Dual Plane Breast Augmentation: Optimizing Implant-Soft-Tissue Relationships in a Wide Range of Breast Types
John B. Tebbetts, M.D.
Dallas, Texas
Received for publication August 4, 2000.
Dr. Tebbetts is a consultant to McGhan Medical Corporation, manufacturer of one of the types of saline-filled breast implants used in this study.
Reprinted and reformatted from the original article published with the April 2001 issue (Plast Reconstr Surg. 2001;107:1255–1272).
Copyright ©2012 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e318269b129
Summary: In breast augmentation, surgeons usually choose a pocket location for the implant behind breast parenchyma (retromammary), partially behind the pectoralis major muscle (partial retropectoral), or totally behind pectoralis major and serratus (total submuscular). Each of these implant pocket locations has specific indications, but each also has a unique set of tradeoffs. When applied to a wide range of breast types, each pocket location has limitations. Glandular ptotic and constricted lower pole breasts offer unique challenges that often are not solved without tradeoffs when using a strictly retromammary, partial retropectoral, or total submuscular pocket. This article describes specific indications and techniques for a dual plane approach to breast augmentation in several different breast types, introducing techniques that combine retromammary and partial retropectoral pocket locations in a single patient to optimize the benefits of each pocket location while limiting the tradeoffs and risks of a single pocket location. A total of 468 patients had dual plane augmentation between January of 1992 and March of 1998 using the specific techniques of dual plane augmentation described in this article. All patients were treated as outpatients and received general anesthesia. Indications, operative techniques, results, and complications for this series of patients are presented. Dual plane augmentation mammaplasty adjusts implant and tissue relationships to ensure adequate soft-tissue coverage while optimizing implant–soft-tissue dynamics to offer increased benefits and fewer tradeoffs compared with a single pocket location in a wide range of breast types. (Plast. Reconstr. Surg. 107:1255,2001.)
Three implant pocket locations are commonly used in augmentation mammaplasty: (1) behind breast parenchyma (retromammary),1 (2) partially behind the pectoralis major muscle (partial retropectoral,2–9 or (3) totally behind pectoralis major and serratus (total submuscular).10–12 Other authors13–17 have addressed the relative benefits and tradeoffs of implant pocket location with respect to capsular contracture rates. This article presents techniques that allow two pocket planes (dual plane) to be developed in a single patient, adjusting the implant and tissue relationships to ensure adequate soft-tissue coverage while optimizing implant–soft-tissue dynamics, to offer increased benefits and fewer tradeoffs compared with a single pocket location in a wide range of breast types.
Each of the previously listed implant pocket locations has specific benefits and indications, but each also has unique tradeoffs in specific breast types. For example, in a glandular ptotic breast with thin soft tissues in the superior pole of the breast, a partial retropectoral or total submuscular pocket location provides the necessary additional soft-tissue coverage superiorly but risks a
“double-bubble” deformity resulting from parenchyma sliding inferiorly off the pectoralis and implant. A constricted lower pole breast in a thin patient needs additional coverage superiorly, but muscle coverage inferiorly restricts optimal expansion of the constricted lower pole.
“double-bubble” deformity resulting from parenchyma sliding inferiorly off the pectoralis and implant. A constricted lower pole breast in a thin patient needs additional coverage superiorly, but muscle coverage inferiorly restricts optimal expansion of the constricted lower pole.
Because each pocket location has unique advantages and tradeoffs, applying a single pocket location to every primary augmentation may risk unnecessary compromises. Patients vary widely in soft-tissue characteristics, breast tissue, and their willingness to accept specific tradeoffs. When a surgeon uses only one pocket location for all primary breast augmentations, it is logical that compromises, complications, or less-than-optimal results will occur, because a single pocket location does not completely address the range of anatomic variations and implant–soft-tissue dynamics that occur in a wide range of breast types. Even if a surgeon chooses the most appropriate of the three pocket locations (retromammary, partial retropectoral, total submuscular) for a given patient, tradeoffs can still occur. For example, none of the three common pocket locations is optimal for the glandular ptotic breast or a constricted lower pole breast in a thin patient. Even in routine breast types without specific deformities, a surgically controlled combination of pocket locations can potentially maximize the benefits and minimize the tradeoffs of a single pocket location.
