Key points
• The male skull is longer and broader compared with the female skull, whereas the female skull has a more pointed chin and tapered jaw.
• Frontal bossing of the male skull generally extends from the region of the nasion medially to the supraorbital region extending laterally to the zygomaticofrontal suture of the lateral orbital wall on each side.
• From an anatomical perspective, the forehead and thyroid cartilage are the two most “masculine” characteristics of the male face.
• Approximately 20% of the female population demonstrates a mild to moderate degree of midforehead bossing (MFB) while approximately 50% of the male population demonstrates midforehead bossing in addition to supraorbital bossing (SOB).
• With many transgender patients presenting in their 50s and 60s, rejuvenation procedures contribute as much to the feminization process as do FFS procedures.
• Narrowing of the chin in the transverse plane by T-osteotomy genioplasty can dramatically change the angularity of the lower face creating a desirable V-line configuration.
• The T-osteotomy genioplasty advancement (TOGA) procedure permits narrowing of the chin in the transverse plane as well as advancement of a retruded chin.
• Feminizing a strong male chin often requires reducing the height of the chin and narrowing the width of the chin with a sliding genioplasty.
• In most transgender women, a successful transformation and the ability to “pass” are dependent on reduction of the thyroid cartilage–chondrolaryngoplasty.
• Care must be taken during thyroid cartilage resection to avoid injury to the adjacent vocal cords which could result in permanent voice changes and hoarseness.
Introduction
Almost 40 years ago, Dr. Douglas Ousterhout pioneered the field of facial feminization surgery (FFS) when, in 1982, Dr. Darrell Pratt, a plastic surgeon who performed gender reassignment surgery (GRS), conveyed the request of a male-to-female transgender patient who wished to have more feminine facial features as people still reacted to her as though she were a man despite her GRS. That request opened the door to a new world in which techniques of transforming the larger, more angular male features to smaller, softer, more feminine female features evolved and progressed with the goal of matching one’s external appearance with the internal perception of oneself.
Bony differences
Numerous anthropologic and anthropometric studies have defined the characteristics that distinguish male skulls from female skulls. In general, the male skull is longer and broader compared with the female skull, whereas the female skull has a more pointed chin and tapered jaw ( Fig. 40.1 ). Frontal bossing of the male skull generally extends from the region of the nasion medially to the supraorbital region extending laterally to the zygomaticofrontal suture of the lateral orbital wall on each side. Perhaps the most prominent component of frontal bossing overlies the frontal sinus and extends laterally as a ridge of varying thickness ( Fig. 40.2 ). The female forehead demonstrates a much more consistently convex contour, with minimal supraorbital ridging or bossing. However, approximately 20% of the female population demonstrates a mild to moderate degree of midforehead prominence or bossing, and approximately 50% of the male population demonstrates midforehead bossing of varying degrees in addition to supraorbital ridging. In general, broader more prominent nasal bones will translate to larger noses in the male, although this is clearly not always the case.


Soft tissue differences
Typical differences in soft tissue characteristics between the male and female faces include skin thickness, especially with respect to the lower third of the nose, presence of the male beard, position of the eyebrows and hairline, temporal hair density, and upper lip length. The male eyebrow rests at or slightly below the supraorbital rim and bony ridge, whereas the female eyebrow rests above the supraorbital rim and bony ridge. As a result, women have a shorter distance between the hairline and eyebrows. The average distance from the hairline to the eyebrow at the midpupillary line is approximately 3 inches in the male and 2 inches in the female. This distance increases as the hairline recedes in the male, especially with loss of hair in the temporal and midforehead regions. The upper lip of the male tends to be longer and flatter than that of the female with less tooth show demonstrated.
Goals of facial feminization surgery
Although the desire to “pass” may be the most commonly stated goal of FFS, lifelong internal struggles with the paradox of improper gender embodiment ultimately cause trans women to strive to feel comfortable in their own skin. Certainly, the importance of external gender perception by others matching one’s own perception of self cannot be understated. Many patients present in their 20s, but some present even in their 60s and beyond, often married and with grown children, indicating they finally have the means, resolution, and support to move forward with what they had contemplated and yearned to do their entire lives. Assimilation and integration into the workplace, family, and social situations are also important goals of FFS. Keith Haring’s vision of a genderless society where equality reigns independent of gender ( Fig. 40.3 ) represents a type of utopia sought by many. Gender equality or “gender blurring” has been symbolically depicted by the transgender community to represent that journey. The transgender symbol links the internationally accepted symbols for male and female together with a new entity that is a combination of the two ( Fig. 40.4 A) and is increasingly seen in public venues and businesses (see Fig. 40.4 B).
