Abstract
This chapter organizes diseases alphabetically for quick reference. Each disease is covered with sections that include General Comments (including the definition and etiology), Keys to Diagnosis (clinical manifestations and tests), Differential Diagnosis, Treatment, and Clinical Pearls. When pertinent, the treatment section is broken down into first-, second-, and third-line treatments. Almost all entities have representative clinical photographs to aid in the establishment of the diagnosis. Also included in some disorders are pertinent photographs of diagnostic tests such as scabies preparations and KOH examination for fungal infections.
Keywords
differential, etiology, examination, manifestations, pearls, photographs, tests, treatment
1
Acanthosis Nigricans
 General Comments
General Comments
Definition
- •
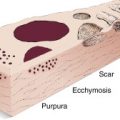
Acanthosis nigricans (AN) refers to the presence of symmetrical, brown, velvety, or verrucous plaques with a predilection for intertriginous sites, including the back of the neck, groin, and axillae ( Fig. 3.1 ).

FIG. 3.1
Velvety thickening of skin in flexural areas such as the axilla with brown-black hyperpigmentation with lighter-colored deep skin lines.
Etiology
- •
It is most commonly seen in obese individuals with insulin resistance or an internal malignancy and in those taking certain medications (nicotinic acid, glucocorticoids, contraceptives, and diethylstilbestrol).
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Asymptomatic. The axilla and neck are the most commonly involved. In obese females who are hyperandrogenic, the vulva is the most commonly affected site.
Physical Examination
- •
Symmetrical hyperpigmented velvety plaques of the major flexures (axilla, groin), neck ( Fig. 3.2 ) , nipples, and vulva.

FIG. 3.2
Darkened, “dirty” appearing, thick skin of the neck with increased numbers of acrochordons that are frequently associated with acanthosis nigricans.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
Laboratory evaluation often reveals elevated glucose levels. Additional useful laboratory tests are thyroid-stimulating hormone (TSH) and follicle-stimulating hormone (FSH)/luteinizing hormone (LH).
 Differential Diagnosis
Differential Diagnosis
- •
Seborrheic keratosis
- •
Hyperpigmented nevus (Becker nevus), linear epidermal nevus
- •
Pemphigus vegetans
- •
Lichen simplex chronicus
- •
Confluent and reticulated papillomatosis
 Treatment
Treatment
First Line
- •
Therapy for underlying cause (weight loss in obese, discontinuation of offending drugs, treatment of malignancy if present)
Second Line
- •
Topical tretinoin, dermabrasion, ammonium lactate, carbon dioxide ablative laser
Third Line
- •
Oral contraceptives, cyproheptadine, oral isotretinoin
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The sudden onset of acanthosis nigricans should be followed by investigation for internal malignancy (e.g., upper endoscopy to rule out gastric cancer and computed tomography [CT] of abdomen and pelvis).
- •
Skin changes precede the malignancy diagnosis (usually neoplasm of abdominal cavity) in one third of cases.
- •
Consider drug use as a cause and review new medications (e.g., nicotinic acid, contraceptives, glucocorticoids).
2
Acne Keloidalis
 General Comments
General Comments
Definition
- •
Acne keloidalis is an idiopathic chronic inflammatory eruption of the nape of the neck occurring most commonly in dark-skinned men. It is also known as acne keloidalis nuchae, acne keloid, and folliculitis keloidalis. However, these are misnomers because there is no family history of keloids, no presence of keloids at other sites, and no development of keloid formation following excision. Despite the name, acne vulgaris is not associated.
Etiology
- •
Unknown. Close shaving of the hair, picking by patients, and chronic rubbing by collars have been suggested as possible contributing factors. This appears to represent a foreign body granulomatous reaction to hair, with subsequent scarring.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Onset is usually after puberty and before age 50.
- •
Clinical presentation consists of a follicular pustular eruption on the nape of the neck ( Fig. 3.3 ).

FIG. 3.3
A follicular-based papular and pustular reaction on the nape of the neck to curved hairs that re-enter the skin, producing a foreign body reaction. More advanced lesion may be associated with keloidal scarring.
Physical Examination
- •
Hard papules with hair emerging from the center are seen on the nape of neck and occipital scalp. Comedomes are not seen.
- •
Papules coalesce into sclerotic plaques.
- •
Pustules, crusting, and drainage may occur with secondary infections.
Diagnostic Tests
- •
Pustule swab for bacterial culture
- •
Deep biopsy
 Differential Diagnosis
Differential Diagnosis
- •
Folliculitis
- •
Simple ingrowing hairs (pili incurvatorum)
- •
Nevus sebaceus
- •
Traumatic causes of keloid
- •
Acne vulgaris
- •
Pseudofolliculitis
- •
Pediculosis capitis
 Treatment
Treatment
First Line
- •
Dissuade close cutting and allow hair to grow long in affected areas
- •
Limit mechanical irritation by a tight collar
- •
Encourage patient not to pick or squeeze lesions
- •
Topical antibiotics (clindamycin or erythromycin)
Second Line
- •
Oral doxycycline, tetracycline, or minocycline
Third Line
- •
Intralesional triamcinolone alone or following use of CO 2 laser vaporization
- •
Oral isotretinoin
- •
Surgery: punch biopsy for small papular lesions; surgical debulking for larger lesions. Any excision must be carried out to the subfollicular depth. If any of the hair follicle is left, recurrence is common.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Most cultures are sterile, but when a bacterium is found, it is usually Staphylococcus aureus.
3
Acne Vulgaris
 General Comments
General Comments
Definition
- •
Acne vulgaris is a chronic disorder of the pilosebaceous apparatus caused by abnormal desquamation of follicular epithelium leading to obstruction of the pilosebaceous canal, inflammation, and subsequent formation of comedones, papules, pustules, nodules, and scarring. Based on their appearance, the acne lesions can be divided into inflammatory (presence of papules, pustules, and nodules) and noninflammatory (open and closed comedones). For inflammatory acne, lesions can be classified as papulopustular, nodular, or both. The American Academy of Dermatology classification scheme for acne denotes the following three levels:
- 1.
Mild acne: characterized by the presence of comedones (noninflammatory lesions), few papules and pustules (generally <10), but no nodules.
- 2.
Moderate acne: presence of several to many papules and pustules (10–40) along with comedones (10–40). The presence of more than 40 papules and pustules along with larger, deeper, nodular, inflamed lesions (up to 5) denotes moderately severe acne.
- 3.
Severe acne: presence of numerous or extensive papules and pustules as well as many nodular lesions.
- 1.
Etiology
- •
Acne is a follicular disease, with the principal abnormality being comedo formation.
- •
Overactivity of the sebaceous glands and blockage in the ducts result in acne vulgaris. The obstruction leads to the formation of comedones, which can become inflamed because of overgrowth of Propionibacterium acnes. The condition can be exacerbated by environmental factors (hot, humid, tropical climate), medications (e.g., iodine in cough mixtures, hair greases), and industrial exposure to halogenated hydrocarbons. Mechanical or frictional forces can aggravate existing acne (e.g., excessive washing by some patients to help rid them of their blackheads or oiliness).
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Various stages of development and severity may be present concomitantly.
- •
Common distribution of acne is on the face, back, and upper chest.
Physical Examination
- •
Open comedones (blackheads), closed comedones (whiteheads) ( Fig. 3.4 )

