A significant subgroup of patients that present to esthetic eye and facial plastic practices are interested in more comprehensive facial rejuvenation than can be achieved with 4 eyelid blepharoplasty alone. Many of these patients are not interested in the larger incisions, extended recuperation and the expense associated with traditional facelift techniques. The endoscopic preperiosteal midfacelift restores a youthful heart shape to the face, is a valuable tool in periorbital rejuvenation, and has a demonstrated track record of safety and longevity. In this review, we describe patient selection and our surgical technique and discuss postoperative care and the management of complications.
Key points
- •
Small incision preperiosteal midface lifting is a useful procedure that addresses the cheek, helps elevate the lid cheek junction, and recreates a youthful heart-shaped face.
- •
With the appropriate equipment and a learning curve facilitated by knowledge of midfacial anatomy, the procedure uses the incisions used for brow lift and extends the dissection to the level of the nasolabial fold.
- •
The procedure has proven longevity with a low complication rate.
- •
Preperiosteal midfacelifting can be useful to address midfacial aging, postblepharoplasty cicatricial ectropion, and midmalar festoons.
- •
The procedure is an excellent adjunct to blepharoplasty, regenerative fat grafting, and laser resurfacing in appropriately selected patients.
Video content accompanies this article at http://www.advancesincosmeticsurgery.com .
Introduction
In an oculoplastic practice, patients frequently request periorbital rejuvenation. They are not interested in a facelift or a necklift with the attendant risks, large incisions, prolonged recovery, activity limitations, and the temporary facial distortion associated with the procedure. They nonetheless note drooping of the cheeks and brows and understand that these esthetic issues contribute to the appearance of their eyes.
Comprehensive periorbital rejuvenation involves not only addressing the skin excess and the steatoblepharon but also involves addressing the brows, the tear trough, and the midface. Multiple approaches and technical variations exist for addressing all these issues. No evidence-based consensus exists for best techniques for brow lifting, addressing the tear trough, or repositioning the midface.
This article describes the preperiosteal approach to the midface that has been developed and refined in our practices during the past 2 decades. Other approaches to the midface, such as the transeyelid approach, may be effective but can be frought with the potential for complications. Although deep plane facelifting is said to also be a technique to address the midface, one of the original surgeons who innovated the composite lift later retracted his contention that the midface was elevated with the deep plane technique [ ]. The transtemporal preperiosteal midface lift is a powerful means of achieving long-lasting cheek rejuvenation. We describe that rationale for this procedure, the history of endoscopic midface lifting and why this technique may be the optimum in terms of risk and reward, with a low complication rate, a high satisfaction rate, and a proven record of longevity.
Rationale
Current trends have the majority of midface volume deficiencies addressed in an office setting using fillers by providers with varying degrees of training and skill and varied qualifications. These fillers may be hyaluronic acid (Juvederm Voluma, Restylane Contour, Restylane Lyft, Defyne, RHA 3 or RHA4) or calcium hydroxyapatite (CaHa) based (Radiesse). The soft tissue fillers are described to have cohesive and rheologic properties that “lift.” Authors have attempted to quantify the lifting effect of fillers [ ]. According to the American Society of Plastic Surgery, more than 5,700,000 of these procedures were performed in 2022, demonstrating their popularity for achieving esthetic benefit. (∗ ASAPS statistics, 2022, plastic-surgery-statistics-report-2022.pdf, page 9.)
Preliminary initial work done in our centers being prepared for publication, however, demonstrates that HA fillers provide expansion in the z-axis and x-axis but produce little to no elevation and, in some cases, actually cause drift in a negative direction along the y-axis (Wulc, Foster unpublished data, 2023).
Clinically, this translates into patients that come into our offices with volume expansion (sometimes, exaggerated volume expansion) from previous exuberant filler injection. In addition to creating a distorted version of the patient’s youthful face, other attendant problems include festooning potentially from gel-related interference with lymphatic drainage and color distortion from internal reflection of filler at the lid cheek junction.
We do not think that volume loss alone accounts for changes in the midface—gravity is also responsible. Eliminating the effects of gravity—or rather changing its vector of force—by changing posture from the upright to the supine position allows the sagging volumes of the midface to reposition and eliminate many of the morphologic changes associated with aging—lying flat produces effacement of the tear trough and elevation of the cheek as the volumes of the face return to a more youthful position. Similarly, the brow elevates [ , ].
