Loss of volume in the temples is an early sign of aging that is often overlooked by both the physician and the patient. Augmentation of the temple using soft tissue fillers improves the contours of the upper face with the secondary effect of lengthening and lifting the lateral brow. After replacement of volume, treatment of the overlying skin with skin-tightening devices or laser resurfacing help to complete a comprehensive rejuvenation of the temple and upper one-third of the face.
Key points
- •
Loss of volume in the temples is an early sign of aging that is often overlooked by both the physician and the patient.
- •
Augmentation of the temple using soft tissue fillers improves the contours of the upper face with the secondary effect of lengthening and lifting the lateral brow.
- •
After replacement of volume, treatment of the overlying skin with skin tightening devices or laser resurfacing help to complete a comprehensive rejuvenation of the temple and upper one-third of the face.
Introduction
The approval by the Food and Drug Administration (FDA) of the first injectable hyaluronic acid in 2003 (Restylane; Medicis, Scottsdale, AZ) marked the beginning of the modern era of global or pan-facial soft tissue augmentation. Since 2003, the armamentarium of available fillers has expanded exponentially and the emphasis has shifted from a relatively myopic view of filling lines, such as the nasolabial folds, to a more global one that values the face as a complete, cohesive esthetic unit. Esthetic physicians began to appreciate that completely effaced nasolabial folds appear unnatural. Furthermore, a perfectly corrected lower face appears mismatched in the setting of a neglected middle and upper face. This type of esthetic has been termed the “Picasso Face,” in that one area of the face is overexaggerated and stylized compared with a neighboring area of the face that has not been addressed at all. Included in a more global view of facial rejuvenation is increased attention to volume restoration of the upper and lateral face in areas such as the temples. The temples are often neglected by both physicians and patients when planning a strategy for global volume restoration. Temporal rejuvenation, however, has the potential to make a major impact in terms of imparting a more youthful shape to the face.
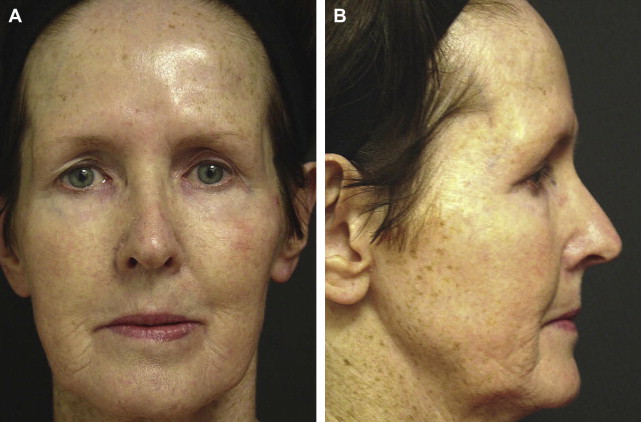
The youthful temple is convex and continuous with the zygomatic arch, such that the outline of the lateral orbital rim is not appreciable and the entire length of the eyebrow is visible from the frontal view. With age, the temporal fossa becomes concave, which emphasizes the bony outline of the lateral orbital rim and pulls the tail of the lateral eyebrow posteriorly, contributing to an overall skeletonized and peanut-shaped appearance of the face ( Fig. 1 ). Hollowing of the temples is a change that often occurs at a relatively young age in thin patients but rarely represents a specific chief concern of a patient seeking cosmetic consultation. Patients more often notice and seek treatment for the fine lines and wrinkles without an appreciation that these are merely a symptom of a larger issue of global volume depletion. Additionally, there are no soft tissue fillers that have FDA approval for use in the temples, which may explain, at least in part, some of the reluctance to treat this area.
The ideal esthetic appearance of a youthful face is not a static image but rather one that changes to reflect the societal values and popular culture of the time. In the mid-1990s, the “heroin chic” esthetic popularized by designer Calvin Klein and super model Kate Moss emphasized features of wasting and cachexia reminiscent of drug addiction. Pale skin, dark under-eye circles, and temporal hollowing were key elements of this esthetic. By the end of the 1990s, the heroin chic era had largely ended after the overdose of fashion photographer Davide Sorrenti and the rise in popularity of Gisele Bundchen and other models with more “healthy” proportions of the face and body. Additionally, with the development of protease inhibitors for the treatment of HIV, facial wasting became socially stigmatizing, leading to FDA approval of both poly-L-lactic acid (PLLA) and calcium hydroxylapatite (CaHA) for the treatment of HIV-associated lipodystrophy. It is still important to obtain an adequate sense of the patient’s esthetic ideals before augmenting any area of the face, as there are patients who prefer a more hollowed out look with prominent facial bones.