FIG. 3.4
Erythematous nodulocystic acne vulgaris found on the back, often resulting in scarring.
- •
Inflammatory papules, pustules ( Fig. 3.5 ) , and ectatic pores

FIG. 3.5
Acne vulgaris of the face demonstrating pustular lesions. Other common areas include the chest and the back.
- •
Inflammatory and noninflammatory acneiform cysts ( Fig. 3.6 )

FIG. 3.6
Severe nodulocystic acne vulgaris on the back demonstrating evidence of early scarring.
- •
Greasiness (oily skin)
- •
Presence of scars from prior acne lesions ( Fig. 3.7 )

FIG. 3.7
Severe acne scarring with active pustules and small cystic lesions.
Diagnostic Tests
- •
Laboratory evaluation is generally not helpful.
- •
Patients who are candidates for therapy with isotretinoin (Accutane) should have baseline liver enzymes, cholesterol, and triglycerides checked because this medication may result in elevation of lipids and liver enzymes.
- •
Negative urine or serum pregnancy test must be obtained in female patients one month prior to, upon initiation of, and monthly when taking isotretinoin.
- •
In female patients, if hyperandrogenism is suspected, levels of dehydroepiandrosterone sulfate (DHEAS), testosterone (total and free), and androstenedione should be measured. Generally, for women with regular menstrual cycles, serum androgen measurements are not necessary.
 Differential Diagnosis
Differential Diagnosis
- •
Gram-negative folliculitis
- •
Staphylococcal pyoderma
- •
Acne rosacea
- •
Drug eruption
- •
Sebaceous hyperplasia
- •
Angiofibromas, basal cell carcinomas, osteoma cutis
- •
Occupational exposures to oils or grease
- •
Steroid acne
- •
Flat warts
 Treatment
Treatment
First Line
- •
Treatment generally varies with the type of lesions (comedones, papules, pustules, cystic lesions) and the severity of acne.
- •
Comedones (noninflammatory acne) can be treated with retinoids or retinoid analogs. Topical retinoids are comedolytic and normalize follicular keratinization. Commonly available agents are adapalene (0.1% gel or cream, applied once or twice daily), tazarotene (0.1% cream or gel applied daily), and tretinoin (0.1%, 0.5%, or 0.025% cream or gel applied once nightly). Tretinoin is inactivated by UV light and oxidized by benzoyl peroxide; therefore, it should only be applied at night and not used concomitantly with benzoyl peroxide. Tretinoin is pregnancy category C; tazarotene is pregnancy category X.
- •
Salicylic acid preparations (e.g., 2% wash) have keratolytic and antiinflammatory properties and are also useful in the treatment of comedones. Large open comedones (blackheads) may be expressed.
- •
Benzoyl peroxide gel (2.5% or 5%) may be added if the comedones become inflamed or form pustules. The most common adverse effects are dryness, erythema, and peeling.
- •
Topical antibiotics (erythromycin, clindamycin lotions or pads) can also be used in patients with significant inflammation. They reduce P. acnes in the pilosebaceous follicle and have some antiinflammatory effects. Combination products containing 5% benzoyl peroxide with topical antibiotics (3% erythromycin or 1% clindamycin) are highly effective in patients who have a mixture of comedonal and inflammatory acne lesions. Fixed-dose combinations of clindamycin phosphate 1.2% and tretinoin 0.025% are also available and are more effective than either product used alone; however, they are much more expensive than the individual generic components.
- •
Pustular acne can be treated with tretinoin and benzoyl peroxide gel applied on alternate evenings; drying agents (sulfa containing products) are also effective when used in combination with benzoyl peroxide.
- •
Azelaic acid, a bacteriostatic dicarboxylic acid, is used to normalize keratinization and reduce inflammation. It may be preferred in pregnancy (pregnancy category B).
Second Line
- •
Oral antibiotics (doxycycline 50–100 mg QD-BID or minocycline 50–100 mg QD-BID) are effective in patients with moderate to severe pustular acne. Erythromycin may also be used but has high rates of bacterial resistance. It is pregnancy category B.
- •
Patients with nodular cystic acne should be treated with systemic agents, including antibiotics (erythromycin, tetracycline, doxycycline, minocycline), isotretinoin, and/or oral contraceptives. Periodic intralesional triamcinolone injections are also effective for individual painful lesions. The possibility of endocrinopathy should be considered in patients responding poorly to therapy.
- •
Oral contraceptives reduce androgen levels and therefore sebum production. They represent a useful adjunctive therapy for some types of acne in women and adolescent girls but are not considered first-line therapy and should not be used as monotherapy for acne vulgaris. Commonly used agents are norgestimate/ethinyl estradiol and drospirenone/ethinyl estradiol.
- •
Spironolactone 100 to 200 mg/day can be administered to women only and has been shown to be particularly effective for adult-onset or “beard distribution” acne.
- •
Blue light can be used for treatment of moderate inflammatory acne vulgaris. Light in the violet/blue range can cause bacterial death by a photoreaction in which porphyrins react with oxygen to generate reactive oxygen species, which damage the cell membranes of P. acnes. Treatment usually consists of 15-minutes of exposure twice weekly for 4 weeks.
Third Line
- •
Isotretinoin is indicated for acne resistant to antibiotic therapy, severe acne, and scarring acne. Dosage is 0.5 to 1 mg/kg/day, and duration of therapy is generally 20 weeks for a cumulative dose 120 to 150 mg/kg. Before using this medication, patients should undergo baseline laboratory evaluation as described previously. Isotretinoin is absolutely contraindicated during pregnancy because of its teratogenicity. Patients, providers, pharmacies, and distributors of the drug must register in the iPLEDGE program prior to initiation of therapy.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Gram-negative folliculitis should be suspected if inflammatory acne worsens after several months of oral antibiotic therapy.
- •
Acne may worsen during the first 3 to 4 weeks of retinoid therapy before improving.
- •
Indications for systemic therapy of acne are painful deep papules or nodules, extensive lesions, active acne with severe scarring or hyperpigmentation, and patient morale.
- •
Erythromycin has a high incidence of early drug resistance.
- •
Doxycycline has a high incidence of sun sensitivity.
- •
Benzoyl peroxide will cause bleaching of fabrics.
- •
Spironolactone can produce menstrual irregularity.
- •
Tetracyclines are contraindicated in children and pregnant women.
4
Acrochordon
 General Comments
General Comments
Definition
- •
Acrochordons are benign outgrowths of the skin; they are also known as skin tags or fibroepithelial polyps.
Etiology
- •
Unknown. They are more prevalent in obese individuals and in women. Acrochordons may be associated with pregnancy and acanthosis nigricans.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
This condition is asymptomatic unless irritated by clothing, jewelry, or friction. It is most common in middle-aged and elderly persons.
Physical Examination
- •
Skin-colored or brown fleshy outgrowths ( Fig. 3.8 ) are usually seen on the side of the neck and around the axillae and groin.

