Advances in 3-dimensional (3D) data capture, tracking, and computer modeling now allow for more appropriate measurement and analysis of the face. 3D video not only enables precise analysis of facial symmetry, it broadens our capabilities to accurately study facial volume and facial movement and the forces generated within tissue. Research in facial plastics outcomes has traditionally been evaluated with subjective measures. Current 3D methods are far superior and generate reproducible, accurate, and objective data for such clinical studies. As these technologies become more readily available, there will be a paradigm shift in how aesthetics research is conducted. 3D videography and newer technologies on the horizon will not only change current research methods; they will be much more pervasive in the clinical practice of aesthetic surgeons as they are incorporated into preoperative planning and used to improve patient communication.
The evaluation of the effectiveness of facial plastic surgical procedures has traditionally focused on subjective opinion and retrospective chart reviews. Since 1992, the practice of medicine has seen a shift from relying on expert opinion toward evidence-based medicine, which “de-emphasizes intuition, unsystematic clinical experience, and pathophysiologic rationale as sufficient grounds for clinical decision making and stresses the examination of evidence from clinical research.” A variety of factors have contributed to the movement toward a more objective, evidence-based analysis of surgical outcomes. These factors include:
- 1.
Assessment of rapidly developing, and often costly technological treatment alternatives
- 2.
Third-party payer reimbursement based on outcomes
- 3.
Variation in management plans between different providers.
Research in facial plastic surgery has transitioned toward a focus on creating high-quality outcomes research, integrating the fields of evidence-based “medicine” with facial plastic reconstructive surgery. The measurement tools for such research rely on subjective outcomes (quality of life questionnaires), but also require facial analysis that is quantifiable and comparable to other results. The objective of this article is to describe the state of the science of facial analysis using one of these tools, 3 dimensional (3D) videography.
The assessment of facial features and, thus, surgical outcomes from facial plastic surgical procedures has been largely based on aesthetic observation and preferences, as opposed to measurable data. Artists, architects, and others have studied the contribution of symmetry and proportionality to aesthetic preferences. Five hundred years ago, Leonardo da Vinci emphasized the mathematic proportions of the human face in his famous works. In this last century, the relationships between the craniofacial skeletal structures including Edward Angle’s classification of dental occlusion helped establish the framework for the science of measuring craniofacial dimensions in the midsagittal plane on radiographs, known as cephalometric analysis. Analysis of reconstructive and aesthetic surgical results now includes a new set of objective measurement tools including laser facial scanning, cone beam computed tomography (CT), integrative 3D CT and 3D photography systems (eg, 3DMD, Atlanta, GA, USA), and 3D videography.
Facial structures can be best analyzed either (1) directly by a skilled observer who can use both visual and tactile clues, or (2) indirectly, using images captured of the subject. Once the patient leaves the office, surgeons often rely on photographs or radiographs for preoperative planning and postoperative critique. Cephalometry is limited by a lack of representation of most of the facial soft tissues. In an attempt to address these shortcomings, facial plastic surgeons have shifted their attention to photography. Digital representations remain limited by the fact that they are 2-dimensional (2D) representations of 3D body structures. Standard photography for facial analysis is limited by a variety of factors. For example, proper and consistent lighting are required to allow comparisons of facial depth and contour. Gross and colleagues demonstrated that 2D measurements significantly underestimated distances as compared with 3D analysis.
The dynamic nature of facial animation poses a particular challenge to obtaining meaningful objective data. Changes in facial movement in a postoperative patient with edema, scarring, or muscle weakness are underestimated without a dynamic analysis. A variety of 3D technologies can overcome deficiencies of conventional techniques, including:
- ■
3D cephalometry
- ■
Morph analysis
- ■
Moire topography
- ■
3D computed tomography
- ■
3D magnetic resonance imaging
- ■
3D ultrasonography, laser scanning
- ■
Digital stereo photogrammetry
- ■
3D videography.
The advent of 3D videography allows for a more comprehensive analysis of hard and soft tissue changes including volume, density, and displacement (movement of landmarks). The vector of movement can be measured and the acceleration of the movement extrapolated into the force exerted within the tissue. 3D videography can be used to acquire data in 3 dimensions and to measure and calculate changes after surgery. 3D videographic analysis has been reported in several studies as an accurate (ranging from 0.2 to 1.0 mm) means of recording facial morphology for analysis.