Managing patient expectations
As with every plastic surgery patient, the patients’ expectations and the surgeons’ vision must be aligned to achieve a successful outcome and a satisfied patient. The transgender patient is no different. A whole world of additional psychology is involved in working with the transgender community, but at the end of the day, the patient and the surgeon must be on the same page before any surgery is undertaken. , Realistic expectations must be met with realistic reassurances. It is often hard to say to the transgender patient, or any patient, “I’m a physician, not a magician.” If the surgeon feels that only a magician would be able to deliver the desired result, then it must be conveyed to the patient that the surgeon will not be able to meet their expectations and that rather than displeasing the patient, the surgeon would prefer that the patient meet with another Board-certified plastic surgeon who might be better able to achieve the result sought. There is no shame in being honest and direct. To the contrary, the patient will be appreciative and potentially adjust his or her expectations as a result. Choosing to find another surgeon will likely do a favor to oneself and the surgeon.
Principles of facial feminization surgery
First do no harm
With FFS, as with all surgeries, including aesthetic surgery, the first principle is derived from the Hippocratic Oath: First do no harm. This especially applies to FFS where some patients may wish to undergo “full facial feminization” in one stage, and some surgeons may be tempted to comply. Conversely, some surgeons may seek the opportunity to combine an excessive number of procedures. The corollary to this principle, of course, is “Safety first.”
The primary goal of FFS is to produce a happy, live transitioned patient. Therefore procedures should be combined only when it is safe and feasible to do so. With some patients, it is certainly feasible to address all concerns in one sitting and achieve “full facial feminization.” With others, however, it simply is not, and overambitious 14-hour procedures should generally be avoided if the first principle of FFS is adhered to and the primary goal of FFS and the surgeons’ goal are the same.
Proportion and symmetry
Ousterhout defined proportion as “the relationship between individual features and the whole face.” 6 The proportion of the face can change in myriad ways, such as when the scalp and hairline are advanced and the forehead height is reduced or when the chin is shortened and the entire face length is decreased. Therefore it is paramount to consider the aesthetic and structural consequences of every procedure before it is performed. This consideration is especially important when multiple procedures are performed simultaneously.
Ousterhout defined symmetry as “sameness between corresponding sides of the face.” Although perfect symmetry is typically not found in nature, in general, individuals with greater degrees of facial symmetry tend to be more attractive, whereas those demonstrating obvious facial asymmetry are usually not considered attractive, but this is not always the case. The goal is always to achieve or restore facial balance, and this is often accomplished by correcting asymmetry or improving symmetry.
Rejuvenation = feminization
Many transgender patients in their 50s and 60s present without a history of prior FFS. In this group of patients rejuvenation procedures, such as facelift, neck lift, and blepharoplasty, contribute as much to the feminization process as do frontal bossing correction, tracheal reduction, and T-osteotomy genioplasty. In fact, performing the traditional FFS procedures to address the male face without addressing the aging face would be counterproductive because squaring of the face with the development of prominent jowls, midface descent with accentuation of the nasolabial folds and marionette lines, and development of eyelid festoons are masculinizing characteristics in both sexes. Every artist knows that before applying the brushstrokes that will create the masterpiece, the canvas must first be “prepped.” The same applies to the face. Aggressive rejuvenation of the male face will produce a feminized appearance; this was the goal of a transgender decathlon winner, but it certainly was not that of a non–transgender country singer, who gambled and lost.
FFS procedures
The FFS armamentarium comprises a multitude of bony ( Table 40.1 ) and soft tissue ( Table 40.2 ) procedures, performed individually or in combination. Most of these procedures are routinely performed in both sexes in a busy aesthetic surgery practice, but some others, such as supraorbital bossing correction and tracheal reduction, are more specifically intended to achieve feminization in the transgender patient. More so than the procedures themselves, it is the surgeon’s transformative vision, the patient’s realistic expectations, and the individualized goals of these procedures that are paramount to successful FFS. Thus variations and combinations of certain procedures are designed to achieve a specific result, for example, a V-line contour with T-osteotomy genioplasty advancement (TOGA), mandibular contouring, and masseter reduction.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Scalp advancement
Receding male hairlines produce the typical gull-wing appearance with vertical lengthening of the forehead and temporal hair loss. Scalp advancement is performed by utilizing a coronal incision at the anterior edge of the hairline. With dissection posterior to the vertex approaching the occiput and galeal scoring, 15 to 30 mm of advancement can be achieved. Depending on the degree of hair loss and the distance from the eyebrows to the hairline, it may be necessary to perform secondary scalp advancement 6 to 12 months later, especially when temporal hair loss is severe. In such cases, a hair transplantation procedure might be considered to produce the optimal result. An important caveat with regard to scalp advancement is that a differential advancement will yield the most natural-appearing female hairline, which typically extends more evenly across the forehead without temporal peaks. Therefore the hairline needs to be advanced in the midline by only 15 mm, but it may be necessary to advance the temporal peaks by 25 mm or more to achieve a consistent result across the forehead. Temporary hair loss at the incision is not uncommon due to tension applied across the incision, and it usually resolves within 6 to 12 weeks. Scalp advancement is commonly performed in conjunction with frontal bossing correction in this transgender patient population and will be demonstrated in the following section.
