Disorders with Short Stature
Kurt Hirschhorn M.D.
Judith Willner M.D.
Clinical Pearls
(KH)
(JW)
Cornelia de Lange Syndrome
Synonym
De Lange syndrome
Brachmann-de Lange syndromse
Inheritance
Most cases are sporadic; autosomal dominant transmission favored in familial cases—variety of chromosomal abnormalities have been reported; recurrence risk estimated at 2% to 5% in families with affected child; nipped-β-like (NIPBL) gene on 5p13.1 has been identified in some cases
Prenatal Diagnosis
Fetal ultrasound—detection of intrauterine growth retardation and/or major structural abnormalities with positive family history
Incidence
Over 1:10,000 (estimate); M=F
Age at Presentation
Birth
Pathogenesis
Mutation in NIPBL gene may play a role in some cases
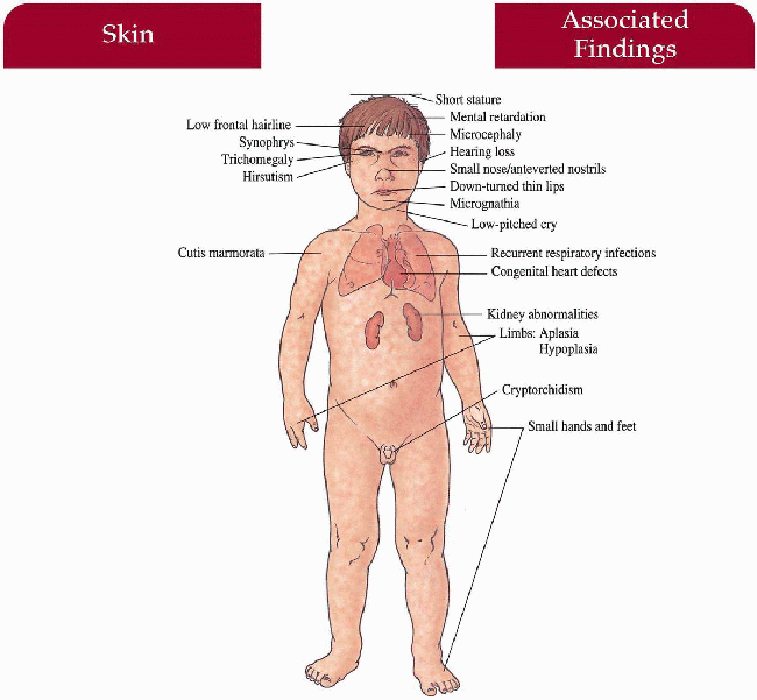
Key Features
Skin
Cutis marmorata, hirsutism, hypoplastic nipples and umbilicus
Craniofacial
Synophrys, trichomegaly (long eyelashes), microcephaly, small nose, anteverted nostrils, long philtrum, downturned, thin lips, late erupting, widely spaced teeth, micrognathia, low-set ears, low hairline, short neck
Central Nervous System
Severe mental retardation, psychomotor retardation, hypertonicity, low-pitched cry in infancy, behavioral problems
Musculoskeletal
Short stature beginning prenatally, small hands and feet, malformed upper limbs/hands with fifth finger clinodactyly, proximally placed thumbs, simian crease; flexion contracture of elbows, syndactyly of second and third toes
Genitourinary
Cryptorchidism, hypospadias, renal anomalies, bicornuate uterus
Cardiovascular
Variety of congenital heart defects
Ear-Nose-Throat
Hearing loss
Lungs
Recurrent infection
Differential Diagnosis
Dup (3q) syndrome
Laboratory Data
Echocardiagram
Abdominal ultrasound
BEAR hearing evaluation
Chest x-ray
Management
Close routine care with pediatrician—infection control; follow psychomotor, behavioral development
Referral to symptom-specific specialist
Prognosis
Often premature death secondary to aspiration, recurrent pulmonary infection; usually severely retarded (IQ often < 35)
Clinical Pearls
Usually sporadic but there have been many familial reports… I (KH) have described a family with three affected children… May turn out to be a microdeletion syndrome … Newborns are very small for gestational age… Facies is striking, characteristic… Makes them look unhappy, almost like a Greek tragedy mask… Although usually severely retarded, some kids have borderline-normal IQs… Downturning, or carp-like mouth is typical… Probably a fairly common syndrome. KH, JW
|
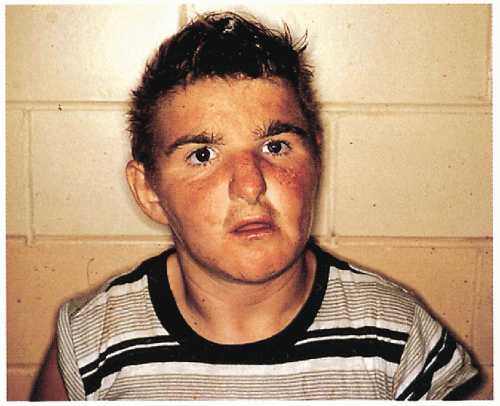
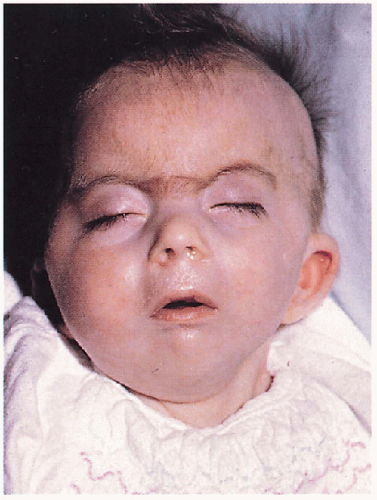 13.1. Infant with marked hirsutism on forehead, synophrys, trichomegaly, anteverted nostrils, long philtrum, and low-set ears. (138) |