Multiple approaches to counter the effects of gravity have been described that lift the cheek through an eyelid incision, a lateral canthal incision, at the temporal hairline, above it, or in front of the ear [ ]. The lift can be accompanied by an intraoral incision to release the periosteum and retaining ligaments at their origins. Thread lifts have been described but are ineffective in creating any long-term lift [ , ].
Subperiosteal approaches to the midface have been described that are safe. Some involve an intraoral incision while others are performed transtemporally or through the lower eyelids [ ].These procedures are not anatomic—while they produce a desired elevation of the cheeks and efface the lid cheek junction, they do not address ligamentous laxity or volume changes within the fat compartments. Additionally, the transeyelid subperiosteal approach has been associated with complications including ectropion in up to 19% of cases [ , ]. These procedures with slight variation continue to be practiced by our colleagues, some of whom have published excellent results [ ].
The preperiosteal approach to the midface performed with a temporal incision is a more forgiving and, potentially, a more anatomic approach. The deep and superficial compartments can be visualized and augmented when necessary with autologous fat. The ligamentous structures are visualized, assessed, and can be supported with cable sutures under little to no tension without resorting to complete disruption.
Complete ligamentous excision as a means of creating a successful result has been emphasized by Mendelson and others [ , ]. Whether it is the tear trough ligament or the zygomatic and masseteric ligaments, we have not found complete transection necessary to achieve a natural and long-lasting result. We have found and witnessed in the work of others that complete ligamentous disruption allows the midface and the face to be moved as a unit but sometimes in a distorted direction that affects not only the position of the face at rest but more importantly alters facial expression unnaturally during animation.
If one likens the ligaments that suspend the face to the structural support of a bridge, the problem of the aging face becomes similar to the problem of a sagging bridge. When a bridge shows signs of its age and begins to lose support, the engineer reinforces areas of weakness. The engineer does not recommend razing all the supporting pylons of the bridge, which weakens the entire structure and necessitates a much more disruptive rebuild.
Although the majority of facial surgeons advocate for and support the complete severance of facial ligaments, there are no studies that corroborate the longevity benefit of these procedures. There are several studies from our group that suggest that there is no esthetic benefit to cutting the orbital retaining ligament (ORL) or the zygomatic ligament and there is a longevity benefit seen with a ligament-sparing approach [ , ].
History
Endoscopic surgery emerged as an adjunct to esthetic surgery in the early 90s and was practiced in Europe and South America and was adopted by surgeons shortly thereafter in the United States. Fodor was one of the first to recognize the importance of this technique, adopted and modified from earlier developments in endoscopic orthopedic, and laparoscopic general surgical and gynecologic procedures [ ]. The smaller incisions, increased magnification and illumination achieved with endoscopes allowed for smaller incisions, less scarring, decreased operative times, less disruption to vascular, lymphatic and neural tissues, and potentially shorter healing times. These advantages were rapidly incorporated in breast augmentation surgery via transumbilical and transaxillary approaches.
In 1994, Isse described the endoscopic foreheadplasty [ ]. His study recognized that weakening of the protractors of the brows alone in conjunction with suspension of the frontalis could produce significant esthetic brow elevation. Fifty-seven cases were presented; in 7 of the cases, the dissection extended into the midface. To our knowledge, this was the first modern description of the technique.
As interest in this technique increased, in 1997, Isse described endoscopic facial surgery in detail, including patient selection, anatomic considerations, and both the subperiosteal and preperiosteal techniques [ ]. Isse used a subperiosteal approach in thin older patients with severe nasolabial folds and recognized that the wide undermining caused extensive and prolonged swelling. He noted that direct suspension with this technique did not produce elevation because of the massive amount of tissue that was displaced. He used the preperiosteal approach in patients with more moderate soft tissue ptosis. This was the first contemporary discussion of the technique that we describe herein. Isse detached the zygomatic ligaments from the bony arch, elevating what he termed the superficial musculoaponeurotic system (SMAS) of the midface above the zygomaticus muscles to the deep temporalis fascia using a single 3 to 0 nylon suture. The results of this technique in the midface were excellent [ ]. Subsequent publications refined his technique [ ].
