists of mixing the harvested fat with washing solutions, such as normal saline, lactated Ringer solution, glucose 5% solution, or even sterile water. The mixture is then left to rest in order to separate the oil, debris, water, blood, and infiltration solution from the viable adipose cells. This method, nevertheless, may traumatize the adipose cells and reduce their viability. Sedimentation is believed to be the least traumatic technique and is the authors’ preferred method. The harvested fat is left still until the components separate into a three-layered product with the oil and debris on top, the viable cells in the middle, and the blood and infiltration solution at the bottom. Lastly, straining involves rolling the fat gently through cotton gauze until the liquid component of the harvested tissue is filtered and separated from the stroma. Because initial survival of the fat graft is by diffusion, injection should maximize the surface area of contact with the surrounding tissue in order to optimize graft survival. Furthermore, small amounts of graft should be injected in a multiplanar radially oriented fashion because injection of large volumes of fat graft can result in central ischemia and subsequent necrosis, leading to partial graft loss, loss of volume, and possible cyst formation. For microinjection the authors prefer a Coleman cannula with 1 mL syringes, whereas for macroinjection, a 3 mm blunt cannula is usually used with 50 mL syringes. To reduce the risk of vessel injection, the graft should be injected with low pressure and during withdrawal of the cannula. There is evidence that survival of macroinjected fat can be enhanced with the use of an external expansion device for several weeks preoperatively. Note We prefer harvesting the nearest available fat deposit with a blunt cannula technique followed by sedimentation and immediate injection of small amounts of fat in multiple passes.
14.1 Introduction
14.2 Basic Science
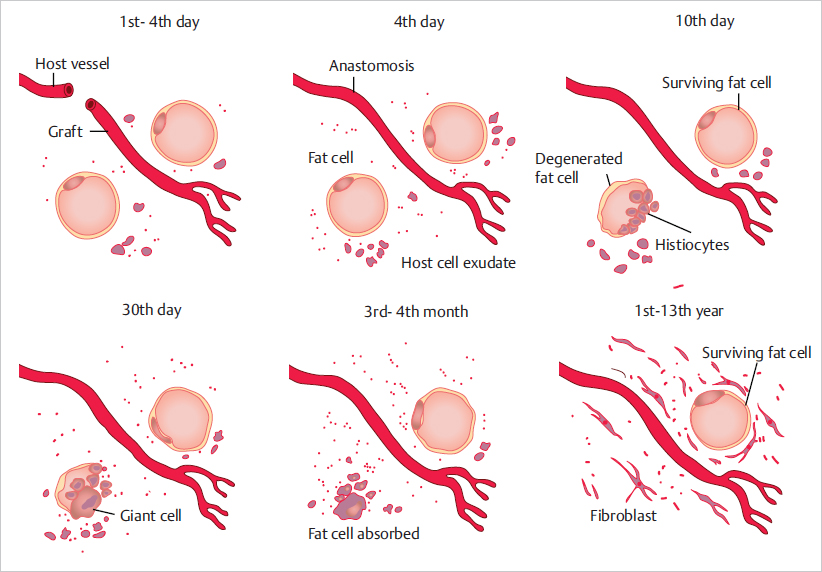
![]() Fig. 14.1). In 1950, after a series of fat transplantations, Peer observed that the average loss of autografts is 45% of their original volume at 1-year follow-up. He also observed that the viable adipocytes at the time of transplantation determine the volume of the final fat graft.
Fig. 14.1). In 1950, after a series of fat transplantations, Peer observed that the average loss of autografts is 45% of their original volume at 1-year follow-up. He also observed that the viable adipocytes at the time of transplantation determine the volume of the final fat graft.
14.3 Surgical Technique
14.3.1 Fat Harvesting
14.3.2 Fat Processing
14.3.3 Fat Injection
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


