Traditional upper blepharoplasty typically involves resection of excess upper eyelid skin and muscle with or without fat excision. Well-established concepts in periorbital aging have been challenged by newer morphologic and histologic studies that have characterized the changes that occur in the various periorbital soft tissue components. Several modified or adjunctive techniques have recently emerged to improve esthetic outcomes in upper blepharoplasty. The authors review surgical technique in detail: nasal fat repositioning, orbicularis oculi preservation, increasing lateral upper eyelid fullness, lacrimal gland resuspension, internal brow elevation, and glabellar myectomy, along with complications and aftercare involved with procedures.
Key points
- •
Similar to recent trends in lower blepharoplasty toward volume conservation and repositioning, improved understanding of upper periorbital aging has allowed surgeons to develop new or modified techniques to improve esthetic outcomes in upper blepharoplasty.
- •
Repositioning the more robust nasal fat compartment laterally toward the central preaponeurotic fat can improve medial redundancy without compromising central upper eyelid volume.
- •
With little to no morphologic or functional change in orbicularis oculi with aging, muscle preservation during upper blepharoplasty may prevent unnecessary complications or scarring in selected patients with dermatochalasis as the primary concern.
- •
Volume loss in the lateral third of the upper eyelid can be restored with pedicled fat flaps or free fat grafts in conjunction with orbicularis oculi imbrication.
- •
The upper blepharoplasty incision allows direct access to the brow and orbital structures that may aggravate upper eyelid crowding and fullness. Internal brow elevation and sculpting and resuspension of a prolapsed lacrimal gland can be performed through the upper blepharoplasty incision.
Introduction
Upper blepharoplasty is one of the most frequent facial cosmetic surgical procedures for periorbital rejuvenation. The natural esthetic and youthful appearance of the periorbital region is characterized by soft tissue fullness framing the eye, whereas the aging eye is typically hollowed and surrounded by a deep upper lid sulcus with variable amounts of upper lid skin laxity with or without pseudoherniation of periorbital fat. When considering upper eyelid rejuvenation, it is imperative to consider all factors that may contribute to the aging upper eyelids. Standard treatments for upper lid dermatochalasis have focused on resection of redundant tissue, including skin, muscle, and fat from the upper eyelid. This may lead to hollowing of the upper lid sulcus from overresection of soft tissue, resulting in an unfavorable appearance.
In recent years, the concept of periorbital volume restoration and augmentation, instead of reduction, has gained increasing popularity among cosmetic surgeons. Improved understanding of periorbital physiology from aging has led to modified techniques using fat conservation and repositioning, orbicularis oculi muscle preservation, and increasing lateral upper eyelid fullness to achieve esthetic enhancements in upper blepharoplasty. These concepts in conjunction with adjunctive procedures, including internal brow elevation, lacrimal gland resuspension, and glabellar myectomy performed through an upper blepharoplasty approach, can provide a myriad of esthetic enhancements to standard upper blepharoplasty.
Anatomy
The upper eyelid crease is located approximately 8 to 10 mm from the palpebral margin in the typical Caucasian eye. Loss of fascial attachments of the orbicularis oculi, levator aponeurosis, and orbital septum into the dermis can contribute to skin laxity and displacement of the crease inferiorly. In the brow, the frontalis muscle interdigitates with the procerus muscle medially, orbicularis oculi muscle laterally, and corrugator and orbicularis oculi muscles in the central portion of the brow. The galeal layer that gives rise to the fascia overlying these muscles contributes to brow height, symmetry, and shape.
Upper Eyelid Fat
The upper eyelid fat is divided into nasal (medial) and preaponeurotic (central) fat pads divided by the superior oblique muscle tendon and is found posterior to the orbital septum. The nasal fat pad is usually pale yellow or white, whereas the lateral fat pad is more yellow. This difference is suggested to be caused by a greater amount of connective tissue and vascularity in the nasal fat and a greater amount of carotenoids in the lateral fat. The retro-orbicularis oculi fat (ROOF) lies deep to the orbicularis oculi muscle but above and anterior to the orbital septum and should not be confused with the preaponeurotic fat pad, which lies deep to the orbital septum. The ROOF is contiguous superiorly with the lateral brow fat pad, which lies beneath the orbicularis oculi and frontalis muscular layer. The ROOF is more fibrofatty than the preaponeurotic eyelid fat and provides fullness to the temporal eyelid and brow, which can persist after upper blepharoplasty if left unaddressed. The lateral brow fat should be distinguished from a prolapsed lacrimal gland, which can present with excessive lateral upper eyelid fullness caused mainly by relaxation of suspensory ligaments. The gland is firmer in texture than the surrounding fat and is tan.