This article addresses two questions:
Can a combination of pocket locations in the same breast (dual plane; combination of retromammary and partial retropectoral) increase the benefits and decrease the tradeoffs of a single pocket location, increase surgical control and predictability of the result, and minimize the tradeoffs, risks, and complications?
When additional muscle coverage is indicated, can the surgeon adjust the anatomic position of the pectoralis major muscle relative to the implant to better control the implant–soft-tissue dynamics for an optimal result?
Definition of Dual Plane Augmentation
Dual plane augmentation is defined as any augmentation that meets the following three criteria:
The implant lies partially behind the pectoralis major muscle and partially behind the breast parenchyma (in dual planes simultaneously).
A specific group of pectoralis major muscle origins are totally divided in a specific area to alter implant–soft-tissue dynamics by anatomically repositioning portions of the pectoralis major relative to the implant (this criterion distinguishes dual plane from partial retropectoral augmentation).
The parenchyma-muscle interface is specifically altered to change the soft-tissue relationships between pectoralis major and parenchyma and to change the implant-parenchyma dynamics.
Two anatomic entities largely control the position of the pectoralis major muscle relative to a breast implant: (1) the origins of the muscle along the inframammary fold inferiorly and the sternum medially, and (2) the attachments of the pectoralis to the breast parenchyma at the parenchyma-muscle interface. To alter the position of the pectoralis major muscle relative to the implant, the surgeon divides origins of the pectoralis along the inframammary fold. The muscle then retracts superiorly until its superior retraction is stopped by attachments at the parenchyma-muscle interface or by remaining muscle origin attachments along the sternum.
In dual plane augmentation, the surgeon alters the position of portions of the pectoralis major muscle by (a) selectively dividing the inferior origins of the pectoralis along the inframammary fold only, with no muscle division along the sternum; and (b) freeing the attachments of parenchyma to muscle at the parenchyma-muscle interface by dissecting in the retromammary plane between the parenchyma and the pectoralis. These two maneuvers are performed at different times and to different degrees, depending on incisional approach, breast type, tissue characteristics, implant–soft-tissue dynamics, and the surgeon’s preferences.
Clinical Criteria and Methods
Each patient’s preoperative breast-envelope characteristics were clinically characterized as tight, normal, or excessively compliant (genetically or postpregnancy). Areola-to-inframammary-fold distance, sternal-notch-to-nipple distance, base width of the breast, and intermammary distance were measured and recorded preoperatively and at each postoperative visit. Soft-tissue pinch thicknesses of the upper pole and at the inframammary fold was measured with calipers. The position of the lower border of the pectoralis was noted pre-operatively and postoperatively by palpation and visualization while the patient contracted the pectoralis. The pocket location for the implant was chosen based on the criteria described below in order of priority.
Adequacy of Soft-Tissue Cover
Adequate soft-tissue cover over an implant is mandatory in both primary and reoperation cases. In primary cases, adequacy of soft-tissue cover in the upper
breast was assessed clinically by isolating the breast parenchyma inferiorly and firmly pinching the soft tissues superior to the parenchyma (Fig. 1, left) to quantitate soft-tissue pinch thickness of the upper pole. If this pinch thickness was 2 cm or greater, the patient was offered a retromammary pocket location, provided that an adequately filled, textured, anatomic implant was used. Soft-tissue pinch thickness was also measured immediately inferior to the inframammary fold (Fig. 1, right). If this pinch thickness was less than 0.4 cm, pectoralis major origins along the inframammary fold were left intact for additional soft-tissue coverage, and the patient was excluded from this study.
breast was assessed clinically by isolating the breast parenchyma inferiorly and firmly pinching the soft tissues superior to the parenchyma (Fig. 1, left) to quantitate soft-tissue pinch thickness of the upper pole. If this pinch thickness was 2 cm or greater, the patient was offered a retromammary pocket location, provided that an adequately filled, textured, anatomic implant was used. Soft-tissue pinch thickness was also measured immediately inferior to the inframammary fold (Fig. 1, right). If this pinch thickness was less than 0.4 cm, pectoralis major origins along the inframammary fold were left intact for additional soft-tissue coverage, and the patient was excluded from this study.