FIG. 3.8
Acrochordons are soft, flesh-colored, pedunculated papules that are commonly located on the neck and axilla.
Diagnostic Tests
- •
None necessary. A shave/snip biopsy can be performed when diagnosis is unclear.
 Differential Diagnosis
Differential Diagnosis
- •
Wart
- •
Seborrheic keratosis
- •
Melanocytic nevus
- •
Dermatosis papulosa nigra
- •
Neurofibroma
- •
Melanoma
 Treatment
Treatment
First Line
- •
No treatment is needed.
- •
Scissor excision with or without local anesthesia may be done for cosmetic reasons or when the skin tag is irritated.
Second Line
- •
Electrodessication
Third Line
- •
Liquid nitrogen cryosurgery
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Skin tags in periorbital area are often confused with neoplastic skin lesions.
- •
Cryotherapy of a skin tag in dark-skinned patients may result in a white spot on the skin (postinflammatory hypopigmentation).
5
Actinic Cheilitis
 General Comments
General Comments
Definition
- •
Inflammatory reaction of the lips due to chronic and excessive sunlight exposure
Etiology
- •
Sunlight exposure
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Painful erosions usually involving the lower lip
Physical Examination
- •
Skin appears atrophic, scaly, fissured
- •
Erosions may be present ( Fig. 3.9 )

FIG. 3.9
Actinic cheilitis demonstrating thinned atrophic lip mucosa with scale, dyspigmentation, and an erosion.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
None usually needed
- •
Consider biopsy of any thickened or suspicious areas to exclude squamous cell carcinoma
 Differential Diagnosis
Differential Diagnosis
- •
Leukoplakia
- •
Squamous cell carcinoma
- •
Hereditary polymorphous light eruption
 Treatment
Treatment
First Line
- •
5% 5-FU cream
- •
Topical imiquimod
- •
Painful areas can be treated with 5% lidocaine ointment
- •
Cool compresses applied PRN several times/day may be useful if inflammation is intense
- •
Avoidance of further sun exposure and use of sunscreen-containing lip pomades when sun exposure occurs
- •
Topical steroids may be used for severe inflammation and pruritus
- •
Mupirocin ointment and oral antistaphylococcal antibiotics if secondary infection is present
Second Line
- •
Cryosurgery for localized lesions
- •
Photodynamic therapy
- •
Dermabrasion
- •
Electrodessication
- •
Fractionated or ablative laser
Third Line
- •
Vermilionectomy of lower lip in resistant cases
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Residual erythema and inflammation may persist for several weeks
6
Actinic Keratosis
 General Comments
General Comments
Definition
- •
Actinic keratosis is a common skin lesion usually presenting as multiple, erythematous or yellow-brown, dry, scaly lesions in the middle aged or elderly. It is also known as solar keratosis.
Etiology
- •
Sun exposure, ionizing radiation
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Typical lesions occur on sun-damaged skin of the face, neck, and dorsal aspect of hands ( Fig. 3.10 ) and forearms.