Age-related changes in the face affect the overlying epidermis, dermis, subcutaneous fat, muscle, and bone. A comprehensive approach to rejuvenation of the temples must take into account all of these changes. Augmentation with soft tissue filler primarily addresses the age-related changes of the bone, muscle, and fat, whereas laser-resurfacing and skin-tightening devices can address the overlying changes in the dermis and epidermis.
Introduction
The approval by the Food and Drug Administration (FDA) of the first injectable hyaluronic acid in 2003 (Restylane; Medicis, Scottsdale, AZ) marked the beginning of the modern era of global or pan-facial soft tissue augmentation. Since 2003, the armamentarium of available fillers has expanded exponentially and the emphasis has shifted from a relatively myopic view of filling lines, such as the nasolabial folds, to a more global one that values the face as a complete, cohesive esthetic unit. Esthetic physicians began to appreciate that completely effaced nasolabial folds appear unnatural. Furthermore, a perfectly corrected lower face appears mismatched in the setting of a neglected middle and upper face. This type of esthetic has been termed the “Picasso Face,” in that one area of the face is overexaggerated and stylized compared with a neighboring area of the face that has not been addressed at all. Included in a more global view of facial rejuvenation is increased attention to volume restoration of the upper and lateral face in areas such as the temples. The temples are often neglected by both physicians and patients when planning a strategy for global volume restoration. Temporal rejuvenation, however, has the potential to make a major impact in terms of imparting a more youthful shape to the face.
The youthful temple is convex and continuous with the zygomatic arch, such that the outline of the lateral orbital rim is not appreciable and the entire length of the eyebrow is visible from the frontal view. With age, the temporal fossa becomes concave, which emphasizes the bony outline of the lateral orbital rim and pulls the tail of the lateral eyebrow posteriorly, contributing to an overall skeletonized and peanut-shaped appearance of the face ( Fig. 1 ). Hollowing of the temples is a change that often occurs at a relatively young age in thin patients but rarely represents a specific chief concern of a patient seeking cosmetic consultation. Patients more often notice and seek treatment for the fine lines and wrinkles without an appreciation that these are merely a symptom of a larger issue of global volume depletion. Additionally, there are no soft tissue fillers that have FDA approval for use in the temples, which may explain, at least in part, some of the reluctance to treat this area.
The ideal esthetic appearance of a youthful face is not a static image but rather one that changes to reflect the societal values and popular culture of the time. In the mid-1990s, the “heroin chic” esthetic popularized by designer Calvin Klein and super model Kate Moss emphasized features of wasting and cachexia reminiscent of drug addiction. Pale skin, dark under-eye circles, and temporal hollowing were key elements of this esthetic. By the end of the 1990s, the heroin chic era had largely ended after the overdose of fashion photographer Davide Sorrenti and the rise in popularity of Gisele Bundchen and other models with more “healthy” proportions of the face and body. Additionally, with the development of protease inhibitors for the treatment of HIV, facial wasting became socially stigmatizing, leading to FDA approval of both poly-L-lactic acid (PLLA) and calcium hydroxylapatite (CaHA) for the treatment of HIV-associated lipodystrophy. It is still important to obtain an adequate sense of the patient’s esthetic ideals before augmenting any area of the face, as there are patients who prefer a more hollowed out look with prominent facial bones.
Age-related changes in the face affect the overlying epidermis, dermis, subcutaneous fat, muscle, and bone. A comprehensive approach to rejuvenation of the temples must take into account all of these changes. Augmentation with soft tissue filler primarily addresses the age-related changes of the bone, muscle, and fat, whereas laser-resurfacing and skin-tightening devices can address the overlying changes in the dermis and epidermis.