If the patient preferred a round implant, smooth or textured, the potential upper pole collapse of the round implant filled to the manufacturer’s recommendations necessitated a partial retropectoral pocket to minimize risks of visible underfill rippling. If the patient requested a markedly bulging upper breast with a step-off (the “Baywatch” breast), she was encouraged to select either an overfilled round implant, a larger round implant filled to the manufacturer’s recommendations, or a larger anatomic implant. Tradeoffs that all patients were required to accept by informed consent included the possibility of an increased (a) risk of a visible or palpable implant edge, (b) capsular contracture rate resulting from increased implant exposure to parenchyma, and (c) interference with mammographic interpretation as implant contact with parenchyma increased.
Patient Preference
If a patient preferred one pocket location over another, the tradeoffs and risks of that pocket location were discussed with the patient, and the patient’s wishes were honored provided that adequate soft-tissue cover was present. If <2 cm of pinch thickness was present superior to the breast parenchyma, the patient was required to accept muscle coverage in the upper breast to ensure adequate coverage with any type of implant, or the patient was not operated on. Pocket locations with potential benefits and tradeoffs included in the information materials and discussed with each patient are listed in Table 1.
Table 2 lists the potential benefits and tradeoffs of the dual plane pocket location compared with strict retromammary or partial retropectoral pocket locations described in Table 1.
In this series of patients, when inadequate soft-tissue coverage (<2 cm pinch thickness) was present superior to the breast parenchyma, upper pole muscle coverage was mandatory. When muscle coverage was indicated or preferred by the patient, three options were discussed: (1) partial retropectoral (with pectoralis origins intact along the inframammary fold and sternum), (2) total submuscular (adding serratus laterally for total muscle coverage), and (3) dual plane (with complete division of pectoralis origins along the inframammary fold, not along the sternum). The goal of the dual plane approach was to optimize the benefits while limiting the tradeoffs of the retromammary, partial retropectoral, and total sub-muscular approaches. Patients who elected the dual plane pocket location after considering all alternatives were included in this study. Preoperatively, all patients, regardless of tissue thickness, were advised of the following in informed-consent documents:
If you can feel your ribs with your finger, beneath the breast or at the side of your breast, you will be
able to feel the edge of your implant beneath your breast and at the side of your breast.
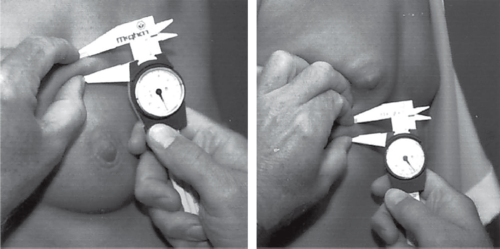
Fig. 1. Soft-tissue pinch thickness of the upper pole (left) and immediately inferior to the inframammary fold (right) is caliper-measured with a firm pinch of the skin and subcutaneous tissue.
Table 1. Alternative Pocket Locations with Potential Tradeoffs
Pocket
Tradeoffs
Potential Benefits
Retromammary
- Increased risk of edge visibility or palpability.
- Possible increased interference with mammography.
- Possible increased incidence of capsular contracture.
- Increased control of breast shape.
- Usually a more rapid postoperative recovery.
- Minimal or no distortion with pectoralis contraction.
- Increased control of inframammary fold position and shape.
Partial retropectoral (without dividing pectoralis origins along the inframammary fold)
- Lateral implant displacement over time, widening the space between the breasts.
- Less control of upper medial fill.
- More postoperative tenderness and a more prolonged recovery.
- Distortion of breast shape with pectoralis contraction.
