Key Points
- ▪
Treatment of advanced lymphedema remains a challenge in reconstructive surgery. Surgical management with excisional procedures is indicated in select patients when conservative measures have failed.
- ▪
Based on an improved knowledge of vascular anatomy and understanding of perforator flap surgery, radical reduction of lymphedema with preservation of perforators applies an excisional approach and microsurgical techniques to the radical reduction of lymphedema.
- ▪
Chen-modified Charles procedure consists of the association of the traditional Charles technique with the lymph node flap transfer. Chen-modified Charles procedure prevents potential complications of the traditional technique, such as recurrent infection and aggravation of the lymphedema.
Introduction
Lymphedema refractory to nonoperative management may require surgical procedures. There are several different surgical approaches to the treatment of lymphedema. Classically, the surgical methods are categorized as physiological and excisional procedures. The physiological procedures attempt to restore or improve lymphatic flow, whereas the excisional procedures aim to decrease the lymphatic load by removing the diseased tissue. This resection approach or debulking procedure involves excision of the excess subcutaneous tissue, and may or may not include the excision of overlying skin, which is known as the Charles procedure. (See Table 11.1 .)
| Stage | Proposed Treatment | |
|---|---|---|
| I | Sentinel decompensation stage, the lymphatic load exceeds lymphatic transport capacity, intralymphatic pressure builds, flow stagnates and valvular incompetence occurs | Nonsurgical treatment |
| II | Brief compensation phase, all lymphatic channels are recruited for drainage. Dermal back flow, mild edema and occasional erythema. Patient is unaware with soft skin | Nonsurgical treatment or Intermittent positive pressure pumping |
| III | Fibroblasts, monocytes, adipocytes and keratinocytes increase in the tissue, along with episodes of infection | |
| IIIA | Symptoms are obvious, but swelling can be improved after rest | Physiological procedures: lymph node transfer or lymphatico-venous anastomosis |
| IIIB | Non-reversible changes are initiated | Lymph node transfer or RRPP ∗ with or without liposuction |
| IVA | Fibrovascular proliferation, brawny leather-like skin, crypts and cutaneous ulcers | Radical excision: Charles procedure with or without lymph node transfer |
| IVB | Stage IVA + severely affected toes; repeated episodes of cellulitis, verrucous hyperkeratosis, deformity or osteomyelitis | Charles procedure and toe amputation with or without lymph node transfer |
In this chapter, we will describe the following excisional methods:
- ▪
Radical reduction of lymphedema with preservation of perforators (RRPP)
- ▪
Chen-modified Charles procedures with vascularized lymph node flap transfers.
RRPP
Concepts
The concept of the excisional approach is removal of significant amounts of skin and subcutaneous tissue since the pathology of lymphedema is limited to these components. This approach serves to slow down the increase in fibroblasts, monocytes, adipocytes and keratinocytes in the affected tissues. Moreover, reduction in limb size also serves to facilitate nonsurgical management by making it easier to fit compressive garments and clothes. Studies have shown that, by decreasing the size of the affected limb, there is a decrease in the frequency of infections, which can eventually prevent further destruction of the lymphatics and subsequent disease progression. Therefore, the main goal of lymphedema treatment should be to decrease the size of affected limb and prevention of infection. This technique can be used for the upper and lower limbs.
The RRPP is based on an improved knowledge of the skin perforators, allowing for more radical excision techniques while still preserving perfusion to the angiosomes. Of the many excisional procedures available, the RRPP has been proven to result in an acceptable, sustainable outcome. This technique is particularly useful in lower limb lymphedema, which has shown an overall reduction of 52%, rather than upper limb lymphedema.
Regional Anatomy
The blood supply to the medial and lateral skin parts of the lower limb is originated from two or three of the following sources:
- ▪
On the medial aspect of the leg, the skin perforators from the posterior tibial artery are usually located between 9–12 cm, 17–19 cm, and 22–24 cm proximal to the medial malleolus.
- ▪
On the lateral aspect of the leg, most of the skin perforators are septocutaneous and are derived from the peroneal artery. These are the usual perforators supplying the skin paddle of the fibula osteocutaneous flap.
- ▪
As the medial and lateral skin flaps are bipedicle in design, there is blood supply from above the knee and below the ankle.
- ▪
On occasions, one of the two major perforators supplying the medial and lateral skin flap is originated from the anterior tibial artery.