FIG. 3.10
Several scaly, adherent, yellow-brown lesions on the sun-exposed dorsum of the hand.
- •
Actinic keratosis is more common in males than females, especially in those with fair complexions who burn rather than tan following sun exposure.
Physical Examination
- •
Advanced lesions are characterized by a hard, spiky scale ( Fig. 3.11 ) and usually measure 1 cm in diameter or less. Early lesions manifest with redness and minimal scale. With progression, scales become thicker and yellow ( Fig. 3.12 ) and may resemble a small squamous cell carcinoma. On palpation, lesions are rough and gritty ( Fig. 3.13 ).

FIG. 3.11
An actinic keratosis located on this patient’s forehead is often best appreciated by its rough, tactile quality, similar to that of sandpaper.

FIG. 3.12
Scaly, raised lesion on sun-exposed back. Pain was elicited when scraping this lesion.

FIG. 3.13
Raised, rough, gritty actinic keratosis on the anterior thigh of an outdoorsman.
- •
The surrounding skin often shows additional features of sun damage, including atrophy, pigmentary changes, and telangiectasia.
- •
Classifications
- 1.
Hypertrophic AK with a cutaneous horn: Biopsy is necessary to distinguish the cutaneous horn from squamous cell carcinoma, seborrheic keratosis, verruca, trichilemmoma, and basal cell carcinoma. Hypertrophic AK has appearance of thick, scaling skin elevations.
- 2.
Lichenoid AK: Most commonly found on the torso and upper extremities. Must be distinguished from basal cell carcinoma due to pink and pearly characteristics.
- 3.
Proliferative AK: Often reappear after treatment and are characterized by a diameter larger than1 cm. The clinical differential diagnosis includes Bowen’s disease or SCC.
- 4.
Pigmented AK: Must be biopsied to distinguish from lentigo, maligna-type melanoma in situ, and solar lentigo.
- 5.
Actinic cheilitis: Characterized by red and sometimes abrasive lesions around the border of the lips.
- 1.
Diagnostic Tests
- •
Skin biopsy can be performed for recurrent lesions or when diagnosis is unclear and to rule out squamous cell or basal cell carcinoma.
 Differential Diagnosis
Differential Diagnosis
- •
Lentigo maligna (heavily pigmented variants may be clinically mistaken for this condition)
- •
Basal cell or squamous cell carcinoma
- •
Seborrheic keratosis
- •
Eczema
- •
Bowen’s disease (intraepithelial carcinoma)
- •
Wart
- •
Lichenoid keratosis
- •
Cutaneous lupus
 Treatment
Treatment
First Line
- •
Cryosurgery with liquid nitrogen
Second Line
- •
Topical 5-fluorouracil cream
- •
Topical imiquimod cream
- •
Topical diclofenac sodium gel
- •
Carbon dioxide laser
- •
Dermabrasion
- •
Curettage
Third Line
- •
Excision
- •
Photodynamic therapy with aminolevulinic acid and blue light
- •
Oral retinoids
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The risk of squamous cell carcinoma in patients with AK is 6% to 10%. Risk factors associated with increased risk of invasive, squamous cell carcinoma arising from actinic keratosis include: anatomic location (lip, ear, extremities); lesion characteristics (ulceration, induration, hyperkeratotic, proliferative, inflamed, bleeding, large surface area and depth); pigmentation (any rapid changes in presentation, presence of multiple lesions, evidence of greater ultraviolet [UV]-induced skin damage); presence of concomitant illness (lymphoma, leukemia); and use of concomitant medications (immunosuppressive agents, medications that increase sun sensitivity).
7
Alopecia Areata
 General Comments
General Comments
Definition
- •
Alopecia areata is an autoimmune alopecia characterized by lymphocytic inflammation of the hair bulb and discrete patches of hair loss on the scalp and/or eyebrows and eyelashes.
- •
Alopecia areata affects up to 1% of the population and is more common between 15 and 40 years of age.
Etiology
- •
Alopecia areata is driven by cellular immunity with autoantibody production.
- •
The increased frequency of this disorder in genetically related individuals suggests that there is a genetic link to the disease.
- •
Histologically, alopecia areata is characterized by normal numbers of follicular units and hair follicles, an increase in the number of catagen and telogen follicles, and a lymphocytic infiltrate affecting the bulbs of the anagen follicles.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Alopecia areata patients typically present with an abrupt development of patches of nonscarring alopecia in different patterns: circumscribed ( Fig. 3.14 ) , bandlike ( Fig. 3.15 ) , and reticular. The degree of involvement is highly variable and can range from very mild disease to diffuse hair loss that may affect the entire scalp (alopecia totalis).

FIG. 3.14
Round, well-demarcated area of hair loss is characteristic of alopecia areata.