Clinical anatomy of the temporal fossa
Bony Landmarks
One of the reasons why dermal fillers are underused in the temporal fossa may be an unfamiliarity or uncertainty with the underlying anatomy. The term “temples” typically refers to the temporal fossa, which is a shallow depression on the lateral sides of the skull between the forehead and the cheek. The bony landmarks of the temple include the superior temporal line, the frontal process of the zygomatic bone anteriorly, and the zygomatic bone inferiorly. Clinically, the hairline marks the posterior-most aspect of the temple.
Fascial Layers
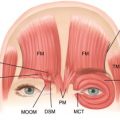
The layers of the temple from superficial to deep include the skin, subcutaneous fat, temporoparietal fascia, deep temporal fascia, temporalis muscle, and temporal bone. The superficial temporal artery and vein course through and are the vascular supply to the temporoparietal fascia, which is immediately deep to subcutaneous fat and is the equivalent of the superficial musculoaponeurotic system (SMAS) below the zygomatic arch. Superiorly, the temporoparietal fascia integrates with the epicranial aponeurosis of the forehead and scalp. The temporal branch of the facial nerve, which innervates the frontalis, corrugator supercilii, procerus, and obicularis oculi, also traverses the temporal fossa, where it lies within the temporoparietal fascia. This is in contrast to areas below the zygomatic arch, where the branches of the facial nerve are deep to the SMAS.
Below the temporoparietal fascia is the deep temporal fascia, which contains the middle temporal artery, a branch of the superficial temporal artery. The deep temporal fascia divides into a superficial and deep layer that envelopes the temporal fat pad approximately 2 to 3 cm above the zygomatic arch. Arising from the deep temporal fascia is the temporalis muscle, which fans out over the surface of the temple ( Fig. 2 ). The temporalis muscle lifts and retracts the mandible.
Evaluation
Age-related changes occur at all levels of the temple from the bone up to the epidermis. Loss of bony substance in the temple, in conjunction with atrophy of the temporalis muscle and wasting of the temporal fat pad, contribute to a gaunt, skeletonized appearance in which the bony outline of the zygomatic arch and the temporal line become more pronounced. These changes become even more prominent in patients who have been previously augmented over the zygoma. Important factors to assess before initiating a strategy for facial rejuvenation include skin elasticity, loss of subcutaneous volume, adherence of the skin to the SMAS, and loss of skeletal support. A complete medical and medication history should be obtained with particular attention to history of autoimmune disease, keloids, current pregnancy, breast feeding, and herpetic infection. Medications known to increase the risk of postprocedure bleeding and bruising include nonsteroidal anti-inflammatories, aspirin, vitamin E, garlic, gingko, ginger, St John’s wort, gingseng, fish oil, and other herbal supplements. If medically reasonable, these medications should be stopped 2 weeks before treatment and the intake of alcohol should be minimized before and after treatment.
History of prior brow lift or facelift can affect the strategy for injection, as the development of scar tissue in the temple can alter the integrity of the fascial planes. It is also important to evaluate the temporal skin, as the presence of overlying rhytides and photodamage can negate or significantly detract from the rejuvenation obtained from soft tissue augmentation. It is important to listen carefully to patients’ preferences; gain an appreciation of their esthetic ideals; and educate them on the risks, benefits, and alternatives of temple rejuvenation.
It is generally advised that the patient be evaluated and marked in an upright sitting position that captures the effects of gravitational forces on the anatomy, contour, and shadowing of the face. Preexisting asymmetry should be documented and discussed thoroughly with the patient. Written informed consent should be obtained, and off-label use of the products disclosed. Preprocedure and postprocedure photography is a key component to managing patient expectations. In the case of temporal augmentation, it is particularly important to take pictures from several angles other than the frontal view to fully demonstrate the improvement in the contour. It has been suggested that oblique views with standardized lighting are best, while recognizing that the subtle 3-dimensional changes can often only be fully appreciated in person.
