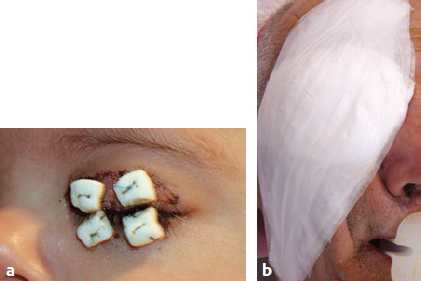
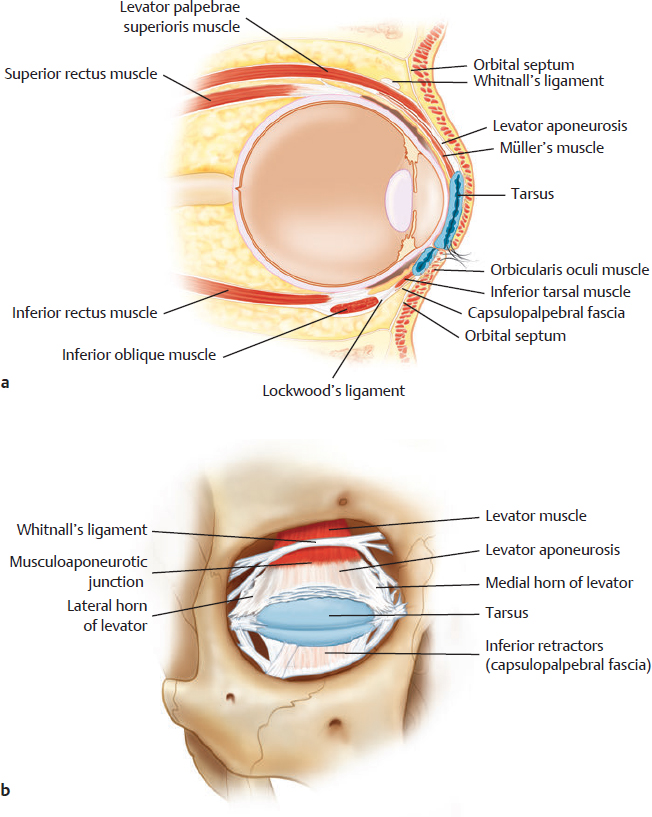
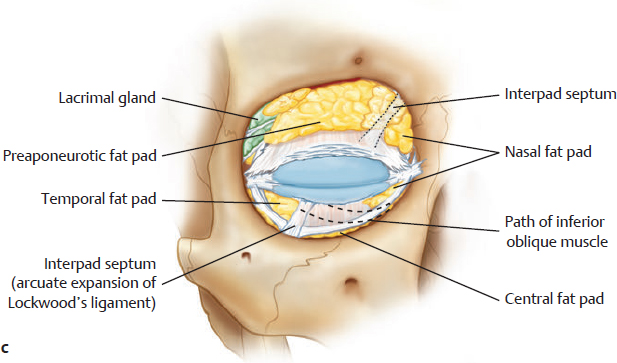
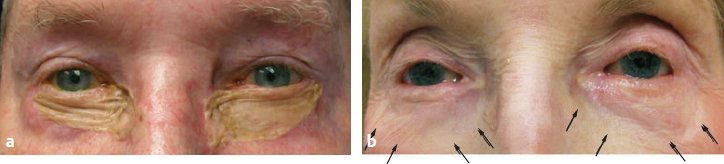
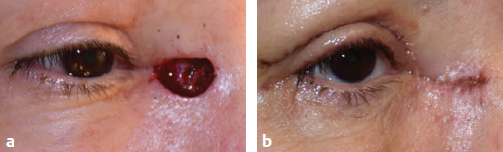
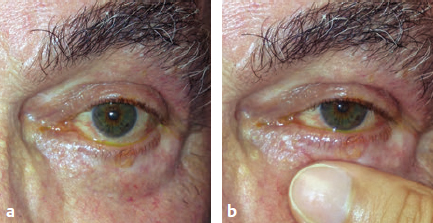
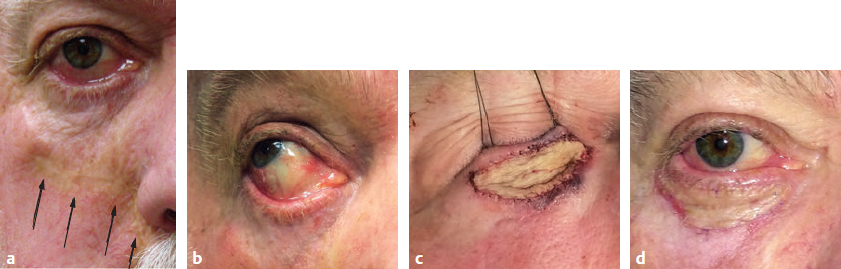
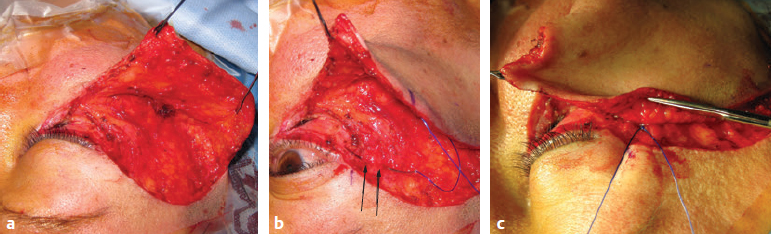
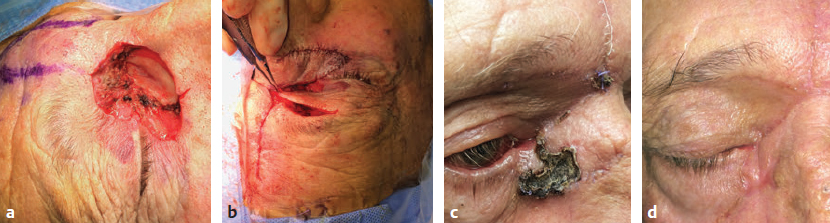
CHAPTER The eyelids are challenging structures to reconstruct because of their unique anatomy, their juxtaposition to a sensitive and vital organ, and their location as the aesthetic focal point of the face. The stakes are high, and patient expectations are even higher. An asymmetry as small as 1 to 2 mm is often perceived as an unacceptable complication by the patient. It is imperative to remember that the most important goal of eyelid reconstruction is to protect the globe. Poorly repaired eyelids leave the globe susceptible to corneal exposure, corneal abrasions and scarring, or even a ruptured globe. Postoperative complications in eyelid reconstruction can be avoided through proper surgical decision-making and reconstructive techniques. This chapter reviews key eyelid anatomy, identifies surgical strategies to reconstruct specific components of the eyelids, and offers surgical pearls to prevent and correct common complications. The eyelids play a critical role in maintaining ocular health by serving as a barrier between the globe and the outside world. They also sustain tear homeostasis by distributing tears evenly across the ocular surface and draining tears through the puncta and nasolacrimal system. This is accomplished when the eyelids are oriented and functioning properly. Proper apposition of the eyelids to the globe prevents desiccation of the ocular surface and keeps the puncta in contact with the upper and lower lid tear meniscus. Disruption of this anatomic relationship causes significant ocular surface irritation and ineffective tear drainage. Entropion (inturned eyelid) irritates the ocular surface by chafing with the eyelashes and keratinized skin. Ectropion (out-turned eyelid) distracts the lid from the globe and leaves the ocular surface exposed without proper lubrication (Fig. 55.1). Horizontal stabilization or tension, through firmly anchored medial and lateral canthal tendons to the orbital rim, gives the characteristic V appearance to the medial and lateral canthi. The tendons stabilize the eyelids during contraction of the orbicularis oculi muscle during the blink. Without sufficient horizontal tension on the eyelid, the horizontal palpebral fissure (the distance between the medial and lateral canthus) narrows and pseudo–eyelid retraction develops. This can affect blink dynamics and cause incomplete closure of the lids. The lower eyelid should rest at the inferior limbus, the inferior border of the cornea, whereas the upper eyelid should rest 1 to 2 mm below the superior limbus. The temporal and zygomatic branches of the facial nerve maintain orbicularis oculi tone and facilitate a complete blink. The blink not only distributes tears along the ocular surface but also contracts the lacrimal sac. This latter function is a vital component in the physiology of tear drainage. Weakened or absent orbicularis tone can lead to lagophthalmos, brow ptosis, and neurogenic lower lid ectropion. Fig. 55.1 (a) Proper lid position. (b) Entropion. (c) Ectropion. Fig. 55.2 Eyelid anatomy. (a) Sagittal view (including the layers of the upper and lower eyelids). (b) Tendinous attachments. (Reproduced from Codner MA, McCord CD. Eyelid and Periorbital Surgery. 