Fan Flaps
W. R. MULLIN
D. R. MILLARD JR.
These flaps were given the name “fan flaps” because of their resemblance to the rotational opening of an oriental folding fan.
INDICATIONS
The fan flap procedure is used today to correct larger full-thickness defects of both upper and lower lips. Attributes of the fan flap are as follows. Two basic principles (1) are observed using this flap: (a) losses should be replaced with similar types of tissue, and (b) tissue from an area of relative excess to supply an area of need should be used. Few conventional axial flaps allow such freedom of movement of such large amounts of tissue based on such a small pedicle. Also, most donor-area scars may be located close to the natural junction lines of facial units.
The fan flap has found its best use for reconstruction of large central full-thickness defects of both upper and lower lips. In such defects, the use of bilateral symmetrical flaps rotated medially usually affords the most satisfactory final result.
FLAP DESIGN AND DIMENSIONS
Owing to the marked elasticity of the lips, evaluation of defects must be determined in the absence of induration and edema. The exact amount of lip loss usually can be judged quite accurately, especially in primary surgical losses resulting from resections for carcinoma if there has not been a large inflammatory response to the tumor. Defects secondary to burns or infection should be allowed to heal to stability and softness before planning reconstruction.
It is most important to recognize that the amount of tissue required to reconstruct an attractive lip is always less than the size of the original defect. It must be stressed that the edges of the defects actually must be grasped and approximated to the desired location so that the true defect to be reconstructed can be visualized and measured. One may see exact percentages quoted, stating X percent of a lip defect can be closed primarily; however, this is a general rule and only a rough guide. More important are the actual examination and the final relationship
of the lip to the opposite lip once the defect is closed. For example, one may be able to close an upper lip tightly without the use of a flap; however, the lower lip may have an unsightly protruding appearance relative to the upper lip.
of the lip to the opposite lip once the defect is closed. For example, one may be able to close an upper lip tightly without the use of a flap; however, the lower lip may have an unsightly protruding appearance relative to the upper lip.
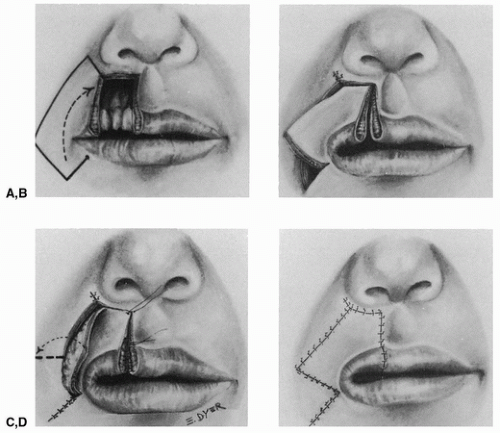 FIGURE 175.1 A-D: Unilateral fan flap for the upper lip. |
The units of the lips always must be honored. In large central upper lip defects, a midline shield-shaped Abbé flap from the lower lip to reconstruct a philtrum may be in order (2, 3); however, this should be done as a secondary procedure so as not to compromise any blood supply traversing the circumoral labial vessel.
Large full-thickness defects of the lateral lip may be repaired using the unilateral fan flap. One also should consider the use of an off-center Abbé flap (4) or an Estlander flap (5), which may be a less elaborate solution to the problem.
Once the true defect that requires reconstruction has been determined, considering laxity and opposite lip relationship, one may proceed to the outline of the flap. A dot is placed at the desired location of the new mouth corner. The length of the defect to be filled is transferred along the adjacent vermilion, and from the point marked, a line is dropped perpendicular from the white roll. The length of this line establishes the bulk and size of the flap, and usually it is at least 1 to 1.5 cm long.
An angle of approximately 60 degrees is turned toward the nasolabial fold. Once the nasolabial fold area is transected, the line follows this area to a point that will provide adequate height and bulk to the flap. In general, approximately no more than one half the upper lip (Fig. 175.1) and two thirds of the lower lip (Fig. 175.3) should be attempted using a unilateral fan flap (1).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