- Less precise control of inframammary fold position, depth, and configuration. This potential tradeoff is minimized or eliminated by division of pectoralis origins along the inframammary fold in patients who have adequate soft-tissue coverage.
- Increased risk of superior implant malposition or displacement (when inferior pectoralis origins across inframammary fold are not divided).
- Longer time required for deepening of the inframammary fold (when pectoralis origins along the inframammary fold are not divided).
- Muscle coverage mandatory if pinch thickness <2 cm above breast parenchyma.
- Possibly more accurate mammograms.
- Less risk of palpable or visible implant edges.
- Possible decreased risk of capsular contracture (small difference with saline-filled implants, greater difference with silicone gel-filled implants).
Total submuscular
- All tradeoffs listed above for partial retropectoral, plus:
- Highest risk of superior implant displacement or malposition.
- Longer operative time.
- Longest postoperative recovery and morbidity.
- Least accurate and predictable inframammary fold and longest to achieve depth.
- Greatest risk of inframammary fold irregularities, lateral flattening, and fold level inaccuracies.
- Possible increased coverage inferolaterally but clinically no significant additional cover long-term.
- Increased risk of edge visibility or palpability.
Currently manufactured implants that strive to achieve durability of the shell have a thicker shell to prolong the life of your implant, and a thicker shell may be easier for you to feel.
If feeling an edge of an implant shell could be a problem for you, do not have an augmentation.
We cannot change the quality or thickness of your tissues. If you are thin or have very little breast tissue, you will be more likely to feel your implant.
The larger your implant, the worse your breast will look over time. A larger implant will stretch your tissues over time and will cause more tissue-thinning and sagging than a smaller implant. Your tissues do not improve with age, and they will be less able to support the additional weight of any implant, especially a larger implant.
Any implant, if filled adequately to prevent collapse and possible folding of the shell when you stand, will feel firmer than a normal breast, regardless of the filler material. If the implant shell folds, it could fail sooner and require you to have a reoperation sooner18 (most patients accept a firmer breast in exchange for a possibly longer life of the implant shell).
If you want a totally natural breast, you should not have a breast augmentation.
Three Types of Dual Plane Augmentation
Three variations of muscle division and pa-renchyma-muscle interface dissection were used in this study:
Type I dual plane: complete division of pectoralis origins across the inframammary fold, stopping at the medial aspect of the inframammary fold, with
no dissection in the retromammary plane to free the parenchyma-muscle interface (Fig. 2, above).
Table 2. Potential Benfits and Tradeoffs of the Dual Plane Pocket Location
Pocket
Tradeoffs
Potential Benefits
Dual plane (compared with retromammary)
- Preserves the potential increased control of lower breast shape with retromammary.
- With proper techniques can have similar recovery as with retromammary.
- Reduced risk of edge visibility or palpability of retromammary by providing more upper pole coverage.
- Reduced interference with mammography by retromammary.
- Reduced possibility of capsular contracture of retromammary by reducing contact with parenchyma compared with retromammary.
Dual plane (compared with partial retropectoral)
- Possible increased risk of palpable or visible implant edges inferiorly
- Provides same mandatory muscle coverage if pinch thickness <2 cm above breast parenchyma.
- Reduced risk of lateral implant displacement over time; dividing inferior origins decreases pectoralis pressure on implant.
- Better control of upper medial fill with division of inferior origins to decrease pectoralis tension and pressure on upper pole of implant.
- Reduced postoperative tenderness and recovery period with proper technique.
- Reduced distortion of breast shape with pectoralis contraction.
- Decreased risk of superior implant malposition or displacement by decreasing pressure of pectoralis on lower pole of implant by dividing lower pectoralis origins.
- Increased control of inframammary fold position, depth, and configuration by decreasing pressure of pectoralis on lower pole of implant along inframammary fold.
- Retains possibility of more accurate mammograms, depending on position of muscle.
- Possible decreased risk of capsular contracture (small).
- Preserves the potential increased control of lower breast shape with retromammary.
