Physical examination is the most important element of preoperative assessment and planning for both reconstructive and cosmetic procedures. Reviewing photographic images with the patient can be helpful when discussing aesthetic concerns and goals.
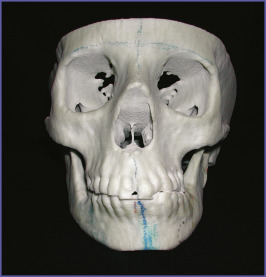
All faces are asymmetric. Asymmetries are usually subtle but, with sufficient scrutiny, detectable ( Fig. 2.1 ).

Their recognition preoperatively is important to both the surgeon and the patient. The patient’s asymmetry should be pointed out during the preoperative consultation so that the patient can anticipate asymmetry in the postoperative result. Preoperatively, the asymmetries belong to the patient. Postoperatively, if not identified before the surgery, they are attributed to the surgeon.
As asymmetries become more severe, it is important to recognize that they are more complex than relative skeletal deficiencies or excesses. Rather, they reflect three-dimensional differences that are most easily conceptualized as twists of the facial skeleton.
Always describe a patient’s asymmetry during preoperative consultation.
Radiologic Examination
Most aesthetic procedures are done without preoperative radiologic assessment. In general, the size and position of the implant are largely aesthetic judgments. Cephalometric X-rays are most often used for planning chin and mandibular augmentation surgery. These studies define skeletal dimensions and asymmetries as well as the thickness of the chin pad.
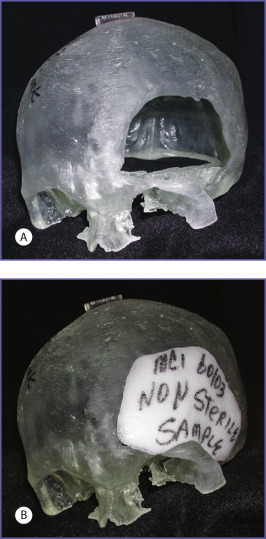
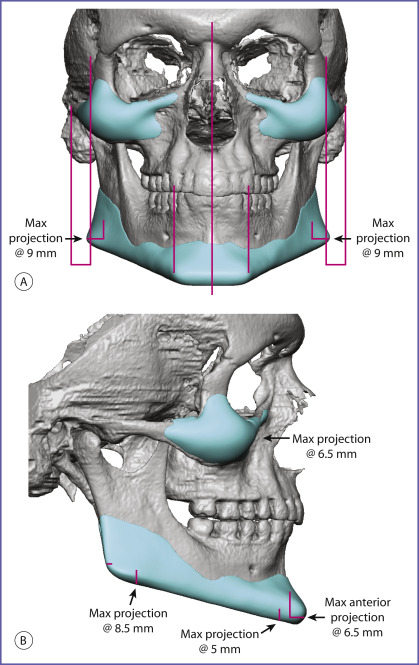
While preoperative radiologic examination is uncommon for purely aesthetic surgery, computed tomographic (CT) evaluation is almost routine for reconstructive procedures. CT scans provide the ability to view the skeleton in different planes and, through computer manipulation, in three dimensions. CT imaging provides digitized information that can be transferred to design software. CAD/CAM implants provide an increased level of refinement in both reconstructive and aesthetic applications. This modality has been used since the 1990s to reconstruct cranial defects. Computer-aided design (CAD) and computer-aided manufacture (CAM) can be used to create life-sized models for surgical planning ( Fig. 2.2 ) and implants customized for the needs of the patient ( Fig. 2.3 ).
The design process can also be conducted virtually as demonstrated in Fig. 2.4 . The CAD/CAM process is the focus of Chapter 14, Chapter 15 .
Cone beam CT scans are available in many dental offices. They have the advantages of less expense and less radiation exposure to the patient. They can provide three-dimensional images of the facial skeleton and are therefore valuable in planning. Because their field is limited and head-positioning devices distort the soft tissue envelope, cone beam CT has a limited role in the CAD/CAM implant process.
Magnetic resonance imaging, invaluable for soft tissue assessment, does not have a role in skeletal evaluation and implant surgery planning.
Facial Measurements
For most reconstructive problems, surgery is performed to return the involved area to its original appearance, or, if that is not possible, to one that is symmetric and accepted as normal. When alloplastic implants are used to make the face more attractive, the aesthetic goal is more arbitrary. Because implant augmentation of the facial skeleton results in measurable changes in facial dimensions and proportions, it is intuitively attractive and appropriate to use facial measurements to evaluate the face and to guide surgery.
Mathematical ideals
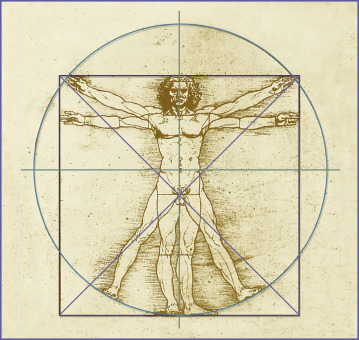
In his book on Leonardo da Vinci’s anatomical drawings, Martin Clayton explains how mathematical ideals influenced classical and Renaissance artists in their perception and depiction of the human body. The ancient Greeks observed that musical notes created by strings whose lengths were in simple numeric ratios were intrinsically pleasing. They extended this concept to spatial intervals and established the concept that harmonic ratios were intrinsically “right” and thus fundamental to the structure of the universe. In the 1st century BC, Vitruvius adapted the proportional concept to the human body. He proposed that the body should be divisible into equal parts, and that all of its units should be expressible in terms of that unit or fractions of the whole. His treatise De architectura , which describes his proportional system, was one of the few classical texts that survived to the Renaissance and became highly influential in the thinking of artists and scholars of that time, including Leonardo da Vinci. Early in his career, Leonardo adopted many of Vitruvius’ ratios. Most of us today associate Leonardo’s anatomic drawings with his rendition of Vitruvius’ ideal proportions for the human body (c.1490–92) whereby “the body when standing with arms stretched fits into a square and, with all limbs splayed, into a circle centered on the navel” ( Fig. 2.5 ).
Leonardo soon found limitations in the use of proportions to depict the human form. By 1500 he abandoned the idea of a single canon of ideal proportion to describe the human body. In the winter of 1510 he collaborated with the Professor of Anatomy at the University of Pavia, Marcantonio della Torre. This relationship provided Leonardo access to human material allowing him to depict human structure with great accuracy. As Leonardo learned human anatomy, he realized that the use of ideal proportions thwarted its accurate depiction. He used proportion as a tool to help describe its form and function rather than as an end to itself.
When the dimensions of normal males and females were evaluated objectively and compared to these artistic ideals, it was found that some theoretic proportions are one of many variations found in healthy normal individuals, including those determined more attractive than most individuals, and some are never found ( Fig. 2.6 ). The neoclassical canons do not allow for facial dimensions known to differ with sex and age. Most of these canons of proportion, for example that the width of the upper face is equal to five eye widths, are interesting but hold for few individuals and cannot be obtained surgically or, if obtainable, only with extremely sophisticated craniofacial procedures.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