Frontal bossing correction
From an anatomic perspective, the forehead and thyroid cartilage (discussed later) are the two most “masculine” characteristics of the male face. Other features may affect both sexes to a greater or lesser extent, but these two are specific to the male. With the forehead spanning 30% to 40% of the face, which comprises a significant amount of facial “real estate,” it is essential that prominent frontal bossing be addressed to achieve facial balance and a feminized appearance.
Ousterhout characterized the male forehead as having significant forward projection, brow ridging or supraorbital bossing, and a small flat recess approximately 2 cm above the nasion, and the female forehead as being convex and smooth and lacking the flat recess. The male with larger than normal frontal sinuses, due to hyperpneumatization or pneumosinus dilatans, will demonstrate an even greater degree of frontal bossing. Such frontal sinuses often demonstrate a thinner anterior sinus wall, which should be taken into consideration during planning of frontal bossing correction. It should be noted that 5% of people lack frontal sinuses and that 8% have only one.
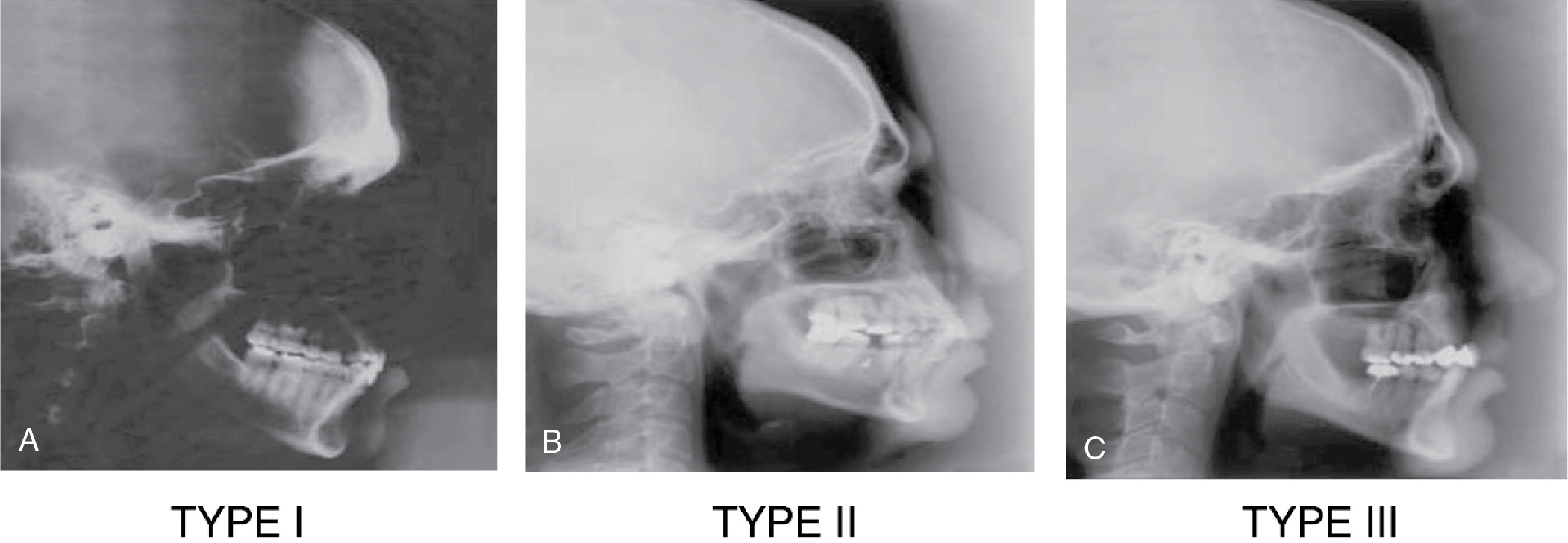
Ousterhout classification
Based on the extent of frontal sinus development, prominence of frontal bossing, and thickness of the anterior frontal sinus wall, Ousterhout described four approaches for surgical correction of bossing. Types I to III relate directly to frontal bossing and the underlying frontal sinus development and can be demonstrated with cephalograms ( Fig. 40.5 A-C), whereas Type IV relates more to forehead deformities requiring custom implant reconstructions, for which Ousterhout used methylmethacrylate, than to frontal bossing.