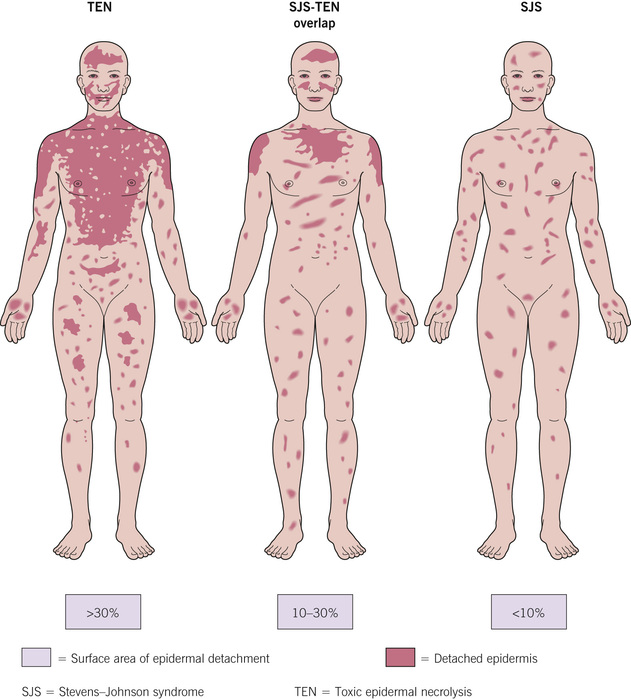
The extent of epidermal injury can be important (Fig. 8.2), and this chapter organizes diseases in that vein (extensive, extensive or limited, and often limited).
Fig. 8.2Spectrum of disease based upon surface area of epidermal detachment.Adapted from Bastuji-Garin S, Rzany B, Stern RS, et al. Clinical classification of cases of toxic epidermal necrolysis, Stevens-Johnson syndrome, and erythema multiforme. Arch Dermatol. 1993;129:92–6. From Bolognia JL, Schaffer JV, Duncan KO, Ko CJ. Dermatology Essentials, 1e. Philadelphia: Saunders, 2014, with permission.
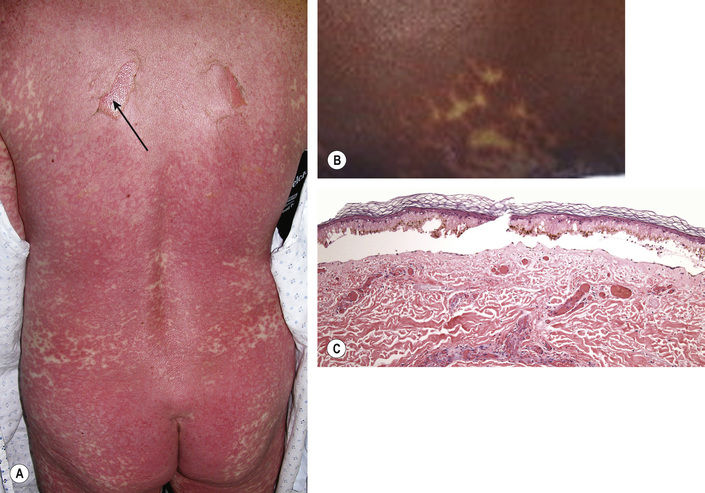
Bullae and erosions (arrow) over the skin (Fig. 8.3)
Fig. 8.3Toxic epidermal necrolysis. A Sloughing of skin. B Macular atypical targets. C Epidermal necrosis with subepidermal cleft.A, B, Courtesy, Yale Dermatology Residents’ Slide Collection. B, From Bolognia JL, Schaffer JV, Duncan KO, Ko CJ. Dermatology Essentials, 1e. Philadelphia: Saunders, 2014, with permission.