2nd ed. New York: Thieme Medical; 2016.) Eyelid anatomy. (c) Fat pads. (Reproduced from Codner MA, McCord CD. Eyelid and Periorbital Surgery. 2nd ed. New York: Thieme Medical; 2016.) The levator is the main elevator of the eyelid and inserts on the anterior face of the tarsal plate. The levator also sends anterior projections to the skin and orbicularis muscle that create the eyelid crease. The upper lid crease varies in its presence and position according to ethnicity. Disinsertion or weakening of the levator causes varying degrees of ptosis that can obstruct part or all of the visual field, whereas fibrosis or scarring of the levator can result in upper eyelid retraction. Understanding several key aspects of eyelid anatomy is critical for a successful reconstruction. Starting from the eyelid margin, the first 10 to 12 mm of the upper lid and the first 4 mm of the lower lid have similar anatomic layers: the skin, orbicularis oculi muscle, tarsal plate, and conjunctiva1 (Fig. 55.2). Oculoplastic surgeons group these layers into reconstructive units, the anterior lamella (skin and orbicularis oculi muscle) and the posterior lamella (tarsal plate and conjunctiva). Conjunctiva lines the posterior aspect of the eyelids and extends into the upper and lower lid fornices, invaginations where the eyelids fuse with the ocular surface. The conjunctiva is a nonkeratinized mucus membrane that secretes mucus into the overlying tear film. This allows for a smooth glide across the sensitive ocular surface with each blink. The puncta are located at the medial aspect of the upper and lower lid margin and are responsible for draining the tears through the nasolacrimal system. Above the superior tarsal border of the upper eyelid, the anterior lamella remains the same, but additional structures come into play. The orbital septum, also known as the middle lamella, is a dense layer of connective tissue that separates the eyelid from the vital orbital structures posteriorly. This includes preaponeurotic fat, the levator aponeurosis, Müller’s muscle, and the conjunctiva. The same arrangement is seen in the lower lid, except the lower eyelid retractors are referred to as the capsulopalpebral fascia (see Fig. 55.2). Before beginning to reconstruct the eyelids, it is critical to ensure that any eyelid neoplasm has been adequately resected and that biopsied tissues have been reviewed by a trusted pathologist. If a patient is referred from an outside facility, the pathology slides should be obtained and reviewed to confirm the diagnosis. In cases where this is not possible, repeat biopsy may be indicated. A metastatic workup should be performed when indicated (e.g., melanoma, large sebaceous carcinoma) before planning total tumor resection. Adequate surgical planning prevents most complications. A thorough review of the patient’s past history is undertaken to identify risk factors for complications. Microvascular disease resulting from hypertension, hyperlipidemia, diabetes mellitus, radiation exposure, or tobacco use can affect postoperative tissue perfusion, although the incidence of postoperative vascular complications is low in the periocular region.2–4 A careful review of previous periocular reconstructive surgeries helps identify available tissues for further reconstruction. For example, if a patient has previously undergone a Hughes tarsoconjunctival flap, which uses the posterior