Subperiosteal endoscopic midface techniques have been described by Anderson and Lo, Williams, and Ramirez, and others [ , , ]. Ramirez in his discussion of his personal evolution of midface elevation initially had success splitting the lateral fibers of the orbicularis in the preperiosteal plane and suspending the suborbicularis oculi fat pad (SOOF), but scarring was a problem so he reverted to subperiosteal intraoral release with suspensions of the Bichat fat pad [ ].
Contemporary descriptions of the preperiosteal procedure are sparse with the exception of the publications by Bernardini, Kao and Duscher, and the authors [ ]. Kao and Duscher published their results in an exclusively Asian population. In older Asian patients, they combined preperiosteal midface lift with a posterior neck lift to avoid preauricular scarring [ ].
Anatomy pertinent to endoscopic preperiosteal midfacelifting
A familiarity with the anatomy of the temporalis fossa and the midface is a prerequisite to performing the procedure. Detailed descriptions of the surface topography and the surgical anatomy associated with the facial upper two-thirds are beyond the scope of this article but are well described elsewhere [ ].
Important Points
- •
Beyond the inferior temporal ligament, the temporoparietal fascia no longer is present and the branches of the temporal portion of the facial nerve are no longer protected: the surgeon must remain directly on the deep fascia.
- •
The correct plane at the level of the temporal branch is identified by a network of veins and nerves that penetrate the temporalis fascia vertically extending into the more superficial planes. These include the medial and lateral sentinel veins (so called because they are sentinels for the facial nerve that is in the roof of the space being traversed) and the medial and lateral zygomaticotemporal nerves.
- •
Ligaments that anchor the face exist along the breadth of the zygomatic arch. We have found that it is neither necessary nor helpful to interrupt these ligaments beyond the malar body. Extending the dissection too laterally—that is, beyond 4 cm from the lateral canthal angle—can result in prolonged orbicularis weakness and potentially injure the temporal branch of the facial nerve.
- •
The lateral canthal thickening (LCT), described by Mendelson is visualized routinely medial and caudad to the medial sentinel vein and represents a safe potential gateway into the midface. The LCT is contiguous with the lateral aspect of the ORL.
- •
The ORL represents the most superior aspect of the transtemporal midfacelift dissection and is not disrupted with this technique. The ligament extends from the orbital rim through the junction of preseptal and orbital orbicularis to skin.
- •
The orbicularis muscle, responsible for eyelid closure, extends at least 2.5 cm from the lateral orbital rim and represents the roof of the midface dissection [ ]. The suborbicularis oculi fat pad is in the floor of the dissection.
- •
The lateral-most extent of the dissection disrupts the most medial aspect of the zygomatic ligament, which overlies the zygomatic major and minor muscles.
- •
As dissection continues more medially to the nasolabial fold, the zygomatic major and minor muscles are often visualized on the floor.
- •
The innervation to the orbicularis muscle enters the midface from laterally below the zygomaticus major muscle in most cases and thus, when the muscle is identified, is protected in a plane below the plane of dissection.
- •
The zygomaticofacial artery and nerve can be visualized along the malar body in a proportion of patients. The infraorbital nerve bundle is not seen in this dissection.
- •
In the midface, superficial fat is seen in the undersurface of the subcutaneous skin and is marbleized and adherent to skin. The amount of this fat increases as the nasolabial fold is approached. These fat compartments have been elegantly described by Rorhich and Pessa [ ].
- •
The deep lateral SOOF is targeted for direct elevation with sutures along with the lateral orbital orbicularis oculi [ ].
- •
The buccal fat pad is not visualized with this dissection.
The aging midface
Facial aging is the result of dynamic changes that occur in all layers of the face. Skin changes, bone changes, volume changes, and gravitational shifts all are involved, and our understanding of the individual contributions of each of these components to the midfacial aging process continues to evolve.
The skin thins and loses elasticity, and collagen becomes less organized and the retinacula cutis thins, lengthens and dehiscences from the underlying subcutaneous collagenous network. Skin texture changes and dyschromias and actinic changes occur along with both dynamic and static rhytids.
Muscular thinning may also play a role but may not contribute as significantly as other factors [ ].
The bony maxilla may retrude creating a steeper midfacial angle contributing to apparent midface descent [ ].