Histopathology:
Normal stratum corneum above epidermal necrosis, often with detachment of the epidermis from the dermis
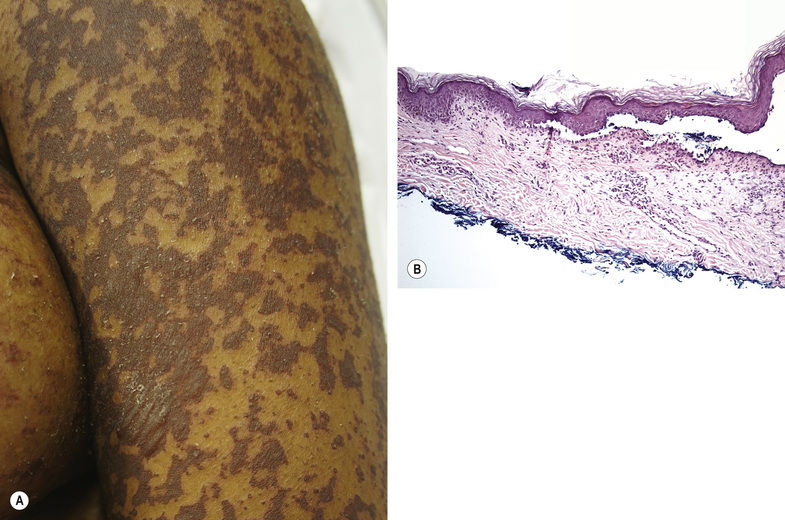
Stevens–Johnson Syndrome
Covers <10% of the body surface area (seeFig. 8.2)
Similar lesions to toxic epidermal necrolysis, clinically and histologically (Fig. 8.4)
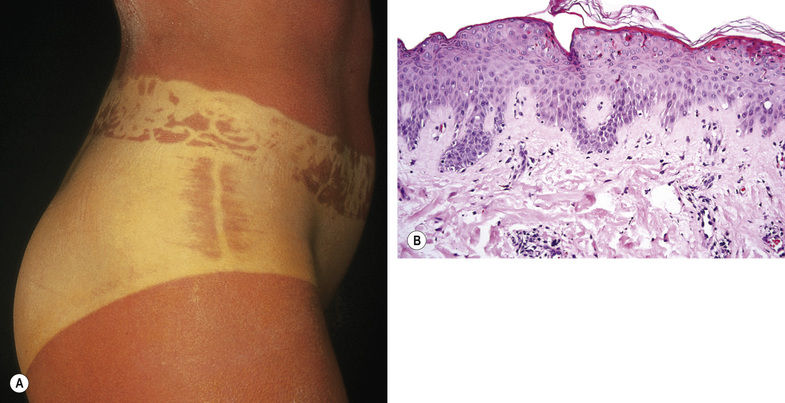
Fig. 8.5Sunburn. A Twenty-four hours after an accidental 10-fold overdose of UVB prescribed as phototherapy. B Scattered necrotic keratinocytes in the epidermis.With permission, Department of Dermatology, University of Würzburg, Germany. A, From Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology, 3e. London: Saunders, 2012, with permission. B, From Brinster NK, Liu V, McKee PH, Diwan H. Dermatopathology: High Yield Pathology. Philadelphia: Saunders, 2011.
Later stages – sloughing of skin
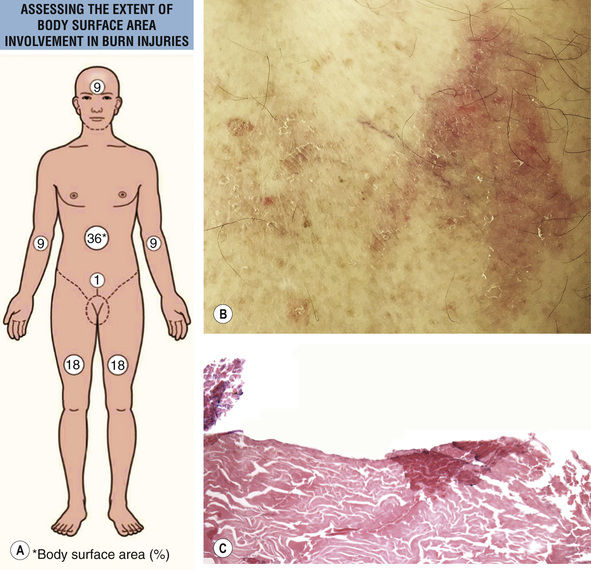
Thermal Burn
Body surface area affected can be estimated using a “rule of nines” (Fig. 8.6A)
Fig. 8.6Thermal burn. A Assessing the extent of body surface area involvement: rule of nines. B Erythema, erosion, and scale secondary to a burn from spilling hot tea. C The epidermis is completely absent in this burn.A, Courtesy, Karynne O Duncan, MD. A, From Bolognia JL, Schaffer JV, Duncan KO, Ko CJ. Dermatology Essentials, 1e. Philadelphia: Saunders, 2014, with permission.
Acute erythema; in more severe cases, sloughing, erosion, and/or ulceration (Fig. 8.6B–D)
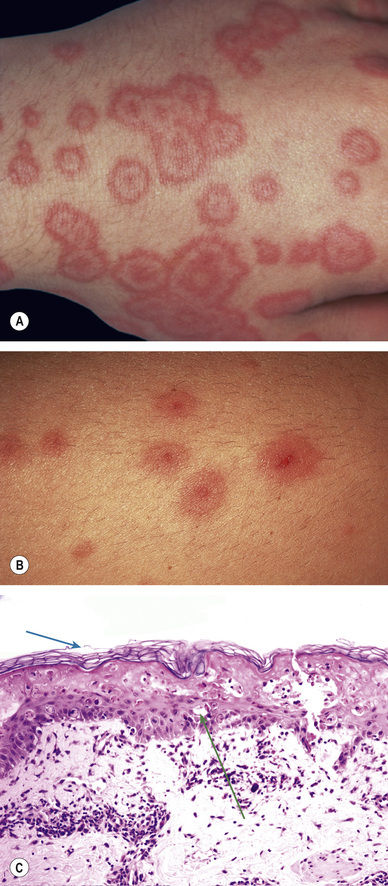
Erythema Multiforme
Favors acral sites
Classic lesion – target with central deep red erythema surrounded by a halo of lighter color and an outer red rim (Fig. 8.7A)
Fig. 8.7Erythema multiforme. A Classic lesion. B Papular atypical targets. C Apoptotic keratinocytes.A,B, Courtesy, Yale Dermatology Residents’ Slide Collection. A,B, From Bolognia JL, Schaffer JV, Duncan KO, Ko CJ. Dermatology Essentials, 1e. Philadelphia: Saunders, 2014, with permission.