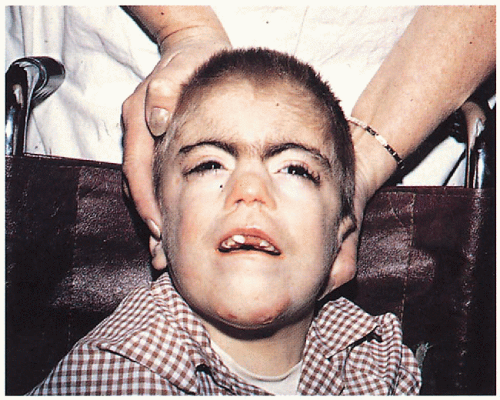 13.2. Similar features in a wheelchair-bound boy. Note late-erupting teeth. (138) |
Rubinstein-Taybi Syndrome
Inheritance
Sporadic; 1% recurrence rate within families of affected child; autosomal dominant transmission proposed; human CREB-binding protein (CREBBP) on 16p13.3
Prenatal Diagnosis
DNA analysis available in future
Incidence
Over 225 cases reported; 1:300 to 500 institutionalized, mentally retarded people over 5 years of age; M=F
Age at Presentation
Birth to neonatal period
Pathogenesis
Mutations in the CREBBP gene, a gene encoding a nuclear protein acting as a coactivator of cAMP regulated gene expression may be responsible for developmental abnormalities, neoplasms, and keloids
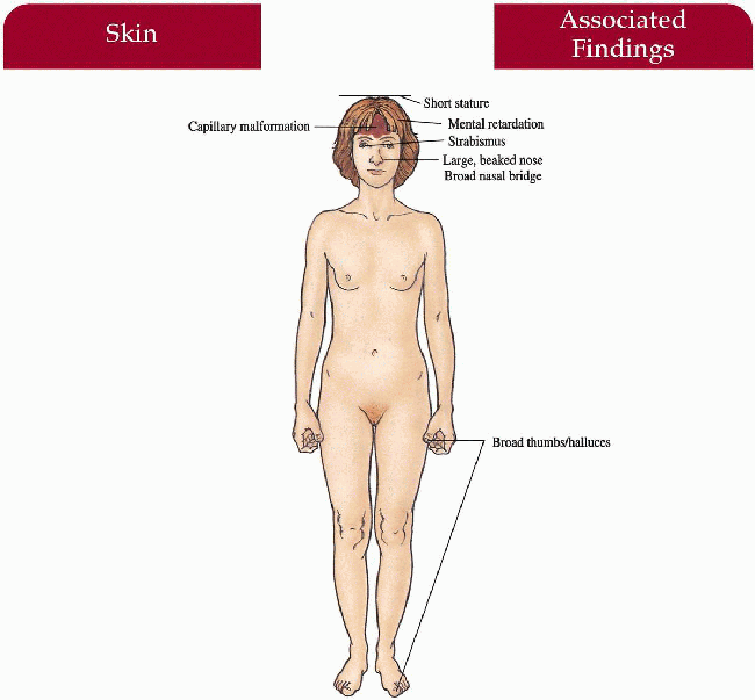
Key Features
Skin
Capillary malformation (50%)
Musculoskeletal
Broad thumbs and halluces (broad terminal phalanges with/without angulation deformity), short stature, stiff gait
Craniofacial
Beaked nose with nasal septum below alae, broad nasal bridge, downslanting palpebral fissures, high-arched palate, epicanthal folds, “grimacing” smile, mild micrognathia, microcephaly
Central Nervous System
Severe mental retardation with speech delay, motor retardation
Eyes
Strabismus
Genitourinary
Cryptorchidism (80%), variety of anomalies
Cardiovascular
Congenital heart defects (35%)
Differential Diagnosis
None
Laboratory Data
X-ray of hands and feet
Management
Close routine care with primary care physician—follow psychomotor, language and speech development
Referral to symptom-specific specialist
Prognosis
May have increased mortality in infancy/early childhood secondary to respiratory distress/infections, feeding difficulties, cardiac failure; often normal life span with IQ ranging from 40 to 50
Clinical Pearls
Big thumbs, big toes, large beaked nose… Antimongolian eyes… Typical facies in nursery… Deletion in 16p has been described in a number of cases… Prenatally, best looking for the microdeletion… Severity of syndrome based on how much gene is clipped off… In our experience, fairly rare syndrome… Severely retarded. KH, JW
|
 13.3. Boy with beaked nose, nasal septum below alae, broad nasal bridge, and “grimacing smile.” (139) |
 13.4. Broad thumbs with angulation deformity. (139) |
Russell-Silver Syndrome
Synonym
Silver-Russell syndrome
Inheritance
Almost all cases are sporadic; rare reports of familial transmission
Prenatal Diagnosis
None
Incidence
Over 150 cases reported: M=F
Age at Presentation
Birth
Pathogenesis
Unknown
Key Features
Skin
Café au lait macules
Musculoskeletal
Short stature starting prenatally, motor milestones delayed, asymmetry of head, limbs or trunk, clinodactyly of fifth finger, syndactyly between second and third toes
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


