Key points
- •
Brow aesthetics and surgical options for brow lift and forehead rejuvenation.
- •
Ideal candidates for the endoscopic browlift technique.
- •
Forehead and periocular anatomy.
- •
Surgical technique and the four key steps for endoscopic brow rejuvenation.
- •
Long-term results and complications.
Patient selection
Since the introduction of the endoscopic approach in 1993 by Luis Vasconez, I have not performed an open coronal brow lift. Almost all of my facial rejuvenation cases today include brow rejuvenation through an endoscopic technique. The best candidates for endoscopic forehead lifts are patients with flat foreheads (flat frontal bone), no receding hairlines (low hairline) and no redundant forehead skin. High hairlines and male pattern baldness can add the challenge of being able to see and remove the glabellar muscles.
Other techniques for forehead rejuvenation include open coronal, lateral temporal brow lift, direct approach through the brow, transpalpebral brow lift with direct excision of the corrugator muscles and Botox injections. During patient selection, the two key problems to be addressed are eyebrow ptosis and frontal and glabellar frown lines.
Indications
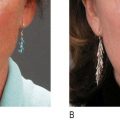
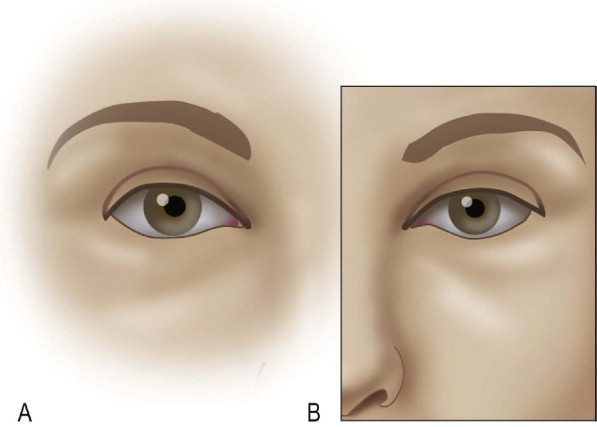
The ideal shape and position of the brow has been changing over the years and through different cultures. Therefore, the brow aesthetics cannot be generalized and must be evaluated in relation to gender, ethnicity, orbital shape and overall facial aging and proportions. Currently, we consider the ‘ideal aesthetic brow’ when the medial brow should be at or below the level of the orbital rim, the medial brow should be above the medial canthus, should have a gentle peak on the last two-thirds towards the lateral end with the lateral tail higher than the medial ( Figure 10.1 ). With facial aging, the eyebrows gradually fall and loose volume encroaching on the orbit and bunching the skin over the lateral orbital rim creating what is known as ‘temporal hooding’. Eyebrow ptosis, eyebrow asymmetry, temporal hooding and forehead wrinkles are all indications for forehead rejuvenation and a brow lift ( Figure 10.2 ).
Anatomy
The anatomy of the forehead and periorbital regions should be appreciated by the surgeon. The temporal ridge is bound by the temporal line of fusion which is a deep bony point of fixation of the overlying soft tissue. In order to adequately release and mobilize the lateral brow and temporal region, the temporal line of fusion should be released to the level of the supraorbital rim. There are also supraorbital ligamentous attachments that require release in order to elevate the brow and forehead ( Figure 10.3 ).
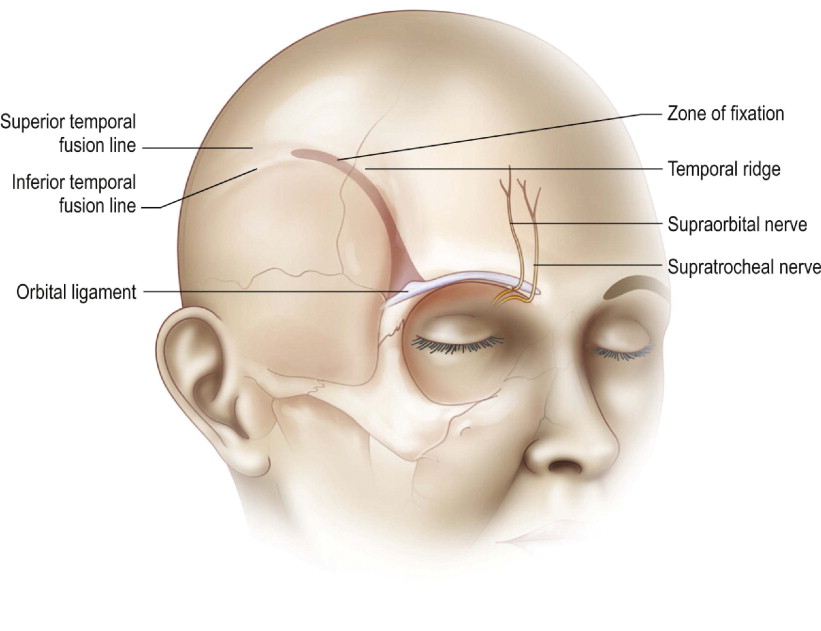
The nerves which are encountered and preserved during endoscopic browlift include the two main sensory nerves, the supratroclear and supraorbital nerves, and the main motor branch of the facial nerve, the frontal nerve. Care is taken to appreciate and preserve these nerves during dissection. Subgaleal dissection lateral to the temporal line of fusion will maintain the plane of dissection deep to the frontal branch. Inferior dissection to the level of the sentinel vein while remaining superficial to the superficial layer of the deep temporal fascia also protects the frontal branch from direct division or traction neuropraxia. Appreciation that the neurovascular bundles for the supratrochlear and supraorbital nerves exit the orbit 1.5 and 2.5 cm from midline respectively allows gentle division of the periosteum at that location to avoid division of the nerves ( Figure 10.4 ).
