Dermoscopy has been shown in meta-analyses to improve the diagnostic accuracy of melanoma unequivocally compared with naked eye examination and to reduce excision rates of benign melanocytic lesions in clinical trials. Sequential digital dermoscopy imaging (SDDI) allows the detection of dermoscopic featureless melanoma. When used in high-risk individuals or on individual suspicious melanocytic lesions, it has a gross impact for detecting melanoma in clinical practice, with a range of 34% to 61% of melanomas detected exclusively using SDDI in these patients. Furthermore, SDDI has been shown to reduce the excision of benign lesions when used in combination with dermoscopy.
Key points
- •
Dermoscopy improves the diagnostic accuracy for melanoma compared with naked eye examination.
- •
Dermoscopy results in a reduction of excisions in addition to an increased sensitivity for the diagnosis of melanoma.
- •
Sequential digital dermoscopy imaging (SDDI) allowed the detection of suspicious dermoscopic change in melanomas that lack dermoscopic evidence of melanoma at a particular time.
- •
When used in high-risk individuals or on individual suspicious melanocytic lesions, SDDI has a gross impact for detecting melanoma in clinical practice, with a range of 34% to 61% of melanomas detected exclusively using SDDI in these patients.
- •
SDDI has been shown to reduce the excision of benign lesions when used in combination with dermoscopy, in both dermatologists and primary care physicians.
Dermoscopy (dermatoscopy, oil epiluminescence microscopy, surface microscopy) is a technique that uses a hand-held magnification device following the application of a liquid at the skin-device interface or uses cross-polarized instruments. This technique allows the visualization of diagnostic submacroscopic, morphologic key structures of pigmented and nonpigmented skin lesions located in the epidermis down to the upper dermis not seen with the naked eye. In 2008 the evidence-based Clinical Practice Guidelines for the Management of Melanoma in Australia and New Zealand gave the recommendation that training and utilization of dermoscopy is recommended for clinicians routinely examining pigmented skin lesions. This recommendation was given the highest grade (grade A: body of evidence can be trusted to guide practice). The following outlines the evidence leading to this recommendation and the subsequent published literature that further supports it.
Meta-analyses performed on studies in a variety of clinical and experimental settings have shown that dermoscopy improves the diagnostic accuracy for melanoma compared with naked eye examination. The 2 earliest meta-analyses included studies in both prospective clinical and experimental settings, the latter using retrospectively collected photographs. These studies, which were mainly conducted in a specialist setting, demonstrated a relative diagnostic odds ratio 4.7 and 3.7 times higher for dermoscopy compared to naked eye examination. The larger meta-analysis of 13 studies published from 1987 to 2000 showed that diagnostic accuracy for melanoma, expressed as log odds ratio, was 4.0 for dermoscopy versus 2.7 for naked eye examination ( P = .001). The other meta-analysis of 8 studies involving only experienced users found similar results: log odds ratio 4.3 for dermoscopy versus 2.8 for naked eye examination ( P = .008). These 2 meta-analyses showed that dermoscopy is significantly better (49% and 56% ) at discriminating between melanoma and nonmelanoma than naked eye examination.
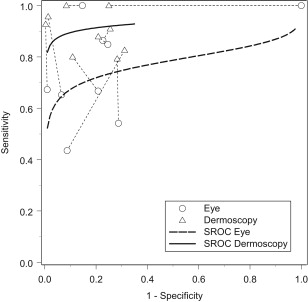
Following these 2 studies, a more recent meta-analysis was performed that restricted the analysis to include only prospective studies on consecutive patients in a clinical setting (published between 1987 and January 2008) ( Fig. 1 ). Nine studies were included in the analysis, which found the relative diagnostic odds ratio for melanoma compared with naked eye examination to be 15.6 (95% CI 2.9–83.7, P = .016). Summary estimates showed the sensitivity was 18% (95% CI 9–27; P = .002) higher than for naked eye examination, but there was no evidence of an effect on specificity.
Like other diagnostic techniques, some training in dermoscopy is needed to achieve improvement in diagnostic accuracy. It has been shown in an experimental setting that dermoscopy may decrease diagnostic performance on pigmented skin lesions for dermatologists without any formal training in the technique. Most of the included studies in the latter described meta-analysis were performed by experienced dermoscopy users, but the participating primary care physicians in one clinical trial had only received a 2-hour teaching session in a simple dermoscopic algorithm for distinguishing benign and malignant tumors.
Although these studies have shown a greater impact in detecting unrecognized melanomas by naked eye examination (ie, improved sensitivity) in comparison with detection of benign lesions, a dramatic effect of dermoscopy on specificity is best examined by its effect on excision rates. In a randomized trial in a specialist setting of naked eye versus naked eye and dermoscopy examination, there was a 42% reduction in patients referred to biopsy in the dermoscopy arm ( P = .01), which is consistent with the retrospective findings of a significant reduction of the benign/malignant ratio of excised melanocytic lesions in clinicians trained in the use of dermoscopy from 18:1 (predermoscopy era) to 4:1 (post-dermoscopy era) ( P = .04). In contrast, nonusers of dermoscopy continued their diagnostic performance without improvement (from 12:1 to 14:1). In a clinical trial looking at the impact of the combination of dermoscopy and sequential digital dermoscopy imaging compared with naked eye examination in primary care physicians, a reduction of 63.5% of benign pigmented lesions excised or referred was achieved ( P <.0005). Recently, in a study looking at the role of dermoscopy in a group of general dermatologists, a significant 9% reduction in excisions of recruited pigmented lesions occurred with the use of dermoscopy.
