Drain-free abdominoplasty using progressive tension sutures (PTS) was initially described in 2000 in a small retrospective series. However, the authors’ experience with this technique spans well over 3 decades, and their technique has evolved to simplify the procedure to make it easier and more reproducible by the surgeon and improve the patient’s recovery and overall experience. This article provides in-depth technical details on the authors’ no-drain abdominoplasty technique. The authors also address through recent literature some of the commonly stated barriers to surgeons instituting this technique into their abdominoplasty procedure, including excessive time of placement, dimpling, and effectiveness.
Key points
- •
The goal of this chapter is to give clear and in-depth detail to allow a surgeon to incorporate Progressive Tension Sutures (PTS) into their practice.
- •
Specifically, a detailed technical description of PTS placement is included with helpful tips to decrease time, dimpling and frustration for those new to the technique.
- •
Complete details of the authors drain-free abdominoplasty technique using progressive tension sutures including post-operative care, pain management, compression and early activities for improved the patient’s experience.
- •
Details of an in-continuity umbilical inset for a natural appearing neo-umbilicus.
- •
Criticisms of PTS such as dimpling and increased operative time are addressed with clear suggestions on eliminating these as barriers to using this technique.
Drainless abdominoplasty using progressive tension sutures
Demand for abdominoplasty continues to grow as bariatric surgery becomes more common, adding to those seeking body contouring for medical weight loss and post-partum abdominal changes. Because of this increase, many changes have been seen in abdominoplasty, improving safety and aesthetics. As a group, surgeons tend to be relatively conservative and slow to change surgical techniques that they either learned in training or have used successfully over many years in practice. This is especially true when that change is something that previously has been considered essential to the operation. And so it is with the use of drains in abdominoplasty. To many plastic surgeons the suggestion of eliminating drains in abdominoplasty is nothing short of sacrilege. From a patient’s perspective dread drains preoperatively, find them uncomfortable and burdensome postop, and remember them as the worst part of the abdominoplasty experience. Additionally the use of drains still result in a significantly high rate of seromas adding to office time and expense as well as patient inconvenience and negative experiences.
Today there are several abdominoplasty techniques that promote eliminating drains while decreasing or maintaining seroma rates relative to traditional methods. It seems, however, that seroma prevention should start with an understanding of the cause of seroma in abdominoplasty. Although still debated, common theories include excessive dead space, interruption of lymphatic function, and flap motion leading to repeated interference in the healing process. The authors believe that it is this latter theory of motion that contributes most to seroma formation in abdominoplasty, as the strong and multidirectional movement of the abdomen repeatedly disrupts nascent healing. This repeated disruption leads to increased inflammation and generation of the inflammatory exudate found in abdominoplasty seromas. Secure fixation of the 2 wound surfaces provided by progressive tension sutures allows for uninterrupted healing, which minimizes inflammation and fluid production.
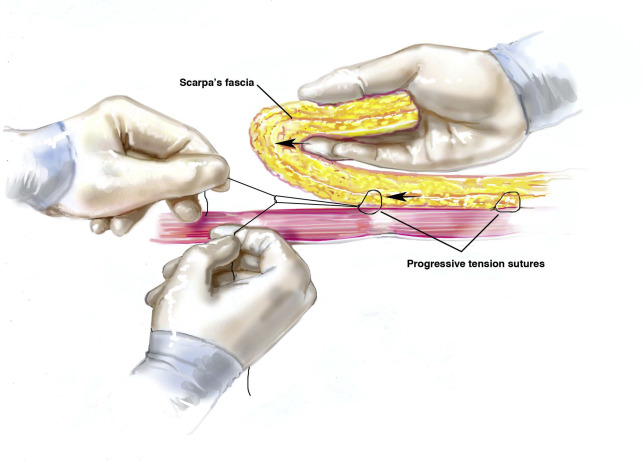
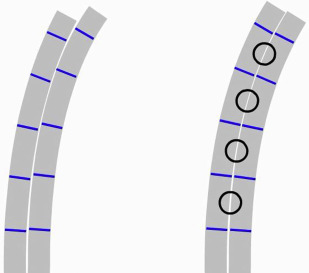
Progressive tension sutures (PTS) are sutures that securely affix a flap in its advanced position over multiple points to the underlying tissue. In abdominoplasty, the sutures are placed from the superficial fascia of the flap to the muscle fascia ( Fig. 1 ). These sutures act not only to secure the flap to the underlying tissue to prevent disruption with abdominal motion but also close dead space ( Fig. 2 ) and broadly distribute tension over the entire flap.