Fat compartments lose volume and/or redistribute their volume [ ]. The volume of lower lid fat seems to increase [ ]. Additionally, the orbital septum elongates, and fat, perhaps in similar volume, seems to protrude through the attenuated septum. The deep compartment of the midface also accumulate volume with aging, particularly in the caudal aspects of the midface [ ]. The deep compartments deflate disproportionately, and the superficial compartments shift inferiorly as a consequence. [ ].
Gravity plays a dynamic role in the topographic changes that occur in the aging midface. Several studies show that in the supine position the midface recovers a more youthful redistribution of volumes [ , ]. The ligaments, particularly the ORL and the zygomaticocutaneous ligament lengthen in the upright position, allowing the skin and fat they support to sag, worsening the hollow deserted by midfacial fat at the ORL and deepening the depth of the nasolabial fold.
In youth, a smooth transition exists between the lower eyelid and the cheek and the well-described “heart shape” of youth is seen. With aging, the downward drift of the midfacial tissues creates the convexity- concavity convexity deformity, wherein the orbital fat protrudes above the tear trough hollow while the bulging midfacial tissues protrude beneath. With time, the midface sags and the face becomes more pear-shaped.
Evaluation of the Brow, Midface, and Periorbital Area
An esthetic assessment of the patient requesting periocular rejuvenation and upper or lower blepharoplasty involves a detailed history and assessment of eyelid position, amount of skin excess and steatoblepharon in the upper and lower eyelids, the condition of the skin, function of the muscles and vector of the eye with respect to surrounding structures (positive or negative vector assessment), the integrity of the medial and lateral canthal tendons, the position of the lacrimal glands, and condition of the skin.
Assessment involves the lower eyelid snapback test, and the lower lid distraction test, as well as measurements of orbital position with an exophthalmometer for vectoral assessment. Slit lamp evaluation when possible should be performed assessing for signs of dry eye including tear meniscus, tear film breakup time, corneal staining, and other signs of dry eye.
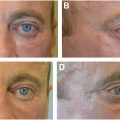
Comprehensive evaluation of the periorbital area involves a comparison with old photographs from varying times—usually each decade—so that the surgeon can determine the individual aspects of each patient’s aging process, which vary from patient to patient: from fat accumulation to fat loss, and to differential changes in the position of the brows that occur over time. In many patients, the brow elevates as a compensatory adjustment for the development of upper lid skin excess or aponeurotic attenuation and the development of ptosis. Frontalis use that results because of this causes shifts in brow contour. A useful maneuver to determine the contribution of the eyelids to brow position involves the instillation of a drop of 2.5% neosynephrine into the ptotic eye or eyes [ ]. If the brow relaxes, this is an indication that the brow may actually become ptotic following upper eyelid surgery. The patient should participate in the decision as to whether the brow should be repositioned at the time of surgery ( Fig. 1 ).
Midface position is assessed and compared with old photographs. In most photographs that patients bring in to the consult, they are smiling and thus comparison of smiling pictures is most useful with the patient smiling in the consultation. Some authors have described the increased facial muscular tensioning that occurs as we age [ ]. We have found that with chronologic age, as the midface becomes more ptotic, smiling requires more effort, produces less incisural show (regardless of upper lip length) and produces a more profound deepening of the nasolabial fold than was present in youth. It is easy to demonstrate this age-related difference in the smile to the patient during the consultation.
As a matter of routine, we shift the patient from upright into the supine position showing them their midface position in the mirror and demonstrating the change in smile that also occurs. In general, changing the gravitational vectors and allowing the facial volumes to move superiorly in the supine position illustrates to the patient the potential for midfacial elevation with the attendant volume restoration that occurs due to the shift.