lamella of the upper lid to reconstruct the posterior lamella of the lower lid, a second Hughes flap cannot be performed for a new or recurrent lower eyelid neoplasm. Many patients may not fully understand their previous reconstructive procedures, but a review of prior operative reports and careful examination of the eyelids and potential donor sites will yield evidence of prior tissue manipulation. In addition, the surgeon can anticipate potential complications or successes by taking note of previous graft contracture, scar formation, and flap viability. Summary Box Complications in Eyelid Reconstruction Anterior lamella • Scar formation • Cicatricial ectropion • Graft/flap necrosis • Facial nerve paralysis • Medial canthal webbing Posterior lamella • Lid margin notch • Eyelid retraction • Cicatricial entropion • Lateral canthal dystopia Tear drainage system • Canalicular stenosis Other • Retrobulbar hemorrhage Postoperative bleeding complications can cause devastating outcomes, such as skin graft necrosis or a retrobulbar hemorrhage causing compressive optic neuropathy. Appropriate suspension of antiplatelet agents and anticoagulants is advisable, particularly if there are no grave systemic contraindications. This, in combination with using local anesthetic mixed with epinephrine and meticulous intraoperative hemostasis, will aid tremendously in reducing bleeding complications. Reconstructive planning commences once the eyelid tumor has been excised with clear margins. Most eyelid neoplasms are fairly superficial and straightforward to remove, but aggressive lesions can extend posterior to the orbital septum and involve the orbital fat. In such cases, a report of clean margins should be viewed warily, because orbital fat involvement is often associated with residual microscopic disease (Fig. 55.3). Definitive reconstruction in this setting or any setting where tumor cannot be cleared should be deferred. Temporizing measures are taken to protect the globe and maintain patient comfort as further treatment plans are considered. These patients require close follow-up, because more extensive treatment such as radiation or exenteration of the total orbital contents is often indicated. Valuable reconstructive options are thus preserved for future use. Fig. 55.3 Eyelid defects. (a) Superficial wound. (b) Deep wound with orbital involvement. In creating a reconstructive plan, the surgeon must take a systematic approach toward assessing areas of tissue loss, including the anterior lamella, posterior lamella, medial canthus, lateral canthus, and nasolacrimal drainage apparatus. In addition, if the entire upper or lower lid tarsal plate is absent, the upper eyelid retractors (particularly the levator palpebrae superioris) and lower eyelid retractors will need to be reattached to the newly reconstructed posterior lamella. Many options exist for repair of anterior lamellar defects. Preoperative considerations in anterior lamellar reconstruction include color and texture match, graft and flap thickness, and vertical lamellar support. The eyelid skin is the thinnest and arguably the most visible skin of the entire body, so the ideal donor site should optimize color and texture match and be non–hair-bearing when possible. Skin grafts from the eyelids are the ideal option for eyelid reconstruction, and excess upper eyelid skin can often be harvested via a blepharoplasty incision. In cases where there is insufficient upper lid dermatochalasis, extensive