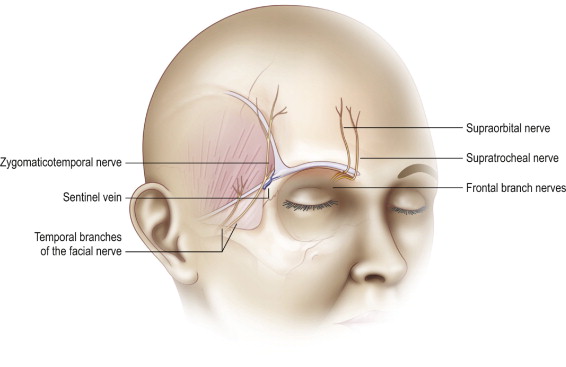
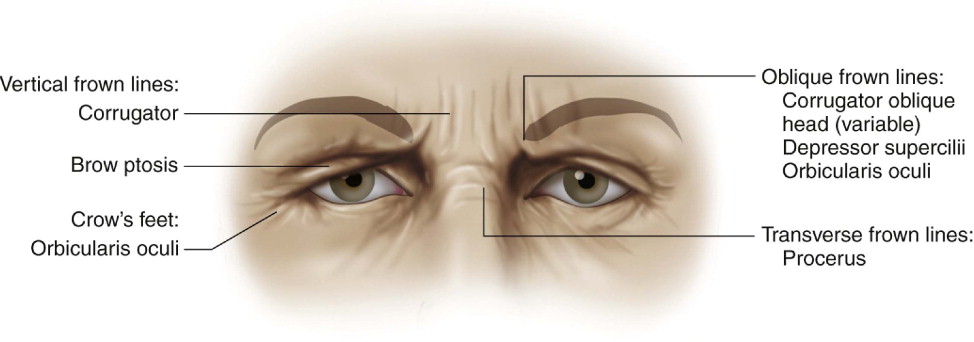
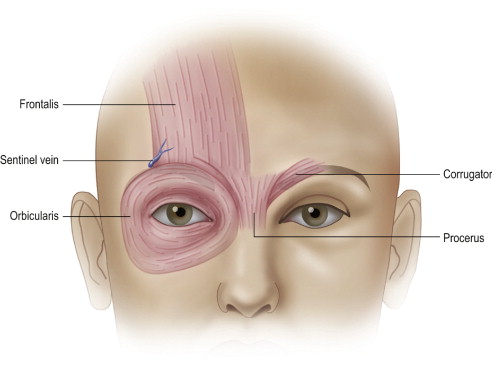
The sentinel vein is inferior to the inferior temporal septum and approximates the level of the frontal branch for the facial nerve. The muscles of the forehead include the frontalis, procerus, corrugator supercilii with oblique and transverse heads, the depressor supercilii, and the orbicularis muscles. The brow elevator includes the frontalis while the other muscles act as varying degrees of brow depressor. While release and physical repositioning of the brow and forehead elevate the brow, division and weakening of the brow depressors also correct dynamic brow ptosis and glabellar frown lines ( Figure 10.5 ).
Operative technique
Pre-operative preparation
After adequate informed consent, the patient is marked for surgery in a standing position. A temporal incision is marked along a superior lateral vector line from the nasal ala crossing the lateral canthus and continues to a point approximately 2 cm behind the temporal hairline. A 2 cm curved line is then marked medial to that point in both temporal areas. Paramedian incisions are marked by a straight line from the mid-pupil superiorly to the anterior frontal hairline. A one centimeter vertical line posterior to the hairline is marked in those areas for the paramedian incisions ( Figure 10.6 ).