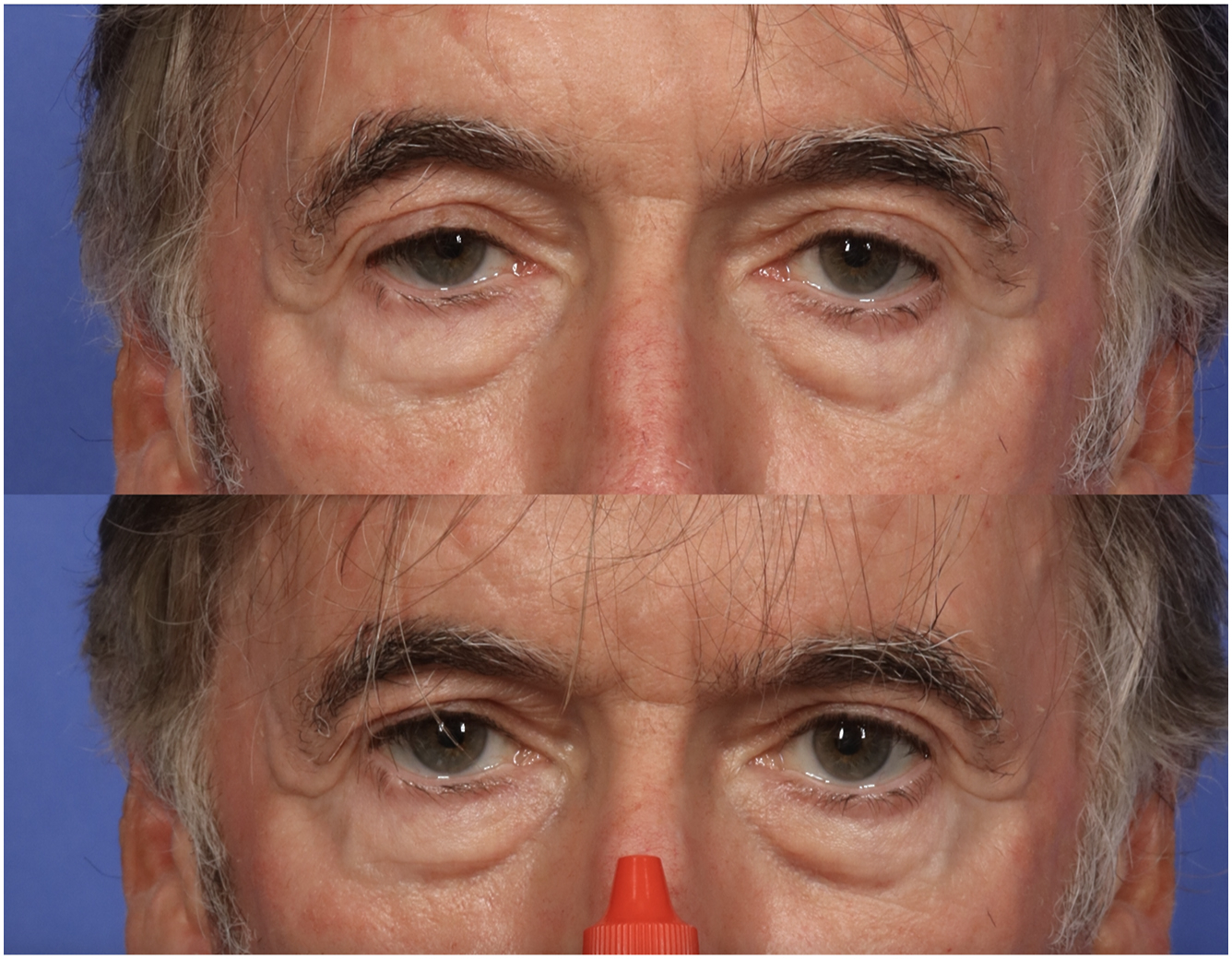
We have previously described an ideal position of the midface based only on the assessment of female models based on Shutterstock two-dimensional images and found that midface position can be assessed and compared with this ideal by measuring the width of the interzygomatic distance (width of the interzygomatic distance of the midface [WIZDOM]) [ ]. This distance is reproducibly measured among examiners. The position of the WIZDOM seems to fall with aging and, in the presence of volume loss, also diminishes in width. We therefore have developed a means of assessing the relationship between the eyes and the midface by measuring the distance between a vertical line dropped by the lateral canthus and the horizontal WIZDOM measurement. In youth, this distance measures 12 to 18 mm, and over time, the distance from lateral canthus (LC) to WIZDOM can enlarge to 20 to 35 mm ( Fig. 2 ). As the midface descends, the lower lid length seems to lengthen [ ].
Our examination documents:
- •
Diminution in the lateral expansion and projection of the midface.