photodamage, history of eyelid cancers, or scarring that makes eyelid skin grafts otherwise unsuitable, retroauricular, supraclavicular, pretragal, or medial upper arm skin can serve as alternative options. Hair-bearing skin and thicker skin from other parts of the body are cosmetically inferior (Fig. 55.4). Fig. 55.4 Bilateral lower lid skin grafts. (a) Graft using split-thickness skin from the thigh. (b) Graft using retroauricular skin (arrows). The superior color and texture match of retroauricular skin is quite evident. Fig. 55.5 A cutaneous defect (a) closed with primary closure (b). Anterior lamellar skin defects may or may not involve the underlying orbicularis muscle, and reconstruction should ideally account for all missing layers to maintain appropriate eyelid volume. If orbicularis is missing, a skin–muscle flap can be used in reconstruction to account for the volume deficit. Small defects should be closed primarily when possible, after undermining adjacent tissue (Fig. 55.5). Larger defects that can be closed primarily may require debulking of the orbicularis to prevent tissue bunching or to allow for closure using a skin–muscle flap. The eyelids are particularly sensitive to vertical vector forces. These changes lead to eyelid retraction or cicatricial ectropion and symptoms of ocular irritation. These vertical vectors are particularly relevant in situations such as with skin graft contraction, primary closures that recruit tissue in a vertical fashion, and bulky myocutaneous flaps involving the midface that are not adequately suspended to the periosteum. Horizontal laxity of the eyelid adds an additional layer of complexity, because lax lids are even more sensitive to the effects of vertical vector forces. Tightening the lower eyelid with a slight supraplacement at the level of the lateral canthus will provide additional support. This can be achieved through a lateral canthopexy or lateral tarsal strip procedure. When choosing an approach to reconstruct anterior lamella, adjacent tissue transfers using local flaps should be favored over full-thickness skin grafts, because the former best address the concerns mentioned previously. In addition, the robust blood supply in the periocular region facilitates a higher success rate. The use of a tissue expander can also be considered, but it can be temporarily disfiguring and requires staged surgery over weeks to months to allow for adequate expansion. Skin grafting should be reserved for reconstruction that is temporizing or when a more extensive adjacent tissue transfer reconstruction is not possible or is undesirable based on comorbidities or patient preferences. Full-thickness grafts are preferred over split-thickness grafts, because they are less prone to contraction and textural abnormalities, are more durable, and do not result in as significant a volume deficit. Scars in the periocular region can affect dynamic function of the eyelids by causing cicatricial ectropion, retraction, or lagophthalmos. However, even when not causing functional lid abnormalities, scars in the periocular region can be disfiguring if they are hypertrophic or if they have a pigmentary or textural mismatch with the surrounding tissue. Although surgical scar revision always remains an option, many nonsurgical options exist for scar rehabilitation. Conservative options that can mildly improve or help prevent undesirable cicatrization include eyelid massage and silicone strips or gel. Intralesional injections with