div class=”ChapterContextInformation”>
10. Telogen Effluvium
Keywords
Telogen effluviumHair lossHair sheddingHair pullPsychological impactNutritionMinoxidilEducationReassuranceIntroduction
Telogen effluvium is one of the most common causes of hair loss; however, it has heterogeneous triggers. The exact number of cases is difficult to assess as many are subclinical and do not result in office visits [1]. It is important to understand that if the triggering factor is not identified, the therapy will be symptomatic instead of resolutive. Telogen effluvium has two subtypes: acute and chronic.
It appears to be more common in women, but this propensity may be due to men underreporting the disease [2]. Acute telogen effluvium results from acute transition of follicles from anagen to telogen phase [1], and it can be secondary to both internal and external insults. The effects of age on acute telogen effluvium are not entirely clear but some studies have shown evidence that elderly woman are more susceptible [2], whereas it is uncommon in children [3, 4]. Chronic telogen effluvium has a strong predilection for women aged 30–60 [5]. It does not appear to have any racial predilection.
Etiology
Proposed mechanisms of telogen effluvium
Mechanism | Notes |
|---|---|
Premature anagen phase interruption | Most common type Hair shedding 2–3 months after initiation of the causative factor, due the transition from anagen through catagen and telogen with a subsequent release of telogen hairs For example, physiologic stress, fever, drugs, scalp inflammation, weight loss, smoking, and major surgeries |
Excessive prolongation of the anagen phase | Hair follicles remain in prolonged anagen phase rather than cycling into telogen. When finally released from anagen phase, telogen effluvium is manifested For example, post-partum telogen effluvium and telogen effluvium occurring after the interruption of topical minoxidil or oral contraceptives |
Reduced anagen phase duration | Mechanism behind telogen effluvium sometimes occurring alongside androgenetic alopecia, hypothyroidism, iron deficiency, and senescent alopecia |
Delayed teloptosis | Hair follicles remain in prolonged telogen phase rather than being shed and recycled into anagen phase For example, scalp psoriasis |
Premature teloptosis | Seen with drugs that promote anagen re-entry or proteolysis and rupture of cadherins Mechanism behind telogen effluvium occurring after the initiation of topical minoxidil [7] Keratolytics and retinoids are also implicated |
Causes of telogen effluvium
Physiologic | Postpartum |
Shedding of the newborn | |
Seasonal shedding | |
Illness associated | Postfebrile and infections (i.e., typhoid, malaria, TB, syphilis) |
Chronic illness (i.e., HIV) | |
Stress | Serious injuries |
Major surgery | |
Hemorrhage | |
Starvation or rapid weight loss | |
Significant psychological stress | |
Strenuous physical exercise | |
Nutritional | Malnutrition [9] |
Crash diets [10] | |
Iron deficiency anemia | |
Acquired zinc deficiency | |
Acrodermatitis enteropathica | |
Drugs | Oral retinoids |
Antithyroid drugs | |
Anticonvulsants | |
Hypolipidemic drugs | |
Heavy metals [11] | |
Beta blockers | |
Captopril [12] | |
Amphetamines [12] | |
Anticoagulants [12] | |
Discontinuation of oral contraceptives [13] | |
Interferon-α-2b [13] | |
Endocrine | Hyperthyroidism |
Hypothyroidism | |
Organ dysfunction | Renal failure |
Hepatic failure | |
Local cause | Hair transplant [14] |
Contact dermatitis (i.e., hair dye application) [15] | |
Local surgery [16] | |
Inflammatory conditions of the scalp (i.e., psoriasis, seborrheic dermatitis) | |
Infectious conditions of the scalp (i.e., fungal, bacterial, viral) | |
Other | Dermatomyositis [17] |
Systemic lupus erythematosus | |
Syphilis | |
Idiopathic | |
Anti-cellulite creams containing iodine or thyroid extracts | |
Over-the-counter drugs to lose weight | |
Traveling from low to high daylight locations (changing time zone) | |
Keratolytic shampoos | |
Herbal remedies |
Clinical Features

