Excision of Soft Tissue Tumors of the Thigh
Raffi S. Avedian
DEFINITION
Soft tissue sarcomas are malignant tumors that arise from mesenchymal cells and are classified according to their cell of origin such as the muscle, tendon, or fat.
Peripheral nerve sheath tumors arise from neural crest cells but are typically grouped with sarcomas because of similarities in location, natural history, and treatment.
The World Health Organization groups soft tissue sarcomas into ten categories based on the tissue of origin.
Most sarcomas occur in a deep location meaning below the muscle fascia, whereas one-third of sarcomas occur in a subcutaneous location.
Patients with soft tissue sarcomas and patients with benign tumors often present with the same chief complaint of having a soft tissue mass.
Rendering an accurate diagnosis prior to surgery is important because the treatment plan may vary based on the nature of the diagnosis. For example, a benign tumor may be monitored or removed with a simple excision, whereas in the case of a sarcoma, the goal of surgery is to remove the tumor with a wide margin.
With appropriate planning, radiotherapy and/or chemotherapy is often incorporated into the treatment plan either before or after definitive surgery.1
ANATOMY
The critical anatomic structures that should be preserved when performing an excision of tumor in the thigh are the femoral artery, sciatic nerve, and femoral nerve.
The common femoral artery enters the thigh under the inguinal ligament. As it travels distally, it gives several branches, the largest of which is the profundal femoral artery (PFA). This branch travels on top of the adductor brevis until the muscle inserts onto the linea aspera at which point the distal half of the PFA continues just posterior to the femur.
Several perforator branches from the PFA pierce the lateral intermuscular septum and go into the anterior compartment. In most patients, limb salvage can be performed even if the PFA is ligated near its takeoff from the common femoral artery.
The superficial femoral artery (SFA) is the most important blood vessel when considering tumor excision. It must be preserved or reconstructed if excised to maintain viable limb perfusion. As the SFA travels distally, it is located on the anterior surface of the psoas, adductor longus, and then adductor magnus until it courses through the adductor canal into the popliteal fossa. The sartorius muscle acts as a cover to the superficial femoral vessels throughout the middle of the thigh.
There are three muscle compartments of the thigh: anterior, medial, and posterior.
The sciatic nerve travels in the posterior compartment. It branches into the common peroneal nerve, which can reliably dissected and found just medial and anterior to the biceps femoris in the popliteal fossa. The tibial nerve portion of the sciatic nerve stays midline with the popliteal vessels.
The femoral nerve divides into several branches that spread out and innervate the anterior compartment muscles soon after passing under the inguinal ligament. Unlike the sciatic nerve, which can be isolated throughout the thigh, the femoral nerve is rarely identified during tumor removal because it branches so proximally.
PATHOGENESIS
The mechanism for sarcoma formation is not known.
Risk factors for sarcoma development include radiation exposure, radiotherapy, pesticide exposure, and hereditary conditions including Li-Fraumeni syndrome and neurofibromatosis.
NATURAL HISTORY
All sarcomas have the potential for local recurrence and metastasis.
Tumor variables that are associated with increased risk of metastasis include high grade and large size (greater than 5 cm).2
Lungs are the most common location of metastasis.
PATIENT HISTORY AND PHYSICAL FINDINGS
Determining when the mass was first noticed and how rapidly it is growing can help the clinician differentiate between benign and malignant tumors.
The presence of pain is often associated with a benign tumor such as a schwannoma or vascular malformation and may not be present with sarcomas until late in the disease course.
Determining the size of the tumor, manual muscle strength testing, and sensory examination are useful to determine if there is neurological compromise. Limb edema assessment and pulse examination can help determine if the tumor is causing vascular or lymphatic compromise.
Range of motion testing and gait assessment are helpful in assessing a patient’s mobility and functional status to guide a perioperative and postoperative counseling.
IMAGING
Magnetic resonance imaging is the modality of choice for soft tissue tumor evaluation.3
Fat-sensitive images such as T1-weighted sequences are best for identifying critical anatomic structures such as nerves and vessels (FIG 1).
Fluid-sensitive images including T2-weighted and STIR sequences highlight pathology very well.
Contrast-enhanced sequences are used to differentiated cystic from solid areas in tumors and identify reactive peritumoral edema, which will be high signal on fluid sequences but not enhance with contrast.
Some benign tumors such as lipoma and schwannoma may be diagnosed on MRI; however, most soft tissue tumors require a biopsy for diagnosis.
DIFFERENTIAL DIAGNOSIS
Benign tumors
Sarcoma
Lymphoma of soft tissue
Infection/abscess
SURGICAL MANAGEMENT
The appropriate treatment for any musculoskeletal tumor is based on its diagnosis and natural history.
Performing a surgery without consideration of the diagnosis and the appropriate margin may cause harm to patients.4
In cases where MR imaging is not diagnostic, a biopsy should be performed.
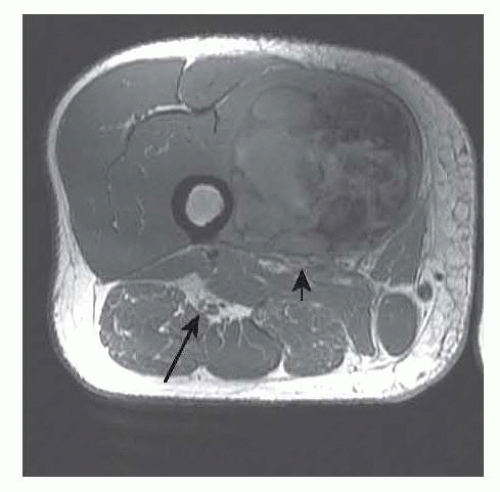
FIG 1 • Axial T1-weighted image demonstrating compartments of the thigh and relevant anatomy of the thigh. The arrow points at the sciatic nerve and the arrowhead at the femoral vessels, and there is a sarcoma in the vastus medialis.Related posts:
 Fasciotomy of the Thigh, Lower Leg, and Foot
Fasciotomy of the Thigh, Lower Leg, and Foot
 Bony Reconstruction of Foot and Ankle (Bone Grafts)
Bony Reconstruction of Foot and Ankle (Bone Grafts)
 Vascular Reconstruction of Lower Extremity, Foot, and Ankle
Vascular Reconstruction of Lower Extremity, Foot, and Ankle
 Tibial Reconstruction
Tibial Reconstruction
 Reconstruction of Femur
Reconstruction of Femur
 Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation
Amputation of the Lower Extremity: Above-Knee Amputation, Below-Knee Amputation, Through-Knee Amputation

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access