FIG. 3.15
Alopecia areata presenting as an annular band of hair loss around the edge of the scalp. This pattern, called ophiasis, is associated with a poor prognosis.
Physical Examination
- •
Examination of the involved scalp reveals that, except for the absence of hair, the skin appears normal. There are patches of acute hair loss, typically 2 to 5 cm in diameter, with normal-appearing skin, black dots (cadaver hairs, point noir) from hair that breaks before reaching the skin’s surface, and occasional “exclamation point hairs,” which are evidence of hair breaking off as they are pushed from the follicle. Fingernails may show fine pitting.
Diagnostic Tests
- •
Laboratory evaluation is generally not helpful.
- •
Antinuclear antibody (ANA), TSH, and B 12 level should be considered in patients with a family history of the disease or other manifestations of autoimmune diseases.
- •
Ferritin level, TIBC/Serum iron, complete blood cell count (CBC) can be evaluated to rule out iron deficiency.
- •
RPR can be performed in selected patients to rule out cutaneous syphilis if history is suggestive of increased risk.
- •
On biopsy, lymphocytes surround the hair bulb and resemble a “swarm of bees.”
 Differential Diagnosis
Differential Diagnosis
- •
Androgenic alopecia
- •
Trichotillomania
- •
Secondary syphilis
- •
Telogen effluvium
- •
Tinea capitis
 Treatment
Treatment
First Line
- •
Topical, high-potency corticosteroids, such as clobetasol 0.05% ointment BID
Second Line
- •
Intralesional corticosteroids (triamcinolone acetonide, 5–10 mg/mL, raising a small bleb within the affected patch)
- •
Topical minoxidil
- •
Topical sensitizing agent or irritants (dithranol, diphencyprone)
Third Line
- •
Systemic corticosteroids for 4 to 6 weeks
- •
Systemic immune modulators and immunosuppressants (e.g., cyclosporine, methotrexate)
 Clinical Pearl(s)
Clinical Pearl(s)
- •
More than 50% of cases resolve spontaneously without treatment within 1 year.
- •
Ten percent evolve to chronic disease.
8
Amalgam Tattoo
 General Comments
General Comments
Definition
- •
Amalgam tattoo is characterized by painless, gray, bluish, black, or slate-colored macules that occur on the gingival/alveolar ridge or buccal mucosa.
Etiology
- •
Particles of amalgam restorations may be traumatically implanted into the mucosa by the dentist during placement or removal of a restoration, by the patient from bite injury, from leakage and disintegration of a restoration (or root canal filling material), or from a restoration falling into a tooth socket after extraction.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
This condition is asymptomatic, generally noted by dentist during routine dental examination.
Physical Examination
- •
Gray, bluish, black, or slate-colored macules can be seen on the gingival/alveolar ridge or buccal mucosa ( Fig. 3.16 ).

FIG. 3.16
Amalgam tattoo is a benign hyperpigmented area of the gingival mucosa adjacent to teeth with amalgam fillings.
(From Fitzpatrick J and Morelli J, Dermatology Secrets Plus , 5th Edition, Philadelphia, PA: Elsevier, 2016.)
Diagnostic Tests
- •
None necessary. Biopsy only when diagnosis is uncertain and atypical neoplasm is being considered.
 Differential Diagnosis
Differential Diagnosis
- •
Melanoma or mucosal melanosis
- •
Nevus
- •
Peutz-Jeghers
- •
Hemangioma or venous lake
 Treatment
Treatment
- •
No treatment is necessary.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The significance of this lesion is that its appearance can be mistaken for melanoma.
9
Anagen Effluvium
 General Comments
General Comments
Definition
- •
Anagen effluvium is nonscarring hair loss of the scalp following a toxic insult to growing hair (in anagen phase).
Etiology
- •
Cancer chemotherapy (e.g., inhibitors of mitosis) is the most common cause.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Hair loss occurs usually within 2 weeks of cancer chemotherapy.
Physical Examination
- •
Hair loss may be slight but is often extensive.
- •
Alopecia is noninflammatory and nonscarring ( Fig. 3.17 ).

FIG. 3.17
Anagen effluvium presenting as marked hair loss, thinning of hair shafts, and normal appearing scalp secondary to chemotherapy. Notice that numerous shed hairs are on the pillow.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
None necessary.
 Differential Diagnosis
Differential Diagnosis
- •
Diffuse alopecia areata
- •
Iron deficiency
- •
Malnutrition
- •
Androgenic alopecia
- •
Telogen effluvium
- •
Trichotillomania
- •
Traction alopecia
 Treatment
Treatment
- •
No treatment is necessary; the disorder is self-limited.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Be sympathetic, even if hair loss seems of a trivial amount. Reassure patient that hair loss is temporary.
10
Androgenic Alopecia
 General Comments
General Comments
Definition
- •
Androgenic alopecia is characterized by progressive patterned hair loss of the scalp due to androgens in genetically susceptible men and less commonly women.
Etiology
- •
Androgens are the main regulators of hair growth. After puberty, they promote transformation of vellus hair follicles, resulting in production of either tiny, nonpigmented hairs or large pigmented terminal hairs. However, androgens may also reverse this process, resulting in the gradual replacement of terminal hairs with vellus hairs and the onset of androgenetic alopecia. This phenomenon is the direct result of 5-alpha-reductase activity, which is found on the external root sheath and the hair bulb papilla. The enzyme converts testosterone into dihydrotestosterone, which has a great affinity for the androgen receptors in the hair follicle.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
In males, the condition usually starts early after puberty, mainly affecting the crown, vertex, frontal, central, and temporal areas of the scalp (Hamilton’s male pattern). There is usually no involvement of the occipital and lower parietal regions.
- •
In females, the hair loss is patterned and characterized by progressive thinning over the frontal/parietal scalp, retention of the frontal hairline (Ludwig’s female pattern), and the presence of miniaturized hairs. The hair loss often starts around the onset of menopause.
Physical Examination
- •
In men, androgenetic alopecia presents as noninflammatory, nonscarring alopecia in defined patterns often resulting in a smooth, shiny scalp devoid of hair follicles ( Fig. 3.18 , Fig. 3.19 ).