The blood supply to the medial and lateral skin of upper limb is derived from one source in the arm and two sources in the forearm. The bi-pedicle design of the medial and lateral skin flaps ensures blood supply from above the elbow and below the wrist. The arm is nourished by septocutaneous or musculocutaneous perforators, or by direct perforators arising from the brachial artery. The forearm is nourished by septocutaneous or musculocutaneous perforators or direct perforators arising from the radial, ulnar and posterior interosseous arteries. The radial artery gives off nine to 17 fasciocutaneous branches, next to the radial recurrent artery, which arises near the origin of the radial artery. The superficial palmar arch arises just distal to the wrist. The ulnar artery, next to the anterior and posterior ulnar recurrent arteries and the common interosseous artery, gives off three to five fasciocutaneous branches running between the flexor carpi ulnaris and the flexor digitorum superficialis.
Surgical Design
The incisions are designed with several considerations in mind. In the lower limb, the incisions are placed at the junction between two angiosomes, notably those of the posterior tibial and peroneal artery. Posteriorly, the incision is made between the two heads of gastrocnemius muscle. Skin incisions are linear and oriented vertically and a skin bridge is preserved to avoid circulation compromise to the central part of the skin flap. The markings on the leg consist of two anterior and two posterior ellipses positioned obliquely and parallel to each other. All the skin has blood supply from one or more perforators, identified previously with a hand-held Doppler. A skin bridge with a minimum width of 4 cm separates the ellipses, both anterior and posterior. The elliptical markings serve two purposes. They allow for skin excision without dog-ears, and provide good access to the subcutaneous layer around the circumference of the leg ( Figure 11.1 ).

In the upper limb, the first incision is placed between the angiosomes of the radial artery and the ulnar artery. Posteriorly, the incision is also made between the two above angiosomes. A line is drawn from 1 cm below the center of the antecubital fossa to the tubercle of the scaphoid on the volar forearm. This surface marking represents the radial artery and anterolateral intermuscular septum. A second line is drawn from the medial epicondyle of the humerus to the lateral edge of the pisiform. The ulnar artery also commences from 1 cm below the center of the antecubital fossa to a point on the second line that is at the junction between the proximal and middle thirds. From this point on the second line, the ulnar artery continues to the pisiform. The markings of the flap consist of an anterior and a posterior ellipse with a 30° angle. The anterior (on the volar aspect) ellipse is designed between the surface anatomical lines corresponding to the radial and ulnar arteries, preserving their major septocutaneous branches. The posterior (dorsal aspect) ellipse is designed at the central area along the axis of the forearm. If a debulking procedure of the arm is required, an ellipse is designed along the medial aspect. The size of the ellipse depends on the size of the extremity and the expected amount of resection after the debulking procedure. The medial side of the arm is preferred for the resection, as there is usually more redundant tissue, and the resulting scar is less conspicuous, providing a better cosmetic result.
Following elevation of skin flaps and resection of the lymphedematous tissue, there is always significant redundancy in the resultant skin envelope. The excess skin is subsequently excised. To minimize dog-ears and preserve the central skin bridge, the excision is directed at an angle that accounts for the 30° angle of the elliptical design.
Patient Selection
Patient selection for this procedure is critical. Lymphedema presents with a progressive course that begins as intermittent swelling of the extremity. Later, the patient has more persistent swelling that may be improved with conservative measures; thereafter, this proceeds to a more permanent swelling that is persistent despite all conservative treatments. Therefore, the indications of RRPP are as follows ( Table 11.1 ):
- ▪
stage IIIb patients who failed medical treatment; patients not fit for just lymph node transfer
- ▪
occasionally for patients with advanced disease who are destined to undergo Charles procedure (but have the higher risk of potential complications)
- ▪
as an adjunct to other treatment modalities (e.g., lymph node flaps).
Preoperative Consideration
Bed rest at home with bathroom privileges is encouraged for five days prior to surgery. The affected extremity is measured on the morning of surgery and compared with tape measurements from the last office visit. If there is no significant decrease (less than 20%) of the circumference, the surgical procedure is postponed until the patient’s compliance is assured. Antibiotics (first-generation cephalosporin) are administered during anesthetic induction and continued for three days postoperatively.
Surgical Techniques for RRPP
The patient is placed in a supine position on the operating table. A pneumatic tourniquet is placed as proximally as possible on the extremity.
In the lower limb, perforating skin vessels from the posterior tibial and peroneal arteries are mapped with hand-held Doppler probe above the levels of the medial and lateral malleoli respectively. In the middle of the leg, one large perforator is identified on the medial and lateral side, supplying the medial and lateral skin flaps respectively. Normal diameter of these perforators ranges from 1–3 mm in diameter for both artery and vein. Two cm of fascia and fat is preserved around the two main perforators in the medial and lateral skin flaps. If several large perforators are found, the one located close to the center and far from the preserved medial and lateral tissue over the malleoli is marked.
