Key points
- •
Gel hardness is a factor in deciding which hyaluronic acid (HA) filler to use depending on the physician and patient.
- •
Restylane indications.
- •
Juvéderm indications.
- •
Adjunctive use of Botox with the HAs.
- •
Key areas can be safely corrected for contouring and shaping the aging face.
Introduction
As we have become more aware of the contribution of qualitative changes of skin and other soft tissue volume depletion effects to facial aging, a comprehensive approach to facial rejuvenation nearly mandates filling agents to achieve the best results. The paradigm shift has swung away from mono-therapy with surgical tightening or repositioning to a more comprehensive approach with the incorporation of a variety of soft tissue fillers. The field of soft tissue filling has also evolved from line (dermal) filling to deeper volumetric reflation. The options for injectable soft tissue augmentation agents continues to grow. In this chapter are descriptions of two particular families of hyaluronic acid filling agents, a rationale for their use and particular product selection as well as techniques to attain optimal results.
Background
In the past 20 years, the appreciation of commercially prepared filling agents as a viable option or complement for facial rejuvenation has surged world-wide. Beginning with bovine collagen, which reigned for the last two decades of the 20th century, the introduction of next-generation products including injectable hyaluronic acid heralded the promise of improved results and safety, a wider spectrum of applications, and longer-lasting effects.
The era of injectable agents for facial aesthetic enhancement, however, started several years after the waning use of bovine collagen in the US, and can be best associated with the introduction of the cosmetic use of botulinum toxin type A (BTX-A) ( ). With BTX-A, both physicians and patients could experience dramatic improvement in their facial appearance by injection that posed negligible down-time and consistent, predictable results ( , ). Initial applications of BTX-A were primarily administered to the upper facial regions and, despite the ability to improve some areas of lower facial aging by chemodenervation with neurotoxin, it became obvious that there was both a void and a strong desire to have reliable and longer-lasting filling agents that could significantly improve the appearance of the lower facial regions. Collagen products proved to be more effective for improvement of the appearance of facial lines yet less effective in replacing lower facial volume loss that would often require an abundance of material that in some could dissipate in a matter of weeks. During that time, there was only sparse discussion of using hyaluronic acid (HA) as a soft tissue filler, yet those in other fields of medicine that already began to incorporate these agents (ophthalmologists and orthopedic surgeons) and preliminary experiences revealed that residence time of non-manipulated HA was, at best, simply a few days.
Research was directed towards reduction of in-vivo degradation of HA using maneuvers borrowed from experiences with bovine collagen (namely cross-linking) that were effective in reducing enzymatic degradation of these agents once injected into the skin ( ). Products such as Restylane® were first introduced for commercial use in Europe (where there are less vigorous regulatory pathways) and physicians who gained experience with these agents were reporting superior results. With the FDA approval of Restylane in 2003, the cosmetic market for injectable agents utilized by practitioners grew at an unanticipated accelerated rate as physicians now had the ability to manage a wider range of facial aging that extended more predictably to the lower face with greater persistence ( , ).
Although reports from European experiences suggested results beyond two years, the reality was that novice injectors could increase the persistence of existing filling agents (bovine collagen) by at least a factor of two. Despite other experiences world-wide, US practitioners extended applications from the commonly treated areas such as the nasolabial folds, lips, and oral commissures to a growing list of facial and extra-facial regions including the jowls, jawline, periorbita, chin, cheeks, forehead, temples, nose, ears, hands and feet ( , ). New patients could be treated on the same day of the initial visit due to the lack of need for skin testing and the eagerness of many to participate in the latest form of youth by injection.
It is my opinion that many of the newer injectable agents including, but not limited to, hyaluronic acids may be appropriate for many areas of the face. As we are gaining more experience with these agents, it is becoming more apparent which agents work best and where. In addition, problems related to early experiences are largely due to inexperience and even mild adverse events in most situations can be traced back to poor injection technique rather than being related to the product itself. With our initial introduction to Restylane, although many injectors with a higher level of understanding of the nature of these new agents could achieve highly pleasing result for their patients, the broader experiences were sometimes met with some difficulties as clinicians could not easily adjust from the injection techniques of collagen with which they were familiar. Many situations were also approached with greater caution leading to conservative volumes (also influenced by cost) that resulted in disappointment and undercorrection ( ).
Some injection techniques, including the plane and volume recommendations were based simply on a few anecdotal suggestions that initially became common practices without the benefit of experience. For instance, many injected these agents in a too superficial plane and delivered results that were also sub-optimal due to visibility of the injected product, which also led to a small degree of dissatisfaction. Again, these issues were far less related to product integrity and more often related to issues that were more proximal to the syringe. In short order, however, many were achieving quite satisfactory results in most facial regions adopting evolved techniques and expanding applications. The availability of a host of hyaluronidase products ( ) that could readily dissolve product that may have been sub-optimally placed also gave many injectors the comfort to approach facial filling with more fortitude.