an antifibrotic agent (e.g., 5-fluorouracil) and/or a steroid (e.g., triamcinolone) are useful adjuvants that modulate the wound-healing process and flatten scars while improving their pliability5,6 (Fig. 55.6). These injections can be performed as early as 2 to 4 weeks after surgery on a monthly basis. Injections should be performed slowly and in a retrograde fashion to prevent intravascular complications such as blindness from retrograde flow of medication into the ophthalmic artery with subsequent retinal artery occlusion and blindness.7 Care should also be taken when injecting high-dose steroids in darkly pigmented individuals, because this can cause hypopigmentation. Fig. 55.6 (a) Eyelid cicatrix that formed after periocular trauma. (b) Intralesional injection of triamcinolone and 5-fluorouracil is performed in a subcutaneous plane with a 27-gauge needle. (c) Marked improvement after full-thickness retroauricular skin graft and three cycles of intralesional injection. Fig. 55.7 Cicatricial ectropion managed medically. (a,b) Before treatment. (c,d) After one round of ablative fractional laser resurfacing with laser-assisted delivery of 5-fluorouracil. (e,f) After a second round of treatment. Laser scar rejuvenation can be performed using a fractional ablative laser (e.g. CO2)8; erbium-doped: yttrium aluminum garnet (Er:YAG); or yttrium, scandium, gallium, and garnet (YSGG) lasers to improve scar thickness, pliability, dyschromia, or textural abnormalities. Pulsed-dye lasers can also be used simultaneously to help eliminate scar redness and telangiectasias. Multiple sessions spaced approximately 1 to 3 months apart yield the best results. Fractional ablative lasers can be immediately followed with topical laser-assisted delivery of steroids or 5-fluorouracil to the dermis9 (Fig. 55.7). Standard postprocedural precautions after ablative laser procedures should be used, including antiviral prophylaxis to prevent herpes simplex virus reactivation. Finally, if surgical revision is required, use of nonabsorbable sutures that induce minimal inflammation (e.g., polypropylene or nylon) and gentle eversion of the wound edges will help minimize recicatrization. Postoperatively, patients should be counseled to avoid sun exposure, wear ultraviolet-filtering sunglasses, and apply sunscreen. Identification of ectropion is fairly straightforward. However, delineating the cause of ectropion poses a bigger challenge, particularly in situations that are multifactorial. A thorough examination of the ocular adnexa will help reveal the cause or causes. One helpful diagnostic technique involves placing the lower lid on superior traction. Sufficiently scarred tissue and tissue tethered to the orbital rim will be resistant to gentle manual elevation of the lower eyelid (Fig. 55.8). A patient with cicatricial changes of the anterior lamella of the lower lid will also have worsening of ectropion on upgaze or with mouth opening. The eyelid should also be evaluated for concomitant horizontal laxity using the lid distraction and “snap-back” tests, and horizontal tightening should be performed when indicated. Finally, the surgeon should examine the midface to determine to what degree the midface can be lifted superiorly to restore support and recruit anterior lamella for the lower lid. Mild cases of retraction and ectropion that occur in the early postoperative period can be managed as described previously in the management of superficial scars. In cases of cicatricial