Bag with hair shed by patient in 1 year

Brush demonstrating hair shedding by patient with telogen effluvium
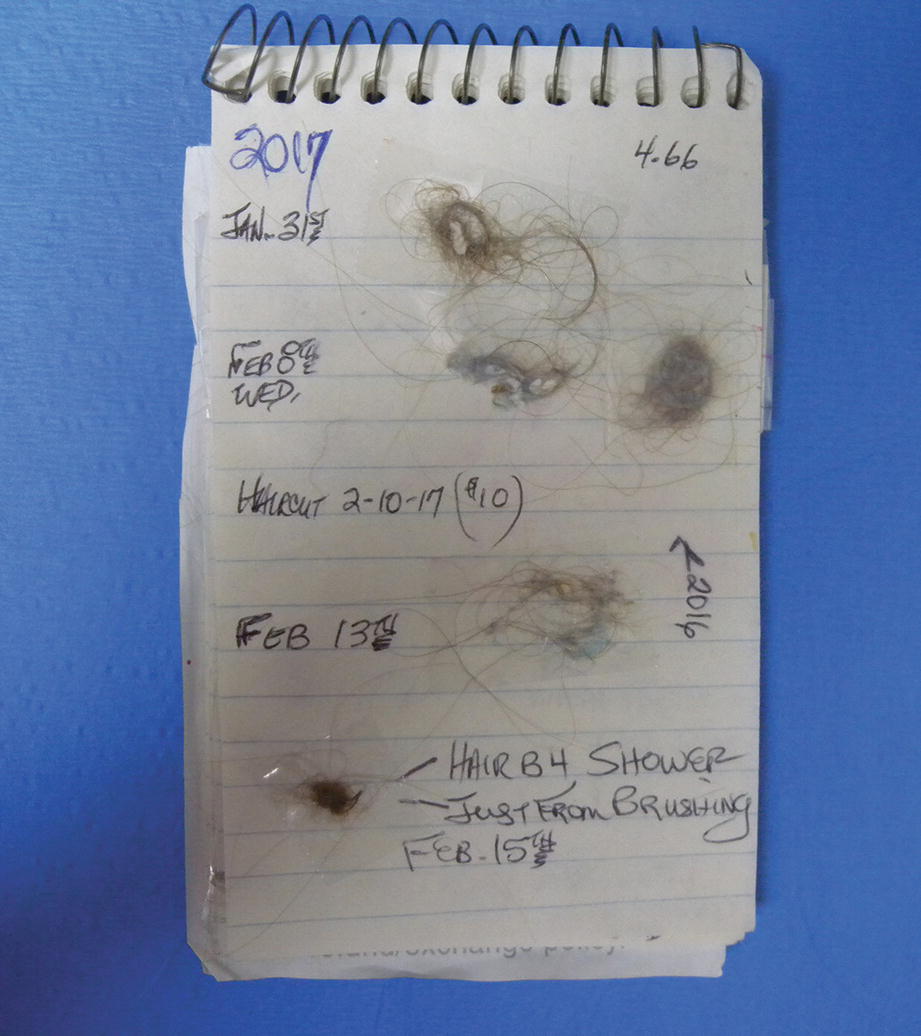
Example of a patient notebook describing hair shedding
The disease can have major psychological impact even when the hair appears to be normal in thickness on exam [2]. This psychologic effect can be seen in both men and women, but it has been reported to be more prominent in women [20].
Acute Telogen Effluvium
Acute telogen effluvium usually ceases within 3–6 months of initial symptom onset [12, 21]. Clinically significant regrowth and recovery usually takes about 6–12 months as hair requires time to grow to an adequate length. Full recovery may be delayed or never realized in older women due to the presence of concomitant androgenetic alopecia and aging follicles [22]. Evidence has suggested that it is relatively common for physicians to diagnose patients with androgenetic alopecia after a delayed recovery from acute telogen effluvium [2].
Chronic Telogen Effluvium
Chronic telogen effluvium is typified by an insidious onset and long fluctuating course with unexplained remissions and recurrences lasting several years [5, 23].
Its cause is usually multifactorial and difficult to establish. It is currently proposed that chronic telogen effluvium may be caused by an intermittent pathologic synchronization of the hair cycle, anagen phase shortening, or early teloptosis. It remains a diagnosis of exclusion, whereby it must be kept in mind that multiple-cause relationships may underlie this type of hair loss, including significant seasonal fluctuations of hair growth and shedding. The condition can resolve completely on its own, but it may take years to even a decade before a cessation in symptoms occurs [24].
Diagnostic Criteria

Demonstration of the correct method of the hair pull test

Telogen hair bulb visualized using microscopy
History and physical exam findings suggesting telogen effluvium
History | Physical exam |
|---|---|
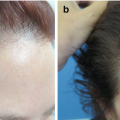
Acute inciting event (see Table 10.2) in previous 2–5 months before onset of hair loss [2] Trichodynia (pain , discomfort, or paresthesia of scalp) sometimes present, though nonspecific [29] Seasonal exacerbations Patient can identify the exact date when symptoms began | Very positive (more than ten hairs) hair-pull test [8] Microscopic examination of shed hair from hair-pull test showing telogen bulb [30] (see Fig. 10.5) Short regrowing frontal hairs [2] Beau’s lines of nails may signal recent severe medical illness [30] Dermoscopy [31]: Acute: empty follicles, multiple short regrowing hairs of normal thickness, may be associated with variability due to concurrent AGA Chronic: less than 20% hair diameter variability, differentiates vs. androgenic alopecia Found only in chronic telogen effluvium: No changes in hair diameter [5] Bitemporal thinning [5] Decrease in pony tail length and thickness Aggravates in the summer Normal pull test |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


