Flap |
|
Tissue |
Skin |
Course of the vessels |
In the intermuscular septum |
Dimensions |
2 × 4 cm; reverse flap located over the proximal metacarpals; antegrade flap located over the proximal phalanx |
Extensions and combinations |
Rarely may include tendon strips from the proper extensor indicis or the proper extensor digiti minimi |
Anatomy |
|
Neurovascular pedicle |
— |
Artery |
DMCA nourished from the dorsal arterial arch or through the volar–dorsal perforator from the volar arch |
Veins |
Small venae comitantes |
Length and arc of rotation |
Reverse pedicle flap reaches the proximal interphalangeal joint; antegrade flap reaches the proximal wrist extensor crease |
Diameter |
— |
Nerve |
— |
Surgical technique |
|
Preoperative examination and markings |
Preoperative Doppler examination for the presence of vessels is mandatory; reliability declines from radial to ulnar aspect; the DMCA artery 4 is only present in approximately 80% of patients |
Flap design |
— |
Patient position |
Supine with arm on arm table; risk of tourniquet-induced ischemia |
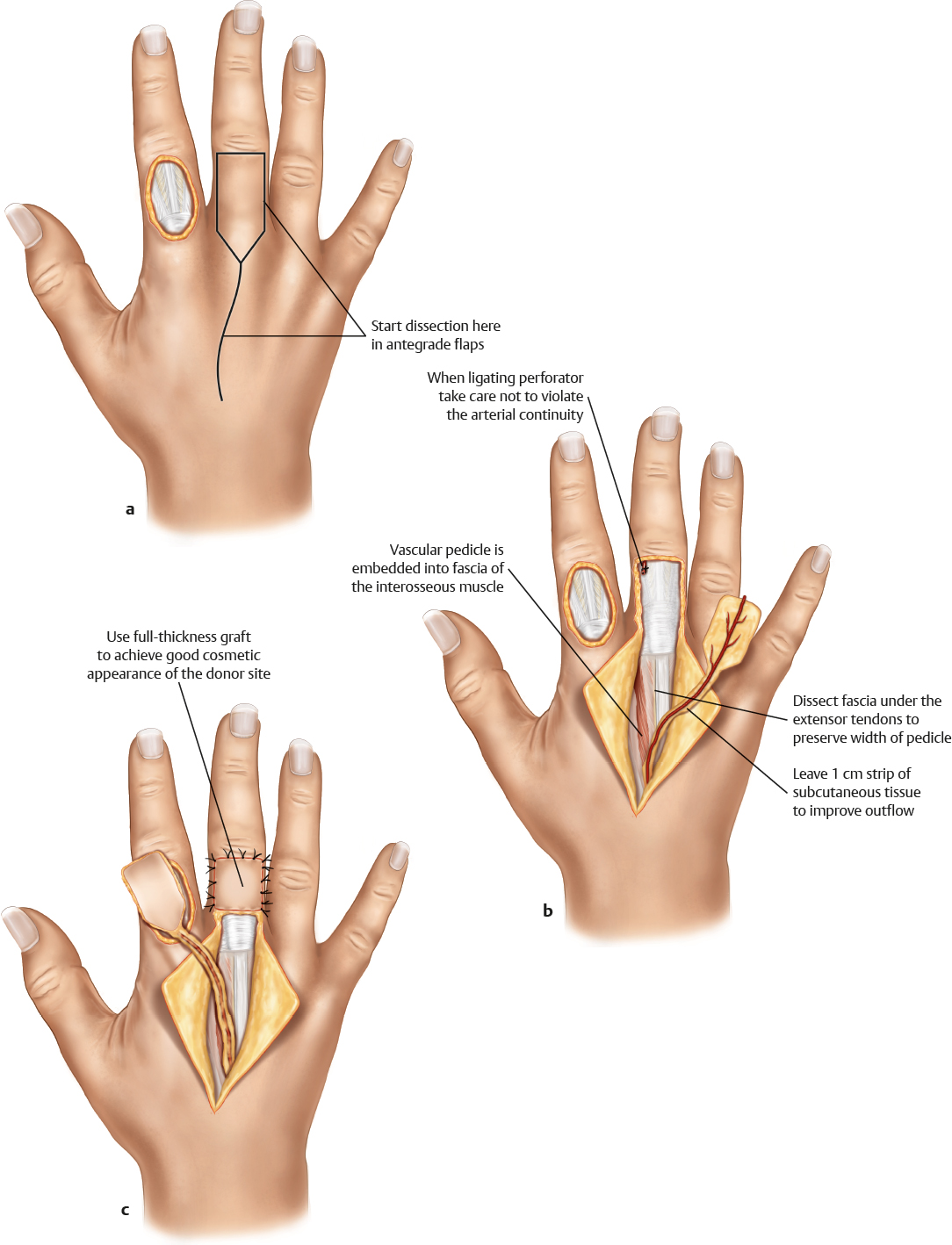
Dissection |
Antegrade pedicle: incise skin along markings; incise interosseous muscle fascia; preserve intermuscular septum and raise fasciocutaneous flap, including fascia; create de-epithelialized pedicle toward volar–dorsal perforator at the level of the metacarpal head; leave approximately 0.5–1 cm of fatty tissue around the artery; ligate the distal pedicle; open the tourniquet; check for perfusion; inset the flap at the recipient site; wait for normal perfusion
Reverse pedicle: incise skin along markings; incise interosseous muscle fascia; preserve intermuscular septum and raise fasciocutaneous flap, including fascia; create de-epithelialized pedicle toward the volar– dorsal perforator at the level of the metacarpal head; leave approximately 0.5–1 cm of fatty tissue around the artery; ligate the proximal pedicle; open the tourniquet; check for perfusion; rotate and inset the flap into the recipient site; wait for normal perfusion |
Advantages |
|
Vascular pedicle |
Both are reliable pedicles with wide arcs of rotation |
Flap size and shape |
Can cover even larger digital defects |
Combinations |
Can be combined with adjacent DMCA flaps for multidigital injuries |
Tissue |
Thin and pliable |
Disadvantages |
|
Donor site morbidity |
Only donor sites of smaller flaps can be closed primarily; skin grafts on the dorsum of the hand can be conspicuous; contour defects improve with time |
Pedicle |
Veins cannot be identified in most cases; flaps often appear ischemic during the first few minutes after deflating the tourniquet; venous congestion may occur |
Pearls and pitfalls |
|
Dissection |
Do not make the arc of rotation too narrow, because venous congestion may occur; preserve the paratenons of the extensor tendons for perfect skin graft take in the donor site; when the tunnel for the flap seems too narrow, create a skin graft pedicle; apply leeches early when venous congestion occurs; avoid any tension on the pedicle; when the flap does not show adequate reperfusion after the opening of the tourniquet, rinse the area with warm saline; it may take 20 minutes to re-establish blood flow |
Extensions and combinations |
Bony segment from the metacarpal may be possible |
Contouring and correction |
Rarely required; flaps shrink with time |
Clinical applications |
Reserve pedicle flap: small- and medium-sized dorsal digital defects as far as the proximal interphalangeal joint |