ectropion that are of moderate severity, a lateral tarsal strip and suborbicularis oculi fat (SOOF) lift may be adequate to reposition the lid margin and recruit anterior lamella from the midface. More severe cases require a full-thickness skin graft to restore anterior lamella to the lower lid, and this can also be performed in combination with other techniques. Fig. 55.8 Assessing the adequacy of the vertical lamella. (a) A patient with lower lid retraction. (b) Gentle pressure on the orbital rim alleviates the retraction and suggests there is adequate anterior lamella. Addressing the posterior lamella will resolve the retraction. The best incision to release an eyelid cicatrix is through a subciliary (lower lid) or supraciliary (upper lid) approach, because the adjacent eyelashes help to hide the resulting scars. After marking the incision, a 4–0 silk traction suture is placed through the Meibomian gland orifices of the lid. The incision is made, and dissection is directed in the suborbicularis oculi fascial plane. Once the entirety of the cicatrix has been released, the eyelid will be well apposed to the globe. The surgeon assesses this intraoperatively by releasing tension on the traction suture. The defect can then be closed with a myocutaneous flap or with a full-thickness skin graft. When sizing the skin graft, oversizing by approximately 25% larger than the anterior lamellar defect (with the eyelid on gentle stretch) helps anticipates future graft contracture. A Frost suture or a tarsorrhaphy can further keep the eyelid on stretch for the first few weeks after reconstruction to counter the vertical contractile forces from the healing skin graft (Fig. 55.9). Similarly, when creating myocutaneous flaps, the flap can be sized to slightly overcorrect the vertical tissue deficiency, particularly for horizontally oriented flaps. Bulky midface flaps, such as Mustardé flaps, are subject to gravitational forces and benefit from robust suspension. This can be achieved by slightly supraplacing and anchoring the flap to the periosteum of the orbital rim (Fig. 55.10) or by securing the flap to the orbital rim through drill holes. If the ectropion is still manifest after scar release, the surgeon will need to reassess and address other causes of ectropion that could be playing a more significant role than previously realized. Fig. 55.9 (a) Cicatricial ectropion after right cheek reconstruction (arrows). The patient has retraction and ectropion from vertical lamellar deficiency. (b) The ectropion became more manifest in upgaze. (c) The scar was released through a subciliary approach and an oversized full-thickness supraclavicular skin graft. The eyelid is shown on stretch with a Frost suture. (d) The patient has significantly improved position of the lower lid. Fig. 55.10 Mustardé flap. (a) The flap has been created. (b) Periosteal bites are taken (arrows) of at least 2 or 3 points along the orbital rim using 3–0 or 4–0 polypropylene suture. (c) The flap is better supported against the gravitational pull on the lower lid. Fig. 55.11 A large defect (a) repaired with myocutaneous advancement of the upper eyelid and a midline forehead flap (b). (c) Necrosis of the distal midline forehead flap several weeks postoperatively. (d) After 3 months of observation, the cosmetic and functional outcomes are acceptable. Flap and graft failures are frustrating complications but fortunately are uncommon in the periocular region because of the robust and redundant