The Juvéderm® family of products, also first introduced in Europe, were relative late-comers to the HA phenomenon in the US. The European comparative experience (Restylane® vs Juvéderm®) was mixed as some preferred one over the other with a large lack of consistency that was less understood. When the Juvéderm® products became approved for use in the USA in 2006, many practitioners were already quite comfortable with their use of the Restylane® line (NASHA) products and were slow to convert existing patients to trying these newer products. Others who lacked experience with these new agents were not convinced that these could perform with much difference from Restylane®. Slowly, clinicians gained more experience with Juvéderm® products and made their own determination of which agent they preferred, which might have been influenced by a variety of issues too complex to discuss. Although the basic scientists would argue the differences and advantages of one against the other, it became clear that these two HA products behaved quite differently.
Finally, with further experience, it also became obvious to many clinicians that one product might perform optimally in one facial region and the other product in another region. This presumption has come to fruition and most experienced injectors have learned which regions and patient individual presentations respond best to one agent versus another as well as which regions are comparable with either agent. Although there are dozens of HA products available worldwide, this chapter discusses primarily the author’s experiences of the two families of HA products that are presently available in the US and are matched in global popularity. The selection process, philosophies, observations, and experiences of the uses of these agents by the author is described herein.
Restylane®
Again, as the first available HA agent in the US, we all gained a wealth of experiences and expanded its applicability as the comfort level with this product grew. The most successful regions treated were as expected (nasolabial folds, lips and oral commissures) and yet expanded and previously unexplored areas of treatment were also met with as least as much excitement. This was especially true for regions that had been previously reserved for the use of autologous fat such as the pre-jowl sulci, cheeks, brow, temples and chin. Other areas such as the lower eyelid, tear troughs and superficial facial lines were consistently met with mixed reviews that began to better elucidate which areas should be either avoided or approached with caution, as well as techniques that optimize outcomes. Nonetheless, we now had a new filling agent in our armamentarium that more closely resembled our criteria that approached ideal.
What is most interesting and practical is not adopting the theoretic explanations of the differences of HA products, rather amending practices based on a wide array of experiences and retro-fitting this with theory that improves results and may have previously been justified by pseudo-science. For instance, we understand that a major difference between Restylane®, Perlane® and other HA products related to rheological characteristics such as G’ or gel hardness. This can be a positive attribute especially as it relates to soft tissue projection and radial expansion when these agents are used to correct volume deficiencies. This is true for, yet not limited to, deep nasolabial folds, flattened cheeks, chin deformities, and the pre-jowl sulcus. When Restylane® was the only approved HA in the US, it was soon applied to most areas of the face with varied techniques, fortunately delivering satisfactory results in many. The gel hardness, however, made it more difficult to treat fine lines. In some however, this could be achieved by incorporating finer needle gauges or injecting into the superficial dermis without causing visibility of the product that often manifested as lumps and bumps that at times could be resolved with vigorous massage or hyaluronidase but, without treatment, could last for years. These adverse experiences suggested to most injectors that this product was best directed to the deeper dermis. As injection techniques evolved, and superior results were achieved, the popularity of this agent grew exponentially.
Juvéderm®
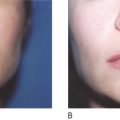
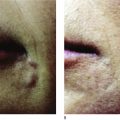
Increased gel hardness has its advantages but also its disadvantages. Many patients experience dramatic improvement with the use of Restylane®. However, at times some felt the product to be too lumpy either palpably or visibly in some facial areas and patient profiles. Experiences with Juvéderm® has shown it to be a softer gel particle filler and in lieu of reduced gel hardness could be more readily applied to the superficial dermis without creating palpable or visible nodules. The problems, however, with reduced gel hardness is a reduced projection that might be desirable in some facial aging regions. This softness was highly advantageous for applications to the mild or moderately deep nasolabial folds in the patient with thinner skin, dermal contour defects that had a line component to it, and some lips (see Case Studies 4 , 5 ) and was less suited in areas where high projection was preferable like the pre-jowl sulcus. Areas like the cheeks could be re-inflated, however, and simply required a bit larger volume (see Case Study 6 ).
The trade-off regarding volume is that softer gels can be placed more superficially in the dermis with avoidance of visible product lumps and possibly achieve more correction in this plane with less volume yet in contrast, typically have less projection so more volume is required to elevate the deeper plane soft tissue depression. Harder gels, on the other hand, must be placed deeper to avoid visible product yet still have the advantage of increased projection. They also tend to remain close to the injection site with a slightly increased cohesivity that may present challenges for fine lines yet has advantages in some areas for example, the tear-trough. There also are some fine discriminatory differences between these two products as they relate to the hygroscopic effects and subsequently the hydrophilic characteristics that translate to differences in the level of localized water retention. Understanding the nuances and characteristics in vivo of a particular HA product allows for selection of the most suitable product that considers the nature of the treated area, potential sequelae, and cost.
Related posts:
 Injectable silicone: current role
Injectable silicone: current role
 Poly -l-lactic acid (Sculptra®)
Poly -l-lactic acid (Sculptra®)
 The potential role of adipose derived stem cells as semi-permanent/permanent fillers in aesthetic surgery
The potential role of adipose derived stem cells as semi-permanent/permanent fillers in aesthetic surgery
 Avoidance and treatment of complications after dermal filler injections
Avoidance and treatment of complications after dermal filler injections
 Possible causes and treatment options of dermal filler granulomas
Possible causes and treatment options of dermal filler granulomas
 Shaping the future: new outcomes in Europe
Shaping the future: new outcomes in Europe
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