Patient perspective
Although most patients do not specifically recognize or request temporal augmentation, it likely contributes to their overall sense of appearing older. Common chief complaints of patients with temporal wasting include “looking tired” or an impression that the “face is falling.” Although the ideal facial shape differs among cultures, a heart-shaped contour that is widest at the temples and narrowest at the chin is often a cosmetically desirable result and can be obtained via augmentation of the temples. Before injection of the temples with filler, local anesthetic or saline can be injected to give the patient a preview of the expected result. Loss of volume in the temples also contributes to the appearance of brow ptosis, as the lateral tail of the eyebrow descends into the hollowness of the temple. Augmenting the temples has the additional effect of bringing the tail of the brow anteriorly, which makes it appear longer and higher when the patient is viewed from the front. Augmentation of the temples should be one part of a global strategy for improving the volume loss of the upper and middle face.
When selecting a filler for temporal augmentation, patients should be thoroughly counseled regarding the differences between hyaluronic acid (HA) fillers and biostimulatory injectables, such as CaHA and PLLA. Particularly with PLLA, patients should understand that the effect is gradual and requires a series of injections. With regard to skin-tightening procedures, the results using nonablative laser or energy devices are subtle compared with those obtained from surgical lifting, but have considerably less downtime. It is crucial that patients have appropriate expectations and understand that these medical interventions are an alternative, not a substitute, for plastic surgery.
Procedure
Temporal Augmentation with Soft Tissue Fillers
Augmentation of the temples can be achieved using autologous fat or fillers, such as HA, CaHA, PLLA, or silicone. Currently, none of the fillers have an FDA indication for augmentation of the temples, and thus patients must be informed that this is an off-label use. The temple, however, serves as an ideal area of the face for an FDA indication, because it is a discrete anatomic location with well-defined borders. The bony landmarks of the temple form a discrete indentation similar to a pool or lake and thus the degree of filling or hollowing can easily be appreciated based on how close the “water” is to being level with the surrounding ground. We propose a scale of temporal hollowing, graded from 0 through 4, with 0 representing a completely contiguous and smooth transition between the zygoma and the lateral temporal line and 4 representing severe atrophy with prominence of the zygoma and bones of the lateral orbit.
Factors to consider when selecting a filler for the temporal region include the onset of the effect, the texture of the product, the longevity of the result, and the safety profile. HA fillers result in an immediate augmentation, have a soft and natural appearance under the skin, and last for approximately 12 months. They are generally considered to be safe, with few serious adverse reactions reported in the literature and no immunogenicity. Additionally, one key advantage of HA fillers is that they are easily reversible with hyaluronidase in the event of vascular occlusion or patient dissatisfaction. PLLA (Sculptra Aesthetic; Sanofi-Aventis, Bridgewater, NJ) is also commonly used for temporal augmentation and provides a gradual volumizing effect over several months. Advantages of PLLA include a natural, soft look that incorporates the endogenous collagen. Disadvantages include cost and the need for several treatments. CaHA (Radiesse, Merz Aesthetics, San Mateo, CA), like Sculptra, is considered a biostimulatory filler with effects that develop gradually over time, but also has an immediately appreciable effect on volume at the time of injection.
Planes of Injection for Augmentation
The appropriate plane of injection depends on the product utilized. When using the semipermanent fillers, such a CaHA and PLLA, the plane of injection is deep, immediately over the periosteum. A deep plane of injection minimizes the chance of inadvertent intravascular injection or injury to the nerves and vasculature as they run significantly more superficial through the temporal fossa. HA fillers may be injected deep or more superficially in the subcutaneous plane with blunt-tip microcannulas. Deeper injections of HA fillers typically require more product than superficial.
Hyaluronic Acid
There are currently no controlled clinical studies that evaluate the safety or efficacy of any of the dermal fillers for temporal augmentation. In a retrospective review of 20 female patients, Moradi and colleagues described their technique for temporal augmentation using Restylane. Patients were prepped and treated with topical anesthetic ointment for 15 minutes. A 30-gauge needle was inserted perpendicular to the skin through the dermis, at which point the angle was adjusted to 45° such that the plane of injection of the filler was immediately above the superficial temporal fascia. Approximately 0.05 to 0.10 mL of filler was injected at each site using an anterograde, retrograde, or depot injection technique with an average total volume of 0.95 mL needed to fill each temporal fossa. All patients self-reported satisfaction with the augmentation, which was sustained for at least 6 months in all cases. There were no adverse events reported other than mild tenderness and bruising.
Ross and Malhotra also reported their experience with temporal augmentation in a series of 20 patients using Perlane (Medicis). After the patient was prepped and anesthetized, a 27-gauge needle was inserted, bevel down, in the plane of the superficial temporal fascia. At each of the 3 injection sites, 0.5 mL of product was placed along the anterior temple and then massaged to prevent contour irregularities. Patients received a mean of 0.9 mL of filler per temple, with a reported duration of effect of approximately 1 year. Complications included postprocedure prominence of the superficial vein, bruising, and discomfort with chewing.
Poly-L-lactic Acid
PLLA (Sculptra Aesthetic; Sanofi-Aventis) is a biodegradable alpha-hydroxy acid material consisting of PLLA microparticles, sodium carboxymethylcellulose, and mannitol that has been used for other medical applications, such as absorbable sutures, for many years. FDA approved in 2004 for the treatment of HIV-associated lipodystrophy, it was also granted FDA approval in July 2009 for cosmetic indications, including correction of nasolabial fold defects and other facial wrinkles. As with the other soft tissue fillers, use in the temporal region is off-label. PLLA is considered a biostimulatory product that promotes the deposition of collagen over time by stimulating an inflammatory tissue response. In contrast to HA fillers, the effects of PLLA are more gradual in onset and require 2 to 8 injections every 4 to 6 weeks over the course of several months depending on the degree of volume deficit. PLLA lasts longer than HA fillers with a duration of action of up to 2 years.
The biostimulatory effect of PLLA is dependent on the host response; thus, only patients with intact immune systems are good candidates for PLLA injections. The main advantages of PLLA include its biostimulatory method of action and the increased duration of up to 2 years. One of the disadvantages of PLLA is that the correction is gradual and dependent on the robustness of the host response, thus making it difficult for the injector to gauge the appropriate end point for correction at the time of injection. Because of a certain degree of unpredictability with PLLA, great caution must be taken to avoid overcorrection. Another potential deterrent to the use of PLLA is the cost and the need for repeat treatments over the course of several months. Although the price of injections varies based on geography and the practitioner, the cost to the patient per vial of PLLA is approximately $900.
Although the package insert recommends reconstitution with only 5 mL of sterile water 2 hours before treatment, most practitioners use a dilution of at least 8 mL with varying combinations of sterile or bacteriostatic saline and 1% or 2% lidocaine. The use of epinephrine depends on the preferences of the injector. Some believe that it improves hemostasis while others believe that the vasoconstrictive effect can mask evidence of impending vascular compromise. After reconstitution, the vial is gently swirled with care to avoid rigorous shaking that can lead to formation of foam that can obstruct the needle. Patient preparation includes cleansing the face with soap and water and application of topical anesthetic. It is worth noting that some practitioners do not use topical anesthesia, believing that the proper plane of injection for PLLA is far deeper than can be penetrated by topical medications. A 3-mL syringe with a 25-G or 26-G needle can be used. PLLA is injected in the supraperiosteal plane, deep to the temporalis fascia, using a depot technique with boluses of 0.3 to 3.0 mL, followed by firm massage.
Calcium Hydroxylapatite
CaHA (Radiesse, Merz Aesthetics) is considered a “combined filler,” with both gradual biostimulatory properties and immediate space-filling effects. The composition of CaHA is 30% CaHA small-particle (25–45 μm) microspheres suspended in 70% aqueous gel composed of 6.4% glycerin and 1.3% sodium carboxymethylcellulose. Because the calcium microspheres are the same as the components of human bone and teeth, CaHA is biocompatible and does not require sensitivity testing before use. The immediate filling effect is a result of the aqueous carrier, which is eventually absorbed over time, leaving behind the calcium microspheres to serve as a scaffold for the growth of new tissue stimulated by the local fibrohistiocytic response. Eventually, at approximately 9 months, the microspheres are also absorbed and eliminated from the body as calcium and phosphate ions through the kidneys. The duration of volume correction after CaHA is reported to be 10 to 14 months, with shorter duration in areas with high mobility and frequent muscle movement, such as the nasolabial fold. A “booster” injection 3 months after the initial treatment may prolong the effect for as long as 15 to 18 months. Radiesse gained FDA approval in 2006 for the correction of moderate to severe facial wrinkles and folds and for correction of HIV-associated lipoatrophy. The use of CaHA for temporal augmentation is considered an off-label use.