Type II dual plane: complete division of pectoralis origins across the inframammary fold, stopping at the medial aspect of the inframammary fold (Fig. 2, center), followed by dissection in the retromammary plane to approximately the inferior border of the areola.
Type III dual plane: complete division of pectoralis origins across the inframammary fold, stopping at the medial aspect of the inframammary fold (Fig. 2, below), followed by dissection in the retromammary plane to approximately the superior border of the areola.
The medial origins of the pectoralis along the sternum were not completely divided in any patient to avoid four potential problems: (1) visible deformities that can occur along the sternum from cut muscle edges adhering to subcutaneous fat and excessive risk of visible implant edges beneath thin parasternal skin; (2) visible implant edges beneath thin skin and subcutaneous tissue in the intermammary space; (3) visible traction-rippling medially that can occur with any implant when the implant places traction on a capsule attached to thin, overlying tissue; and (4) possible synmastia. The distinct, isolated, white, tendinous-looking medial origins of the pectoralis that are located lateral to the main body of parasternal origins along the sternum in some patients were divided to maximally enlarge the medial pocket without risking the tradeoffs of complete division along the sternum. Complete division of the medial origins of pectoralis along the sternum allows slightly greater narrowing of the intermammary distance but greatly increases the risks described previously, and the risks far outweigh the potential benefits.
Selection of Technique by Breast Type
One of the three dual plane techniques was selected for each patient, according to the requirements dictated by the patient’s anatomy and desired implant–soft-tissue dynamics required for an optimal result. The goal was to match the surgical technique to the needs of the breast to (1) maximize soft-tissue coverage and
minimize forces that could cause undesirable implant displacement, (2) avoid restricting optimal expansion of the lower pole, and/or (3) reduce the risks of inferior displacement of breast parenchyma sliding off the pectoralis.
minimize forces that could cause undesirable implant displacement, (2) avoid restricting optimal expansion of the lower pole, and/or (3) reduce the risks of inferior displacement of breast parenchyma sliding off the pectoralis.
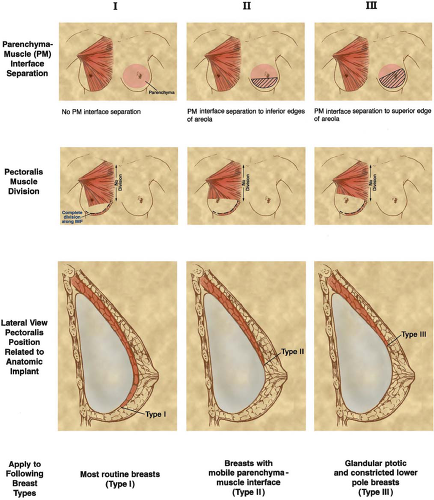 Fig. 2. Extent of dissection at the parenchyma-muscle interface (above), the position of the inferior edge of divided pectoralis origins (center), and pectoralis position relative to the implant (below) for types I, II, and III dual plane augmentation techniques. |
A type I dual plane technique was selected for most routine breasts that fit the following three criteria (Fig. 3):
Related posts:
 Breast Augmentation
Breast Augmentation
 Breast Augmentation
Breast Augmentation
 The Process of Breast Augmentation: Four Sequential Steps for Optimizing Outcomes for Patients
The Process of Breast Augmentation: Four Sequential Steps for Optimizing Outcomes for Patients
 Acellular Dermal Matrices in Breast Augmentation
Acellular Dermal Matrices in Breast Augmentation
 Brava and Autologous Fat Transfer Is a Safe and Effective Breast Augmentation Alternative: Results of a 6-Year, 81-Patient, Prospective Multicenter Study
Brava and Autologous Fat Transfer Is a Safe and Effective Breast Augmentation Alternative: Results of a 6-Year, 81-Patient, Prospective Multicenter Study
 Understanding the Fascial Supporting Network of the Breast: Key Ligamentous Structures in Breast Augmentation and a Proposed System of Nomenclature
Understanding the Fascial Supporting Network of the Breast: Key Ligamentous Structures in Breast Augmentation and a Proposed System of Nomenclature
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