Orbicularis Oculi Muscle
Traditional upper blepharoplasty often includes an en bloc excision of skin and orbicularis oculi muscle. The palpebral portion of the muscle is limited to the eyelid and is divided into pretarsal and preseptal components. The functions of this muscle are primarily for eyelid closure, compression of tears, and dilation of the lacrimal sac. Although the skin and subcutaneous tissue layer undergo significant changes with aging, the orbicularis oculi muscle remains anatomically and physiologically intact and is not affected by advancing age, as described in a recent study by Pottier and colleagues. Their histologic study showed that orbicularis oculi muscle fibers remained intact with the same bulk of fibers through the aging process. However, the loss of skin elastic fibers and skin laxity were significant and paralleled the advancement of age. Additionally, electromyographic analysis showed that age did not have a significant effect on motor unit action potentials and the force of muscle contraction. A similar histologic study by Lee and colleagues showed that the orbicularis oculi muscle remained morphologically intact with advancing age in the Asian population. The authors concluded that a minimally invasive approach with muscle sparing in upper blepharoplasty in selected patients who desire volume preservation of the youthful convexity of the upper eyelid–brow junction could yield positive esthetic results and retain excellent eyelid function while minimizing postoperative complications.
Upper Eyelid Aging
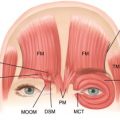
Recent studies on anatomic, chemical, and biologic characteristics of the upper eyelid have shown that the central fat pad seems to diminish in volume with aging, whereas the nasal fat pad increases in volume with advancing age ( Figs. 1 and 2 ). This disparity seems to begin in the early fourth decade of age, with the most significant change after age 70 years. This disparity may be explained by differences in vascularity and connective tissue composition. The nasal fat pad is similar in composition to intraconal orbital fat, whereas the more yellow central fat pad is similar to adipose tissue found elsewhere throughout the body. Korn and colleagues reported that there was a 2-fold increase in the number of adult stem cells derived from human orbital adipose tissue in the nasal fat pad compared with the central fat pad. The authors suggest that the relative abundance in progenitor stem cells in the nasal fat may explain the relative increase in nasal fat pad volume during an individual’s lifetime.
Evaluation
When determining a surgical treatment plan for a patient who presents with excess periorbital tissue and heaviness in the upper eyelids, it is important to consider all of the factors that may contribute to the redundancy of the upper eyelids. The surgeon must evaluate the patient’s individual periocular features, both in the present and in his or her past youthful state. The gradual loss of skin elasticity, with or without pseudoherniation of periorbital fat, is primarily responsible for the aging look of the upper eyelid. Dermatochalasis in the older population can impair peripheral vision as a result of an excessive fold of upper eyelid skin. Preoperative ophthalmologic consultation is recommended for documentation of visual field impairment in this patient population.
It is also important to consider less common etiologies for upper eyelid redundancy when evaluating a patient for upper blepharoplasty. Excessive bulging in the lateral third of the upper eyelid may be caused by a prolapsed lacrimal gland, which can be identified preoperatively with manual compression over the globe, which may show a slightly movable defined mass in the lacrimal fossa. A prolapsed gland can be observed in approximately 10% of patients at the time of surgery. Unintentional resection of the lacrimal gland as a result of erroneously mistaking the gland for periorbital fat can lead to disruption of lacrimal secretory function. Another condition that can present with upper eyelid heaviness is blepharochalasis, a recurrent inflammatory condition resulting in intermittent edema and erythema of the upper eyelid skin because of an increased histamine and immunoglobulin E response. Unlike dermatochalasis, blepharochalasis is often difficult to correct.
A complete evaluation of the upper eyelid includes an assessment of the brow shape and its position relative to the eye. Upper blepharoplasty performed alone in the presence of significant brow ptosis can result in further lowering of brow position. It may also lead to excessive skin excision, which can overly narrow the space between the palpebral margin and the brow. Additionally, this may introduce the heavier thick brow skin into the upper eyelid, potentially worsening brow ptosis and lid function. Medial brow ptosis may be associated with deep glabellar rhytids, particularly as a result of the strong depressor action of the corrugator and depressor supercilii muscles.
A thorough medical and ophthalmologic history must be obtained from the patient, including a history of diabetes, hypertension, cardiac disease, thyroid disease, bleeding disorders, problems with dry eyes or excessive tearing, and prior periorbital or ocular surgery. Old photographs of patients in their youth are particularly helpful in determining the approach to upper eyelid rejuvenation. These photographs enable the surgeon to evaluate eyelid crease height, palpebral fissure size, periorbital asymmetries, brow position, and brow shape in the patient’s youthful state. All of these factors must be considered before selecting the surgical plan that best suits the patient’s needs.
Related posts:
 Advances in Esthetic Surgery from Four Specialties
Brow and Upper Lid Aesthetics and Rejuvenation: Views from Four Disciplines
Advances in Esthetic Surgery from Four Specialties
Brow and Upper Lid Aesthetics and Rejuvenation: Views from Four Disciplines
 Contemporary Concepts in Brow and Eyelid Aging
Technical Considerations in Endoscopic Brow Lift
Adjunctive Fat Grafting to the Upper Lid and Brow
Asian Upper Lid Blepharoplasty Surgery
Contemporary Concepts in Brow and Eyelid Aging
Technical Considerations in Endoscopic Brow Lift
Adjunctive Fat Grafting to the Upper Lid and Brow
Asian Upper Lid Blepharoplasty Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