blood supply. Any concern for graft failure should be followed closely. Prophylactic oral antibiotics and topical ophthalmic antibiotic ointment help prevent bacterial superinfection. The role of hyperbaric oxygen has not been clearly established; however, given its low risk profile, a referral for treatment can be considered. Necrotic grafts are débrided and allowed to granulate. These wounds tend to cicatrize and may require staged surgery, revision surgery, or other interventions for scar rehabilitation (Fig. 55.11). As in other parts of the body, skin grafts are more likely to fail than local flaps given their dependence on the underlying vascular bed. Skin grafts can be risky in the setting of concomitant posterior lamellar reconstruction, because most options for posterior lamellar reconstruction are avascular tissues (e.g., hard palate grafts, free tarsal plate grafts, cartilage grafts, donor sclera, or acellular collagen matrices). The key to a successful skin graft lies in maximizing blood supply to the avascular graft. After ensuring a healthy vascular bed, the skin graft should be thinned to the point that dermal appendages are identified. Fenestrating the skin graft, placing bolster sutures, and applying a pressure dressing all serve to minimize the accumulation of serosanguinous fluid that can accumulate at the graft–host interface (Fig. 55.12). Application of the pressure dressing requires special care to ensure that the eye is closed while it is applied. A dressing placed over an open eye can cause corneal abrasions and will desiccate the ocular surface. The role for postoperative systemic antibiotics has yet to be fully examined. In contrast, local flaps and tissue advancements are perfused by a robust network of subcutaneous vessels. In addition to optimizing systemic medical conditions, ensuring that local flaps do not exceed a length-to-width ratio of 2:1 will reduce the risk of flap necrosis. Minimizing tension on the wound and avoiding excessive cautery will also help maintain peripheral perfusion. Axial flaps such as the median, paramedian, and midline forehead flaps are used with much less regularity for eyelid reconstruction. Maintaining the integrity of any source vessel and avoiding excessive flap rotation around the pedicle (usually under 90 degrees) will preserve vessel patency and prevent kinking. Preoperative Doppler ultrasonography can be useful to delineate the course of the supraorbital and supratrochlear arteries. Identification of large bleeders should be addressed before securing the flap into the defect, because pressure from a postoperative hematoma may compromise blood flow. Flap division and thinning should be delayed by at least 3 weeks.
55
Eyelid Reconstruction
Anatomy
Key Components of Orientation
Apposition of the Eyelids to the Globe
Horizontal Stabilization
Proper Vertical Positioning of the Upper and Lower Lids
Key Components of Function
Adequate Innervation of the Orbicularis Oculi Muscle without Mechanical Obstruction

Adequate Positioning and Function of the Levator Palpebrae Superioris without Mechanical Obstruction
Avoiding Unfavorable Results and Complications in Eyelid Reconstruction
Surgical Planning
Repairing the Anterior Lamella
Color and Texture Match
Graft and Flap Thickness
Vertical Lamellar Support
Complications in Anterior Lamella Repair
Superficial Scar Formation


Cicatricial Ectropion
Local Flap and Skin Graft Necrosis
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine