Melanoma remains one of the most deadly of skin cancers and its incidence has been rising steadily throughout the past several decades. The risk factors associated with melanoma include external factors, such as exposure to ultraviolet radiation, and host factors, such as family history, history of dysplastic nevi, and number of nevi. The 2002 American Joint Committee on Cancer tumor-nodes-metastasis staging classification incorporates Breslow depth, Clark’s level, ulceration, pathologic microstaging attributes, and nodal and distant metastases. Prognosis remains poor for advanced disease and surgery remains the mainstay of treatment for early stage melanoma.
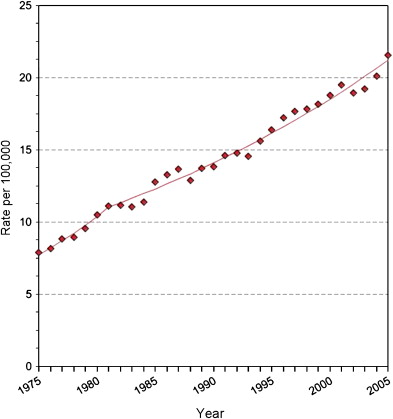
The incidence of malignant melanoma is rising steadily and rapidly in the United States. Melanoma is now the sixth and seventh most common new cancer among men and women respectively. An estimated 62,480 new cases of cutaneous melanoma will be diagnosed in 2008, a 13% increase compared with 2004 (55,100 new diagnoses). In addition, there will be an estimated 54,020 new cases of melanoma in situ in 2008. From 1975 to 2005, data from the National Cancer Institute Surveillance Epidemiology and End Results (SEER) show that the incidence of melanoma nearly tripled ( Fig. 1 ). One in 55 men and women in the United States will be diagnosed with cutaneous melanoma.
Prevalence is also increasing. In 2005, 723,416 men and women alive in the United States had a history of melanoma of the skin—349,414 men and 374,002 women.
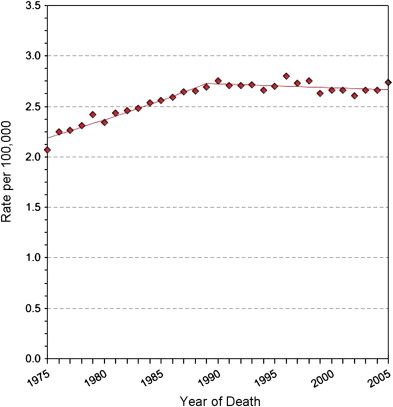
The mortality rate for melanoma increased by about 20% from the 1970s to 1990, but has largely stabilized from the 1990s onwards ( Fig. 2 ). In 2008, an estimated 8,420 people will die from melanoma compared with 7,910 in 2004. Currently, one person in the United States dies from melanoma every hour.
Incidence and mortality by age, sex, and race
Based on the SEER data for 2001 to 2005, the median age at diagnosis for melanoma of the skin was 59 and the median age at death was 68. Additional breakdown in incidence and mortality by age group is shown in Table 1 .
| Age | Incidence(%) | Deaths(%) |
|---|---|---|
| <20 | 0.9 | 0.1 |
| 20–34 | 8.1 | 2.9 |
| 35–44 | 12.9 | 7.2 |
| 45–54 | 18.9 | 15.0 |
| 55–64 | 19.5 | 18.8 |
| 65–74 | 17.8% | 21.3 |
| 75–84 | 16.4 | 23.6 |
| >85 | 5.5 | 11.0 |
The age-adjusted incidence and death rates for melanoma were 19.4 and 2.7 per 100,000 per year respectively between the years 2001 and 2005. This data is further divided by sex and race in Table 2 . Melanoma is several times more common in whites compared with more deeply pigmented ethnic groups. Men are approximately 1.5 times more likely to develop melanoma than are women, and more than twice as many men die of melanoma compared with women (see Table 2 ). In men, the most common area for melanoma development is the back. In women, melanoma most commonly arises on the arms and legs.
| Race or Ethnicity | Incidence Rates by Race | Death Rates by Race | ||
|---|---|---|---|---|
| Male (per 100,000) | Female (per 100,000) | Male (per 100,000) | Female (per 100,000) | |
| All races | 24.6 | 15.6 | 3.9 | 1.7 |
| White | 28.5 | 18.5 | 4.4 | 2.0 |
| Black | 1.1 | 0.9 | 0.5 | 0.4 |
| Asian or Pacific Islander | 1.6 | 1.3 | 0.5 | 0.3 |
| American Indian or Alaska Native | 3.9 | 2.6 | 1.5 | 0.7 |
| Hispanic | 4.8 | 4.9 | 0.9 | 0.6 |
Risk factors
Risk factors can be divided into environmental factors and host factors. The main environmental risk is ultraviolet radiation (UVR). The increasing incidence of melanoma may be partially due to the depletion of the ozone layer, which allows more UVR to penetrate the atmosphere. In addition, many people use tanning beds, which emit high amounts of UVR.
A history of sunburns confers twice the risk of developing melanoma compared with no prior history of sunburns Those with a childhood history of sunburns are at an even higher risk. Patients with a history of more than 10 severe painful sunburns increase their risk for developing melanoma in the upper extremity by up to 6.8-fold; 2.4-fold in the head or neck; 2.1-fold in the lower extremity; and 1.7-fold in the trunk, shoulder, hip, back, or abdomen. Tanning bed exposure may lead to a higher risk of melanoma with one meta-analysis showing a 1.25 odds ratio (CI 95%) in patients with prior exposure compared with those with no prior exposure. Interestingly, the use of sunscreen as a UVR-protective device has not been shown to reduce the risk of melanoma. This may be explained by the results of several studies that show that those using sunscreen are more likely to spend more time in the sun and hence increase their total UVR exposure.
Certain phenotypic characteristics such as red hair, skin type, sun sensitivity, and freckles are associated with an increased risk of developing melanoma. Skin type is determined by the quantity and type of melanin. Melanin, produced by the melanocyte, is the skin’s natural protectant against ultraviolet damage. Melanin absorbs UVR and possesses potent antioxidant properties that can neutralize free radicals produced by the radiation. There are two types of melanin produced in the skin: eumelanin and pheomelanin. The ratio of eumelanin to pheomelanin is controlled by the melanocortin 1 receptor, which, when functioning well, leads to an increased amount of eumelanin production. Eumelanin is responsible for gray, black, yellow, and brown colors found in hair and skin and confers greater UVR protection. Pheomelanin produces more pink and red colors and is the primary form of melanin in people with red hair. People with red hair have diminished melanocortin 1 receptor function—an independent risk factor for developing melanoma.
Family history and the presence of melanocytic nevi are also strong risk factors for melanoma. Patients with a first-degree relative with melanoma have a twofold higher risk of developing melanoma compared with patients with no family history of melanoma. The risk of developing melanoma increases with the number of moles. Having more than ten moles greater than three millimeters on the arm can increase the risk of melanoma development by up to 4.7-fold on the trunk, shoulder, hip, back, or abdomen; 3.5-fold on the head or neck; 2.5-fold on the upper extremity; and 2-fold on the lower extremity. Sunscreen (sun protection factor 30) usage has been shown to decrease the number of acquired nevi that develop in children.
Evidence suggests that the presence of dysplastic nevi confer an independent risk factor for melanoma. A recent meta-analysis concluded that subjects with five or more dysplastic nevi had six times the risk of developing melanoma compared with subjects with no atypical nevi.
The Spitz nevus sometimes causes diagnostic confusion with melanoma. Most Spitz nevi are found in children. However, there are spitzoid melanomas, and these are usually found in adults, that share microscopic features of Spitz nevi, but are malignant, with the potential to metastasize. Lyon provides detailed discussion in this issue.
Larger nevi are associated with a greater risk of melanoma. In particular, giant congenital melanocytic nevi (>20 cm) have a substantial risk of malignant transformation. The estimated lifetime of risk of melanoma in these patients has been reported to be between 5% and 40%. Their melanomas tend to occur within the first 3 to 5 years of life (50% of occurrences by 3 years of life, 60% by childhood, 70% by puberty).
Women with a history of breast cancer may have a slightly higher chance of developing melanoma (standardized incidence ratio = 1.41, CI 0.91–2.09). This has fueled speculation that hormonal factors can influence the development of melanoma. Interestingly, a pooled-analysis study showed a reduced risk (odds ratio 0.33) of melanoma among women with higher parity (>5) with an early age at first birth (<20 years) compared with women with a later age at first birth (>25 years) and lower parity.
The overall risk of melanoma increases when multiple risk factors including family history, increased number of nevi, history of severe sunburn, freckling on the upper back, light hair color are present. Having one or two risk factors can increase the risk of melanoma by two- to fourfold, and more than three risk factors can increase the risk by more than twentyfold.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