FIG. 3.18
Frontal recession of hairline typical of early androgenic alopecia.

FIG. 3.19
Progressive androgenic alopecia with loss of hair extending from frontal to vertex regions.
- •
In women, androgenic alopecia is characterized by a noninflammatory, nonscarring alopecia that is characterized by diffuse thinning of the hair on the scalp ( Fig. 3.20 ).

FIG. 3.20
Diffuse hair loss in female androgenic alopecia.
Diagnostic Tests
- •
Ferritin and iron studies, TSH, serum testosterone and dihydrotestosterone levels, ANA
- •
Scalp biopsy if diagnosis is unclear
 Differential Diagnosis
Differential Diagnosis
- •
Iron deficiency
- •
Malnutrition
- •
Hypothyroidism
- •
Telogen effluvium
- •
Trichotillomania
- •
Traction alopecia
- •
Alopecia areata
- •
Anagen effluvium
- •
Tinea capitis
 Treatment
Treatment
First Line
- •
Topical minoxidil 5%
- •
Finasteride 1 mg PO QD (men only). Dutasteride (off-label) has been shown to be superior to finasteride in a randomized trial but requires higher doses than that used for BPH.
Second Line
- •
Hair transplant from occipital scalp
- •
Hair weaves, wigs
Third Line
- •
Spironolactone 100 mg BID (women only)
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Androgenetic alopecia affects more than 50% of males over age 50 and 40% of females by age 70. There is often a familial history of baldness.
- •
At least 6 months are needed to assess a response to minoxidil and nearly 12 months for finasteride.
11
Angioedema
 General Comments
General Comments
Definition
- •
Mucocutaneous swelling caused by the release of vasoactive mediators. The hivelike swelling involves the deep layers of the dermis and the subcutaneous tissue.
- •
Angioedema is classified as acquired (allergic or idiopathic) or hereditary.
Etiology
- •
Angioedema is caused by mast cell activation and degranulation with release of vasoactive mediators (e.g., histamine, serotonin, bradykinins) resulting in postcapillary venule inflammation, vascular leakage, and edema in the deep layers of the dermis and subcutaneous tissue.
- •
Hereditary angioedema is an autosomal dominant disease caused by a deficiency of C1 esterase inhibitor (C1-INH). C1-INH is a protease inhibitor that is normally present in high concentrations in the plasma.
- •
Other causes of angioedema include: infection (e.g., herpes simplex, hepatitis B, and coxsackie A and B viruses; Streptococcus, Candida, Ascaris, and Strongyloides bacteria); insect bites and stings, stress, physical factors (e.g., cold, exercise, pressure, and vibration); connective tissue diseases (e.g., systemic lupus erythematosus (SLE); Henoch-Schönlein purpura); and idiopathic causes. Angiotensin-converting enzyme (ACE) inhibitors can increase kinin activity and lead to angioedema.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
This condition is characterized by poorly demarcated, nonpruritic, burninglike edema, often involving the eyelids, lips ( Fig. 3.21 ) , tongue, and extremities, which resolves slowly.
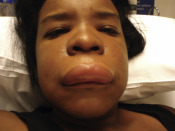
FIG. 3.21
Angioedema is a hivelike swelling of the mucosa and skin that can involve the tongue, lips, or larynx and, at times, can encroach on the airway.
- •
It can involve the upper airway, causing respiratory distress, and can involve the gastrointestinal (GI) tract, leading to cyclic abdominal pain.
Physical Examination
- •
Edema of the subcutaneous tissues, often resulting in temporary disfigurement, is seen.
Diagnostic Tests
- •
A detailed history and physical examination usually establish the diagnosis of angioedema.
- •
Extensive laboratory testing is of limited value.
- •
CBC, erythrocyte sedimentation rate (ESR), and urinalysis are sometimes helpful as part of the initial evaluation.
- •
Stool testing can be done to detect ova and parasites.
- •
Serology testing can be performed.
- •
C4 levels are reduced in acquired and hereditary angioedema (occurring without urticaria). If C4 levels are low, C1-INH levels and activity should be obtained.
- •
Skin and radioallergosorbent (RAST) testing may be done if food allergies are suspected.
- •
Skin biopsy is often performed in patients with chronic angioedema refractory to corticosteroid treatment.
 Differential Diagnosis
Differential Diagnosis
- •
Cellulitis
- •
Arthropod bite
- •
Hypothyroidism
- •
Contact dermatitis
- •
Atopic dermatitis
- •
Mastocytosis
- •
Granulomatous cheilitis
- •
Bullous pemphigoid
- •
Urticaria pigmentosa
- •
Anaphylaxis
- •
Erythema multiforme
- •
Epiglottitis
- •
Peritonsillar abscess
 Treatment
Treatment
First Line
- •
Acute life-threatening angioedema involving the larynx is treated with subcutaneous epinephrine, IV diphenhydramine, IV ranitidine or cimetidine, and systemic steroids.
- •
The mainstay therapy in angioedema is H1 antihistamines.
- •
H2 antihistamines can be added to H1 antihistamines.
Second Line
- •
Corticosteroids are rarely required for symptomatic relief of acute angioedema and are used more often in chronic angioedema. Prednisone 1 mg/kg/day is generally given for 5 days and then tapered over a period of weeks.
Third Line
- •
Tricyclic antidepressants (Doxepin 25–50 mg QD) can be used.
- •
Androgens (danazol, stanozolol, oxandrolone, methyltestosterone) are used for the treatment of hereditary angioedema that does not respond to antihistamines or corticosteroids. C1-INH replacement therapy (cinryze IV infusions given twice weekly; icatibant [firazyr] or ecallantide [kalbitor]) is available in some centers.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
ACE inhibitors can cause angioedema months after initiation.
- •
Acquired angioedema is usually associated with other diseases, most commonly B-cell lymphoproliferative disorders, but may also result from the formation of autoantibodies directed against C1 inhibitor protein.
12
Angiokeratoma of Scrotum
 General Comments
General Comments
Definition
- •
Dilatations of the superficial dermal blood vessels in the scrotum
Etiology
- •
Increased venous pressure (i.e., venous insufficiency, hemorrhoids)
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Onset generally after age 20
- •
Trauma/abrasion can result in significant bleeding
Physical Examination
- •
Multiple 1 to 3 mm red to purple papules consisting of blood vessels in the skin of the scrotum ( Fig. 3.22 )