The authors’experience in using this method preceede the original paper by decades with documentation found in operative notes dating back to 1980. The technique has evolved significantly over time in order to make it more consistent and reproducible. The authors first published the concept of PTS and its use in abdominoplasty to reduce the rate of seromas while eliminating drains in 2000. Since publication of that small consecutive series, the authors updated technical modifications and reviewed their experience in 597 consecutive patients. They also published papers using PTS in facelift, browlift, and latissimus dorsi donor site. But few good ideas develop in isolation, and others have described similar techniques with comparable results. ,
The goal of this article is to describe the technical details of placement of PTS in the context of the authors’ abdominoplasty procedure in adequate detail to allow a surgeon to incorporate the use of PTS into their practice.
In addition, they review common barriers surgeons have noted in adding PTS to abdominoplasty and provide ways to avoid these problems. They also review evidence of the effectiveness of PTS in abdominoplasty and support the elimination of suction drains while decreasing the rate of seroma formation.
Surgical technique
The primary focus of this article is to provide the surgeon with the technical detail that will allow them to begin to use the progressive tension suturing technique in their abdominoplasties successfully and with as little frustration as the learning curve will allow. The authors also detail their general approach to abdominoplasty to share with the reader what they have found to be successful. But, by no means is this protocol meant to be a recipe that requires exact duplication for success. It is very important to understand that PTS is a technical adjunct that can be applied to most abdominoplasty techniques as well as other procedures that involve an advancement flap.
Patient Selection
All patients are assessed for their overall health, surgical risk, and specific indications for body contouring. Patients older than 50 years or with significant health issues are referred to their primary care physician or an appropriate specialist for preoperative clearance and any specific perioperative recommendations for that patients’ individual medical condition.
Body mass index (BMI) is considered in assessing a patient’s appropriateness for abdominoplasty, and the association of higher BMIs with the increase in complications is respected. But a specific BMI is not considered an absolute contraindication. Patients are evaluated on an individual basis, as well-developed musculature and large bone structure affect BMI negatively without the associated surgical risks seen in obesity. In individuals deemed too great a surgical risk, care is taken to explain their unacceptably risk and a referral to a weight loss specialist is made.
Body contouring procedures on patients who have had a bariatric procedure and lost a significant amount of weight are delayed until weight has been stable for at least 6 months. Patients who have lost weight through diet and exercise over a slower period may be operated on after only 3 months of stable weights if their diet is not one of high caloric restrictions. A nutritional assessment is done in all weight loss patients.
Venous thromboembolic (VTE) risk is assessed using Caprini’s identified risk factors and prophylaxed based on these risk factors. All patients have sequential compression devices placed before induction and are ambulated early postoperatively. Chemoprophylaxis is reserved for patients considered high VTE risk and in those who show poor postoperative advancement in ambulation. Subcutaneous enoxaparin is started approximately 8 hours postop for a 7-day course. The patients are ambulated early postop in an upright position. The goal is to ambulate the patient in an upright posture 4 hours following surgery completion. Although considered a VTE risk, compressive garments are used in most cases. More details will be addressed in the section discussing postoperative care. As a final word on this topic, it seems clear that the science of VTE prevention is incomplete and surgeons must rely on their best judgment based on the knowledge available.
Patients who smoke are encouraged to stop but are not strictly required to do so in most instances. The patient is engaged in a candid discussion about smoking’s effects on wound healing, VTE, and pulmonary risks and the conversation is documented. A patient’s unwillingness to cease smoking is factored into their overall risks, and a determination is made on that patient’s acceptability as a surgical candidate. In the authors’ series, 13.7% of patients admitted to smoking and those patients had no greater incidence of complications.
Preop Prep and Markings
Patients are marked in an upright position denoting anatomic landmarks, areas of adiposity, and any special considerations such as a lap band port, scars, contour irregularities, or other characteristics of relevance. Areas of adiposity are marked topographically. The incision is marked on the table, as it has been noted that when marked standing it can be displaced superiorly when the patient is placed supine on the table.
The one exception is patients who are having an extended or circumferential procedure in which some excision must be done in a prone position and later joined with the anterior excision. In this case, the anterior- and posterior-lateral excision is planned and marked with the patient standing. The patient is then placed supine and a mark is made at the farthest posterior point along the incision that can be easily worked on from a supine position. This is typically around the midaxillary line or a little posterior. An ellipse is then designed with the posterior excision that ends near that point marked. This marks what will be excised while the patient is in a prone position. Cross-hatching is helpful in aligning the wound edges after excision, and these can be marked at this point or on the table.
Approximately three-quarters of the patients are operated under general anesthesia. The patients are warmed preoperatively in the holding area, and sequential compression devices are applied and begun immediately on entering the operating room. If a concomitant breast procedure is planned, the breasts are not included in the abdominal prep to allow for forced air warming of the upper body while the abdomen is addressed. If available, a bed-warmer is useful in maintaining patient’s temperature.
The patient is initially placed prone on the operating table if posterior liposuction or excision is indicated. In most patients some posterior liposuction is used to achieve a good flank contour and rounding of the superior buttocks. The areas to be suctioned (and excised) are infiltrated with wetting solution containing epinephrine only (Lactated Ringers 1 L, 1:1000 epinephrine 1 mL). Local anesthetic adds nothing to the patient under general anesthesia, and it is feared that when liposomal bupivacaine is used, the pooled lidocaine may have a detrimental effect of premature freeing the bupivacaine from the liposomes even after the recommended wait of 20 minutes. The authors infiltrate at approximately a 1:1 ratio with what is anticipated to be removed or as a superwet infiltration. In most cases, the authors choose to infiltrate by hand for more even distribution and for better control of the volume.
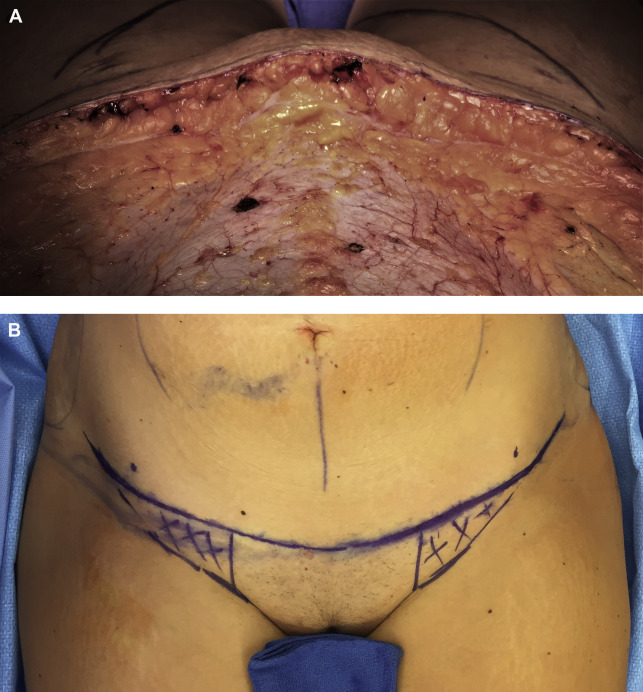
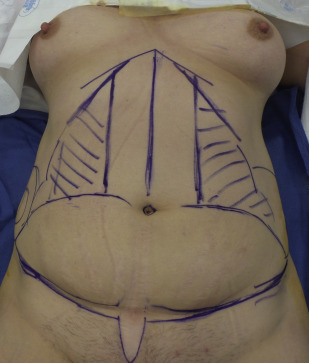
When the patient is turned to a supine position the abdomen is marked. Markings are made denoting the incision, approximate area to be excised, costal margin, iliac crest, and approximate lateral rectus ( Fig. 3 ). This helps direct liposuction and areas to avoid over defatting based on their postoperative position on the flap. The incision is designed in a gentle curvilinear shape. The central incision over the mons pubis is relatively flat and placed 6 to 7 cm above the vulvar commissure. This measurement and marking need to be done with the mons elevated to the desired postoperative position. The incision is extended at a superiorly directed angle to just below the anterior superior iliac spine. Again, this should be marked while elevating the lower inguinal tissues to their desired postoperative height. The planned incisions are infiltrated with 0.25% Bupivicaine with epinephrine and the areas of liposuction as well as dissection are infiltrated with the same epinephrine-only wetting solution previously described for vasoconstriction and hydrodissection.
In most patients, the greatest amount of liposuction is done in the lateral abdomen and anterior flanks. Liposuction is used as needed under the abdominal flap and in adjacent areas to achieve the desired aesthetic appearance based on individual patient assessment. The authors use liposuction in most of the patients. Their published series documented 67% of patients having suction in the flank and abdomen. Suctioning done under the abdominal flap is limited to the subscarpal plane. The authors use their variation of SAFE liposuction technique with the power-assisted liposuction device in all cases. A 5.0-mm basket cannula is used without suction followed by suctioning with a 5.0-mm double Mercedes cannula. The “equalization” portion of the SAFE liposuction technique is often omitted.
The authors elevate the abdominal flap with the electrocautery on a cut/coagulation blend and attempt to stay a few millimeters above the muscle fascia leaving a small amount of areolar tissue. Elevation is at that level over the entire abdomen without attempt to preserve Scarpa’s fascia. The exception is at the level of the incision, between the lateral Mons and the iliac crest where a cuff of superficial fascia is developed to suture later in order to assure inclusion of fascia in closure while avoiding a deeper suture bite in this area. This minimizes risk of lateral femoral cutaneous nerve entrapment or irritation ( Fig. 4 ). Although electrocautery dissection has been implicated in seroma formation and preservation of Scarpa’s fascia has been touted as a means to decrease seroma risk, the authors have had no problems maintaining a very low seroma rate with this technique. The degree of dissection is individualized but wide dissection to the costal margin is most common. Dissection above the costal margin is rarely used except in the central area over the xyphoid to assure diastasis repair is to its most superior extent.