Eyelid (Cancer and Reconstruction)
Description
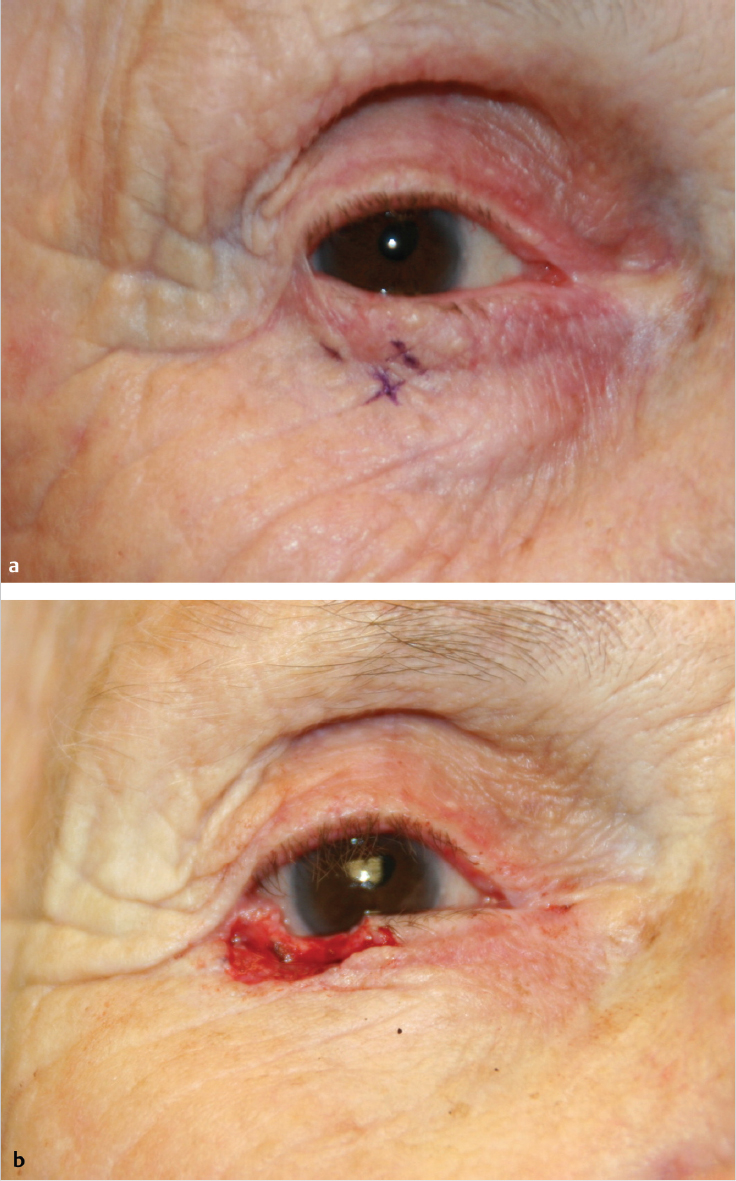
Basal cell carcinoma of lower eyelid with poorly defined margins (e.g., good candidate for Mohs micrographic surgery).
Full-thickness defect of lower eyelid
~ 50%, including lid margin and entire height of tarsus.
Contiguous skin and muscle defect extending to cheeklid junction.
Medial and lateral canthal tendons intact with no evidence of lacrimal system involvement.
Work-up
History
History of ophthalmologic conditions, including dry eye and excessive tearing.
Personal or family history of skin malignancy or significant sun exposure.
History of previous periorbital surgery or trauma.
Physical examination
Divide the periocular region into “zones” (Fig. 8.2).
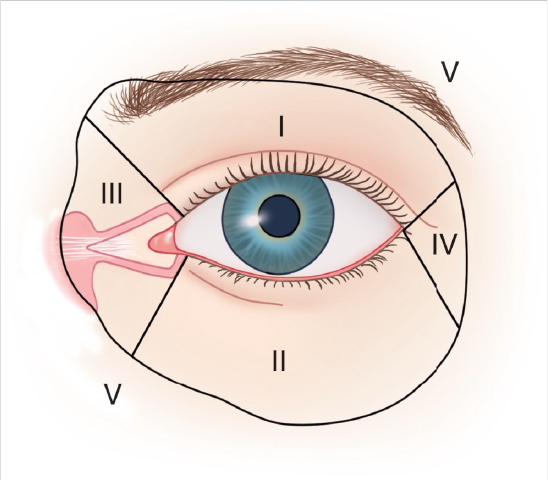
Zones of the eyelid.
Determine layers that have been lost.
Full or partial thickness.
Skin, muscle, tarsus, conjunctiva.
Evaluate canthal support and suspected involvement of lacrimal system.
Identify viable elements available for reconstruction (i.e., skin, muscle, tarsus, conjunctiva).
Evaluate eyelid function.
Diagnostic studies
Establish the diagnosis: If it was not done earlier, an incisional biopsy should be performed at initial visit to confirm the pathology.
Confirm negative pathologic margins following initial resection before attempting significant reconstruction.
Magnetic resonance imaging: Useful adjunct in determining extent of tumor and lymph node status in cases of aggressive tumor histology (e.g., perineural invasion or deeply invasive tumors).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