FIG. 3.22
Angiokeratoma of Fordyce presenting as numerous small vascular papules on the scrotum.
(Fitzsimons Army Medical Center Collection)
- •
Diffuse redness of involved area may be present
Diagnostic Tests
- •
None needed
 Differential Diagnosis
Differential Diagnosis
- •
Trauma
- •
Cherry angiomas
 Treatment
Treatment
First Line
- •
Simple scissor excision
Second Line
- •
Electrodessication and curettage
Third Line
- •
Laser ablation
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Treatment is generally not necessary; reassurance is sufficient in most cases
13
Angioma (Cherry Angioma)
 General Comments
General Comments
Definition
- •
Cherry angiomas (also known as Campbell de Morgan spots and senile angiomas) are very common tiny red papules on the trunk ( Fig. 3.23 ) and upper limbs of the middle aged and elderly.

FIG. 3.23
Example of numerous red to violaceous papules found primarily on the trunk and upper extremities.
Etiology
- •
Etiology is unknown. Histologically, a cherry angioma is a small polypoid lesion with an epidermal collarette and multiple lobules of dilated and congested capillaries in the papillary dermis.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Asymptomatic lesions appear most often in middle age and increase in size and number with age.
Physical Examination
- •
Smooth, cherry red lesions with shape variable from dome to polypoid papules ( Fig. 3.24 ).

FIG. 3.24
Raised, dark, violaceous angiomas such as this can sometimes be confused with nodular melanomas.
Diagnostic Tests
- •
None necessary. Skin biopsy is done only when the diagnosis is unclear.
 Differential Diagnosis
Differential Diagnosis
- •
Petechiae
- •
Telangiectasia
- •
Bacillary angiomatosis
- •
Melanoma
- •
Benign pigmented purpura
- •
Insect bite
- •
Pyogenic granuloma
- •
Angiokeratoma
 Treatment
Treatment
First Line
- •
Observation only
Second Line
- •
Electrodesiccation and curettage
Third Line
- •
Liquid nitrogen therapy
- •
Laser surgery
 Clinical Pearl(s)
Clinical Pearl(s)
- •
There is no known association with malignancy.
14
Angular Cheilitis (Perleche)
 General Comments
General Comments
Definition
- •
Angular cheilitis refers to inflammation of one or both of the corners of the mouth.
Etiology
- •
Most unilateral lesions are due to trauma (mechanical irritation from dental flossing, excessive salivation, lip licking, mouth breathing, braces, tongue studs). Bilateral lesions are often due to infection (most often Candida albicans or S. aureus ) or nutritional deficiencies (iron deficiency, riboflavin deficiency).
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Burning and discomfort are felt at the corners of the mouth.
- •
Symptoms are made worse by attempts of patients to moisten the area by licking it.
Physical Examination
- •
Erythema, fissures, scales, and crust may be present at the angles of the mouth ( Fig. 3.25 ).

FIG. 3.25
Angular cheilitis in the elderly is characterized by moist, overlapping skin at the angles of the mouth, which often becomes inflamed and fissured as a result of nocturnal drooling of saliva.
(Fitzsimons Army Medical Center Collection)
- •
Area of fissure may be surrounded by papules and pustules.
Diagnostic Tests
- •
Culture for candidiasis and bacteria or potassium hydroxide preparation (KOH) preparation for fungal elements ( Fig. 3.26 ).

FIG. 3.26
Positive KOH for candidiasis demonstrating an admixture of thin-walled yeast and pseudohyphae.
(Fitzsimons Army Medical Center Collection)
- •
Human immunodeficiency virus (HIV) testing in patients with risk factors
- •
CBC, BMP, iron, folate, and vitamin B 12
 Differential Diagnosis
Differential Diagnosis
- •
Impetigo
- •
Contact dermatitis (lip balms, mouthwash, toothpaste)
- •
Lip smacking/lip licking dermatitis
 Treatment
Treatment
First Line
- •
Elimination of risk factors (e.g., poorly fitting dentures, repeated attempts by patients to lick and moisten area)
- •
Topical miconazole or nystatin cream after meals and at bedtime
- •
Protective lip balms or ointments
Second Line
- •
Topical mupirocin if microbiology swabs reveal Staphylococcus colonization
Third Line
- •
Injection of collagen in the commissures when mechanical factors are causative
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Angular cheilitis is often present in HIV-positive patients (more than 10% may have localized candidiasis).
15
Antiphospholipid Syndrome
 General Comments
General Comments
Definition
- •
Antiphospholipid antibody syndrome (APS) is characterized by arterial or venous thrombosis and/or pregnancy loss and the presence of antiphospholipid antibodies (aPL). aPL are antibodies directed against either phospholipids or proteins bound to anionic phospholipids. Three types of aPL have been characterized:
- 1.
Lupus anticoagulants
- 2.
Anticardiolipin antibodies
- 3.
Anti-β2 glycoprotein 1 antibodies
- 1.
Etiology
- •
APS is an autoimmune disorder.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
The syndrome is referred to as primary APS when it occurs alone and as secondary APS when in association with systemic lupus erythematosus (SLE), other rheumatic disorders, or certain infections or medications. APS can affect all organ systems and includes venous and arterial thrombosis, recurrent fetal losses, and thrombocytopenia.
Physical Examination
- •
Cutaneous: livedo reticularis ( Fig. 3.27 ) , cutaneous necrosis, skin ulcerations ( Fig. 3.28 ), gangrene of digits

FIG. 3.27
Bluish, netlike, reticular pattern of discoloration involving the lower extremities associated with circulating antiphospholipid antibodies in this patient.