3D videography technology
Capturing a 3D image relies on the principle of stereo photogrammetry, which has been a long-verified technique of triangulation and vector analysis. Two or more cameras are positioned as a stereo pair to identify unique external surface markers in 3D space by calculating the distance between the camera units and their focal distance in relation to the object or marker of interest. Points can be tracked in 3D space, allowing exact stereo triangulation. High-definition cameras are used to maximize data capture and allow for exquisite 3D recreations of facial structure and movement. The precise measurement and tracking abilities enable the researcher to accurately and reproducibly capture and quantify small excursions of movement in the whole face, and to describe both the spatial and temporal features of this movement.
Three-dimensional videography has numerous advantages compared with the commonly used photography analysis technique, the visual analogue scale (VAS). Using an ordinal grading system (eg, 1–10), the facial characteristic that is of research interest (scar, lip symmetry, nostril position) is rated using the VAS. The VAS model is plagued by interobserver inconsistencies and possibility of observer bias. Inherent confounding variables such as the tendency for a rater to avoid scoring the extremes (eg, 1 or 10) also complicate the effectiveness of this method. VAS analysis attempts to take the gestalt observation and convert it into a numerical measurement to allow for statistical analysis. With 3D videography, precise reproducible measurements can eliminate the “human factor” by collecting true, objective data. Such advantages do come with some consequences.
Limitations
The costs of starting a 3D imaging or videography system are likely the most prohibitive factor for more widespread use. The high-definition camera hardware system, exclusive of the 3D computational and rendering software, can cost $50,000. In recent years, high-definition camera systems and high-speed microprocessors capable of handling such large data streams have become more readily available and more economical.
One can currently set up a limited cost-effective system for approximately $10,000. These systems require precise placement and calibration. Minor movements of the camera units require tedious recalibration. The user interfaces of these systems are not as intuitive as other software interfaces and do require dedicated trained personnel. The systems are not portable, and should have dedicated space for maximal accuracy and reliability.
Materials Needed
A typical 3D videography system consists of 3 separate subunits: image capture devices, the computer system, and 3D software. The image capture devices track the defined points in space. A minimum of 2 high-definition video cameras are needed for triangulation. More cameras can be added to increase resolution and raw data. High-definition monochrome high-speed charge-coupled device (CCD) video recorders from Basler (Vision Technologies, Exton, PA, USA) are available from (Graftek Imaging Inc, Austin, TX, USA).
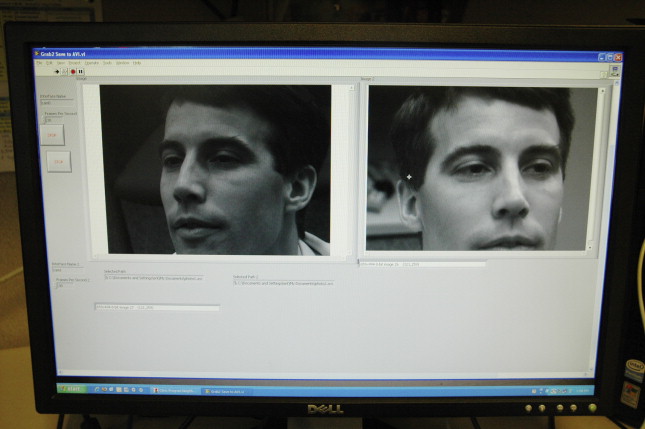
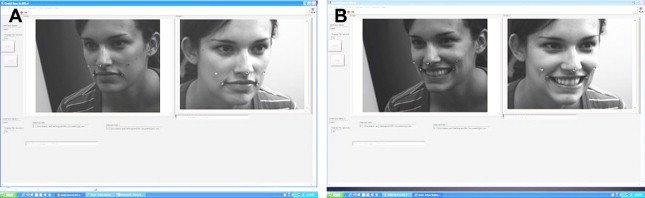
The cameras are placed at different fixed points within a room, and all are convergently focused at a single predefined area ( Fig. 1 ). Each of the CCD video cameras must be calibrated with matching exposure and focal length setting. These cameras are connected via firewire to a computer system. The computer system must have a dedicated video card with memory, separate memory for the main central processing unit, and a large storage device for data. The last component of the system is the 3D tracking and rendering software, such as Simi Motion (zFlo Motion Capture Analysis Inc, Lexington, MA, USA), which allows for data acquisition and analysis. Markers are placed on surface landmarks that are to be tracked. Markers can consist of reflective dots, light-emitting diode (LED) lights or, more simply, inked points from a felt-tip marker. The contrast between the subject’s skin and marker is essential for the tracking system to follow the marker successfully ( Fig. 2 ). Three-dimensional movement of each marker is captured at a rate of 30 frames per second. Landmarks are defined by x, y, and z coordinates to represent a 3D position in space. Throughout the recording subjects initiate repeated movements, which allows for recording of changes in position and acceleration of key landmarks for experimental use.