The ellipse represents the area of skin that will be excised after preservation of skin perforators. The skin flap is retracted by two skin hooks and the subcutaneous fat grasped using Allis clamps. The subcutaneous fat is tangentially excised until the skin flap is approximately 5 mm thick, preserving the subdermal venous plexus and minimal subdermal fat. The size of these ellipses depends on the size of the leg and the expected amount of debulking procedure. One should initially make conservative markings and if necessary, more skin can be resected after preservation of skin perforators. The leg is partially exsanguinated, which allows for better visualization of the perforators to the skin. The incisions are made down to the level of the deep fascia overlying the muscle compartments. All layers above this fascia are elevated as one unit, on both the medial and lateral aspects of the leg.
Care is taken to preserve the superficial peroneal nerve and sural nerve. Loupes magnification is used for this part of the procedure. The subcutaneous tissue and skin around the medial and lateral malleoli is left untouched. Meticulous surgical technique is necessary throughout the procedure to minimize unnecessary trauma to the skin flaps. Viability of the skin flaps is assessed by wiping the skin edges with a sponge and observing dermal bleeding. The tourniquet is deflated and hemostasis is performed. The skin ellipses along with underlying subcutaneous fat are then excised. The resultant wound edges are approximated to see if further skin excision is possible. Otherwise, suction drains are introduced and the wounds are closed.
In the upper limb, the presence of radial and ulnar arteries is confirmed by using a hand-held Doppler probe. The ellipse of skin marks the area of skin that needs to be excised for the debulking of the forearm. The size of these skin ellipses depends on the size of the extremity and the expected amount of resection for debulking. Like the leg, the elliptical markings serve two purposes. They allow for a skin excision without dog-ears, and provide wider access.
Care is taken to preserve the medial and lateral cutaneous nerves of the forearm, in particular the cutaneous branch of the ulnar nerve around the elbow. The vascular branches are identified during elevation of the medial and lateral skin flaps.
The areas on the medial and lateral aspect of the forearm, around the wrist, are left untouched. Using two skin hooks, the skin flap is elevated. The incisions are made down to the deep fascia. All the tissue layers above the fascia are elevated and the procedure is carried out in the same manner as already described. The large veins are preserved as much as possible. Then, using Allis clamps, the subcutaneous fat is grasped and pulled backward and downward. A minimal thickness of 5 mm of skin flap is raised, preserving the subdermal venous plexus and minimal subdermal fat. The tourniquet is deflated for hemostasis. The skin is approximated and assessed to see if any further skin excision is needed. The skin is then closed over suction drains.
Postoperative Care
Postoperative dressings include an inner loose elastic bandage and an outer tight, compressive elastic bandage. The outer bandage is removed two hours after the procedure in the post anesthesia recovery unit. Patients usually remain in hospital for 3–5 days and are then discharged, with the recommendation to use a compression stocking and to elevate the extremities for the next two weeks.
Outcomes
In our experience, there is minimal operative morbidity or complications requiring operative intervention. Overall, extremity reduction was statistically significant when pre- and postoperative measurements were compared with the unaffected contralateral limb.
In the lower limb, the average percentage of circumferential reduction for all patients above the knee was 51%, below the knee 66%, at the ankle 44%, and at the level of the foot 41%. The overall circumferential reduction for the lower limb lymphedema was 52%. Complications consisted of cellulitis in 20% of the patients who received only RPPP without other procedures, seroma in 6.7%, and hematoma in 6.7%. There was no incidence of wound breakdown or skin flap necrosis. In 13.3% of the patients, there were complaints of numbness in the extremity, which had not resolved within a year. Most patients complained of a transient numbness of the leg that resolved within six months.
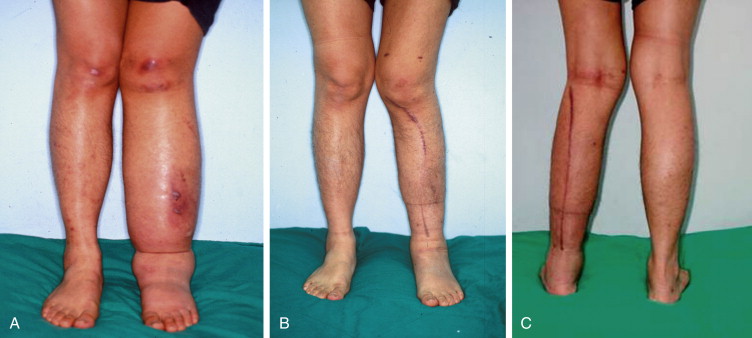
For the upper limb, the average circumferential reduction above and below the elbow, at the wrist, and at the hand were 15.1%, 20.7%, 0.5%, and 3.6%, respectively. Statistical analysis showed significant circumference reduction above and below the elbow but not at the wrist and at hand. There were no cases of wound breakdown, skin necrosis, or cellulitis in the postoperative period. Mild numbness confined to the vicinity of the surgical incisions was a complaint in 36.3% of the patients. All lymphedema reductions were completed in one stage ( Figure 11.2A–C ).