- •
An increase in the WIZDOM lateral canthal distance (also seen with overfilling)
- •
The position of the lid cheek junction
- •
The presence or absence of malar festoons
- •
Baring of the inferior or lateral orbital rim
- •
Depth of the nasolabial fold
We have found that the preperiosteal approach with our described technique does not improve the depth of the nasolabial fold but addresses these other aspects of the midfacial aging process. A recently published study on the deep plane lift confirms that this may be because the deeper tissues on which suspension relies are exceedingly elastic regardless of midface approach used: the deep plane lift also does not ameliorate the nasolabial folds [ ].
Comprehensive facial analysis also involves the general assessment of facial proportions, asymmetries, quality of skin, amount of jowling and changes at the cervicomental angle, lesions, facial nerve function, previous scars, platysma cording, subplatysmal and preplatysmal fat, salivary glandular prominence and thyroid prominence, position of the hyoid, and so forth. In most patients, one cheek is lower and flatter than the other. One explanation for this may be extrapolated from Anson, Kane, and Lambros who postulated that positioning during sleep not only created a distinct pattern of facial wrinkles but also created differential areas of expansion and compression [ ].
Equipment for the procedure
The procedure we describe involves simultaneous upper and lower blepharoplasty, liposculpture, laser resurfacing, and endoscopic surgery.
- •
Blepharoplasty tray
- •
Endoscopic facial plastic surgical tray
- •
A 4-mm endoscope with midface sheath (Hayden Medical, Santa Clarita, CA)
- •
Endoscopic viewing camera and tower (Karl Storz, Karl Storz, Tuttlingen, Germany)
- •
Trepsat or Viterbo elevators (Hayden Medical, Santa Clarita, CA)
- •
Tonsil forceps
- •
Long needle holder or other suture passer device
- •
Liposculpture equipment
- ○
Cannula for liposuction—(Tonnard cannula, Tulip Aesthetics, San Diego, CA)
- ○
- •
Processing device (any one of the below has been used in our cases)
- ○
Hogue prism particle sizer (Hayden Medical, Santa Clarita, CA)
- ○
Lipocube™, (London, UK)
- ○
Tulip Nanofat Set™ (Tulip® Aesthetics, San Diego, CA)
- ○
- •
Injection cannulas SoftFil® –18 g and 23 g cannulas (Prollenium®, Richmond Hill, Ontario, Canada)
Surgical technique
Endoscopic midface lifting is generally only a part of periorbital rejuvenation that, when indicated, is usually accompanied by sculptural lower blepharoplasty, endoscopic forehead lift and brow reshaping, upper blepharoplasty, regenerative fat grafting, and dual erbium laser resurfacing. Surgery can be performed under intravenous sedation or with general anesthesia.
If an upper blepharoplasty is indicated in the planned periorbital rejuvenation, the general order of surgery begins with the following:
- •
Marking
- •
Infiltration of local anesthetic
- •
Infiltration of tumescent local anesthetic
- •
Upper blepharoplasty without upper eyelid skin closure
- •
Fat harvest
- •
Liposculpture (fat is infiltrated into the lower lid at the tear trough before lower blepharoplasty to prevent egress of fat through the tranconjunctival incision.
- •
Lower transconjunctival blepharoplasty
- •
Endoscopic brow lift
- •
Endoscopic midface lift
- •
Closure of upper eyelid skin after conservative removal
- •
Lower lid skin pinch or laser resurfacing
In the preoperative holding area, the areas of volume loss and volume excesses are marked in the upright position because landmarks change or disappear in the supine position.
The patient is brought to the operating room. Tetracaine drops are instilled.
The upper eyelid creases are marked with the patient awake, by opening and closing the eyes and verifying that the incisions lie symmetrically in the natural upper eyelid creases. The forehead is marked centrally immediately posterior to the hairline with an intended incision of approximately 1.2 cm. Approximately 4.5 cm laterally in each direction, 2 intended paramedian incisions of the same length are marked. Temporal incisions are outlined 1.5 cm from the superior temporal crest ligament approximately 1.5 cm from the temporal tufts bilaterally and these incisions span 2 to 2.5 cm in length.
Other markings that are helpful include (1) Pitanguy’s line, which extends from 0.5 cm below the inferior border of the tragus to 1.5 cm above the lateral brow, marking the course of the temporal branch of the facial nerve, (2) the location of the upper and lower borders of the bony zygomatic arch and the malar body, and (3) the approximate location of the zygomaticus major and minor muscles ( Fig. 3 ).