Such studies showing a reduction of excisions in addition to an increased sensitivity for the diagnosis of melanoma with the use of dermoscopy were crystallized recently in a large 10-year international multicenter survey of the number-needed-to-excise (NNE) values for melanoma detection comparing specialized clinical versus nonspecialized settings. The participating clinics contributed a total of greater than 300,000 cases, including 17, 000 melanomas and 283,000 melanocytic nevi. The overall NNE values achieved in specialized (clinics purely dedicated to skin cancer detection) and nonspecialized clinics in the 10-year period (1998–2007) were 8.7 and 29.4, respectively. The NNE improved over time in the specialized clinics (from 12.8 to 6.8), but seemed unchanged in the nonspecialized clinics. In particular, it was noted that there was a significantly greater number of excised melanomas in the specialized clinics. Although formal data on dermoscopy usage were not obtained, it is reasonable to conclude that dermoscopy had a highly significant impact on the results.
There is now widespread literature on the dermoscopic features of both pigmented and nonpigmented skin tumors. Nevertheless, most evidence-based studies on the effectiveness of the technique have assessed the impact of pigmented skin lesions, more often melanocytic lesions, and in particular, melanoma. It should be noted that in a recent study there was a greater impact on the improvement in the diagnosis of pigmented nonmelanocytic versus melanocytic lesions.
Sequential digital dermoscopy imaging (SDDI) involves the capture and assessment of successive dermoscopic images, separated by an interval of time, of one or many melanocytic lesions to detect suspicious change. This imaging is performed in 2 settings: short-term digital monitoring (over a period of 3 months) for suspicious melanocytic lesions, and long-term surveillance (usually at intervals of 6–12 months). In a recent meta-analysis that grouped both short-term and long-term SDDI together, it was shown the number of lesions needed to monitor one detected melanoma ranged from 31 to 1008 depending on the clinical setting (lower number of lesions needed to monitor for short-term monitoring of suspicious lesions). For every additional month of monitoring, one additional melanoma was detected, with the chances to detect a melanoma during surveillance shown to increase as the length of follow-up extended. Furthermore, the proportion of in situ melanoma and thin melanomas detected by SDDI were higher than expected in the general population.
In 2008 the aforementioned Clinical Practice Guidelines for the Management of Melanoma in Australia and New Zealand gave the recommendation to consider the use of sequential digital dermoscopy imaging to detect melanomas that lack dermoscopic features of melanoma. This recommendation was given a grade B: body of evidence can be trusted to guide practice in most situations. The basis of the recommendation was 4 high-level diagnostic studies that consistently showed that SDDI allowed detection of suspicious dermoscopic change in melanomas that lack dermoscopic evidence of melanoma at a particular time. In these studies featureless melanomas were more frequently found with short-term versus long-term SDDI. Importantly, in one study that reviewed the lesion baseline images, there was no difference in the prevalence of specific dermoscopy melanoma features found in melanoma versus nevi, highlighting the importance of change to detect featureless melanomas.
Since the Australian and New Zealand guidelines have been published, there have been many studies describing the impact of SDDI in clinical practice. In one cohort of moderate-risk to high-risk patients, 34% of melanomas were found exclusively using SDDI. In a follow-up study, these researchers showed lower risk individuals (those with >50 nevi but <4 atypical nevi) had a high benign/melanoma ratio (79:1) of excised changed lesions using SDDI, compared with higher risk groups (atypical mole syndrome 15:1, and familial atypical mole and multiple melanoma syndrome 4:1). The conclusion of these researchers was long-term SDDI of nevi is less efficacious in lower risk individuals; this has also been noted by others.
In a prospective observational study of dermatologists comparing the use of dermoscopy versus dermoscopy with SDDI (short-term and long-term), there was a significant improvement in the excised benign/melanoma ratio in the group using SDDI (8.1 vs 2.4). Furthermore, 55% of melanomas were detected exclusively by SDDI in the latter group. In this arm, melanomas detected with SDDI were significantly thinner than those detected without SDDI. The 10-year experience of following another cohort of high-risk melanoma patients using total body photography and SDDI (short-term and long-term) showed 61% of melanomas were detected with SDDI. In contrast with the previous study, there was no difference in the thickness of melanomas detected with SDDI or without.
As mentioned previously, in a sequential intervention clinical trial in Australian primary care physicians, the combination of dermoscopy and short-term SDDI reduced excision/referrals of benign lesions by 64%, with the benign/melanoma ratio of excised/referred lesions decreasing from 9.5:1 to 3.5:1. Furthermore, the sensitivity for the diagnosis of melanoma using the techniques nearly doubled compared with baseline naked eye examination (72% vs 38%). When isolating the effect of SDDI by analyzing only those lesions undergoing monitoring, there was a gross increase in sensitivity for the diagnosis of melanoma (73%) compared with only 18% achieved with naked eye examination. This increase in sensitivity occurred without any loss of specificity.
In conclusion, dermoscopy unequivocally improves the diagnostic accuracy of melanoma compared with naked eye examination. It has also been shown to reduce excision rates of benign melanocytic lesions. SDDI allows the detection of dermoscopically featureless melanoma. When used in high-risk individuals or on individual suspicious melanocytic lesions, SDDI has a gross impact for detecting melanoma in clinical practice, with a range of 34% to 61% of melanomas detected exclusively using SDDI in these patients. Furthermore, SDDI has been shown to reduce the excision of benign lesions when used in combination with dermoscopy, in both dermatologists and primary care physicians.
Financial Disclosures: None.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