Like PLLA, the plane of injection for CaHA in the temples is immediately superior the periosteum. Because the plane of injection is deep, pain control is an important consideration, as this affects both the patient’s perception of the outcome and his or her desire to return for additional treatment. Compared with HA fillers, injection of CaHA is associated with more discomfort regardless of the plane of injection. In 2009, the FDA officially approved the injection technique of adding lidocaine to the CaHA syringe immediately before injection, which dramatically improved pain control and reduced the need for regional nerve blocks. In this technique, 0.15 to 0.20 mL of 2% plain lidocaine is drawn up in a 3-mL syringe and attached to the 1.3-mL or 1.5-mL syringe of Radiesse using the female-to-female luer lock connector provided separately in the Merz Aesthetics Accessory Kit. The 2 syringes are pushed back and forth, pushing the Radiesse into the lidocaine first, until a smooth mixture is obtained. It should be noted, however, that the addition of lidocaine at a concentration of 0.3% will decrease the viscosity and elasticity of Radiesse to the level of medium-viscosity and elasticity HA fillers such as Restylane and Perlane. This in turn reduces the degree of lifting that can be obtained with a given volume.
CaHA is injected with a 27-gauge, 1.25-inch or 28-gauge, 0.75-inch needle using a variety of injection techniques, including retrograde, linear, fanning, or cross-hatching. For temporal augmentation, many injectors prefer a bolus depot technique followed by firm massage to prevent nodules. CaHA can safely be combined with laser or light therapies such as intense pulsed light (IPL) or nonablative fractional resurfacing to address overlying photodamage. Studies have also shown that CaHA is not altered after radiofrequency heating; thus, combination with skin-tightening procedures is also safe. Similarly, other products, such as HA fillers, can be layered with CaHA to address the more superficial lines that remain after the volume deficit has been addressed. One advantage of CaHA in the temples is that, because of its high viscosity and elasticity relative to HA fillers, a smaller volume is generally required to produce the same degree of correction. Because the temple can sometimes require larger volumes for adequate correction, the semipermanent fillers have the potential to be more cost effective for the patient. A large-particle CaHA has FDA approval for the treatment of urinary incontinence, and there are preliminary data in 3 case reports suggesting that it is safe when injected in the middle face and may have longer-lasting clinical effects relative to the small-particle Radiesse. The larger-size particles, however, necessitated the use of a larger-bore needle (21 gauge) and regional nerve blocks for adequate anesthesia.
Authors’ Technique for Temporal Augmentation
For temporal augmentation, the authors have found the semipermanent biostimulatory fillers PLLA (Sculptra) and CaHA (Radiesse) to produce the best results and to be the most time and cost effective for the patient. PLLA is reconstituted at least 24 hours before the procedure with 8 mL of bacteriostatic water. Immediately before injection, 1 mL of 2% lidocaine with epinephrine is added to the vial. Once reconstituted, PLLA should be refrigerated and can be stored for up to 3 to 4 weeks. Using a 3-mL syringe with a 25-gauge, 1.0-inch or 1.5-inch needle, the plane of injection is deep, just above the periosteum with aspiration before injection ( Fig. 3 ). A depot bolus technique is used, starting at the front of the hairline and proceeding anteriorly to the medial aspect of the eyebrow, which provides a secondary effect of lifting the tail of the brow. Typically, 2 to 4 injection points are needed for adequate augmentation. Keeping the injecting thumb off the plunger until the needle is in the plane of injection helps to prevent inadvertent deposition of product in the muscle, and brisk injections in succession will avoid clogging of the needle. At the initial visit, 1 to 2 vials are used with no more than 2 vials used in a single visit. Subsequent visits are timed 1 month apart for 1 to 2 visits and then every 6 to 8 weeks for additional visits. Ice packs are applied immediately postprocedure and patients are instructed to massage the area 3 to 5 times per day for 5 minutes for 5 days. Postprocedure complications are minimal with some patients complaining of a mild soreness in the jawline. When using Radiesse, the injection technique is the same, using approximately 0.3 to 0.5 mL of product per side with molding and massage to avoid overcorrection and nodule formation.