FIG. 3.28
Lacelike appearance of the skin with blue mottling in this patient with an ulcer due to infarction.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
Diagnostic criteria for APS include at least one clinical criterion and at least one laboratory criterion.
Clinical
- •
Venous, arterial, or small vessel thrombosis or
- •
Morbidity with pregnancy, defined as:
- •
Fetal death at more than 10 weeks gestation or
- •
More than one premature births before 34 weeks gestation secondary to eclampsia, preeclampsia, or severe placental insufficiency or
- •
More than three unexplained consecutive spontaneous abortions at less than 10 weeks gestation
- •
Laboratory
- •
IgG and/or IgM anticardiolipin antibody in medium or high titers or
- •
Lupus anticoagulant activity found or
- •
Anti-β2 glycoprotein-1 IgM or IgG antibodies found on more than two occasions, at least 12 weeks apart
Laboratory Tests
- •
Abnormal tests include:
- •
False-positive test for syphilis (RPR/VDRL)
- •
Lupus anticoagulant activity, demonstrated by prolongation of activated partial thromboplastin time (aPTT) that does not correct with 1:1 mixing study
- •
Presence of anticardiolipin antibodies (ELISA for anticardiolipin is most sensitive and specific test [> 80%])
- •
Presence of anti-β2 glycoprotein 1 antibody
- •
 Differential Diagnosis
Differential Diagnosis
- •
Other hypercoagulable states (inherited or acquired)
- •
Inherited: antithrombin (ATIII) deficiencies, protein C or S deficiencies, factor V Leiden, prothrombin gene mutation
- •
Acquired: heparin-induced thrombocytopenia, myeloproliferative syndromes, cancer, hyperviscosity
- •
Nephrotic syndrome
- •
Cholesterol emboli
- •
Thrombotic thrombocytopenic purpura
- •
Hyperhomocysteinemia
- •
Atherosclerotic cardiovascular disease
 Treatment
Treatment
First Line
- •
For positive aPL and venous thrombosis:
- •
Initial anticoagulation with heparin, then lifelong warfarin treatment (international normalized ratio [INR] 2.0–3.0)
- •
- •
For positive aPL with arterial thrombosis:
- •
Cerebral arterial thrombosis: acetylsalicylic acid (ASA) 325 mg daily or warfarin therapy (INR 1.4–2.8)
- •
Noncerebral arterial thrombosis: warfarin therapy (INR 2.0–3.0)
- •
- •
For pregnant women with previously diagnosed APS:
- •
Warfarin should be discontinued secondary to its teratogenic effects.
- •
ASA, 81 mg, and heparin subcutaneously (SC) should be administered to partial prothromboplastin time PTT of 1.5 to 2 times control value.
- •
Intravenous immunoglobulin (IVIG) and prednisone have also been used with success if aspirin and heparin fail.
- •
- •
For pregnant women with (+) aPL antibodies and a history of fewer than three spontaneous abortions:
- •
ASA 81 mg should be taken daily at conception and subcutaneous heparin 5000 to 10,000 IU q12h at time of documented viable intrauterine pregnancy (approximately 7 weeks gestation) until 6 weeks postpartum.
- •
A midinterval PTT should be checked and should be normal or similar to baseline before therapy.
- •
- •
For pregnant women with (+) aPL antibodies without a history of deep vein thrombosis (DVT) or pregnancy loss:
- •
Consider low-dose subcutaneous heparin, ASA 81 mg, or surveillance.
- •
- •
For catastrophic APS:
- •
The highest survival rate is achieved with the combination of anticoagulation, corticosteroids, and IVIG or plasma exchange.
- •
Case reports describe Rituximab and the monoclonal antibody eculizumab are effective for patients with life-threatening thrombosis refractory to anticoagulation.
- •
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Laboratory testing of anticardiolipin and LA antibodies indicated in:
- •
Patients with underlying SLE or collagen–vascular disease with thrombosis
- •
Patients with recurrent, familial, or juvenile DVT or thrombosis in an unusual location (mesenteric or cerebral)
- •
Possibly in patients with lupus or lupuslike disorders in high-risk situations (e.g., surgery, prolonged immobilization, pregnancy)
- •
16
Aphthous Stomatitis (Canker Sores)
 General Comments
General Comments
Definition
- •
Stomatitis is inflammation involving the oral mucous membranes. Aphthous stomatitis is a chronic, painful, relapsing ulcerative condition of the nonkeratinized mucosa ( Fig. 3.29 )

FIG. 3.29
Aphthous ulcers are most commonly found on the mucous membranes of the oropharynx and appear as shallow, punched-out erosions.
Etiology
- •
Unknown
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
There are three variants: minor, major, and herpetiform.
- •
Ulcers of the minor form (the most common variant) are smaller than 1 cm, last 7 to 14 days, and heal without scarring.
- •
Ulcers of the major form are more common in children and adolescents, usually larger than 1 cm, last many weeks, and heal with scarring ( Fig. 3.30 ).

FIG. 3.30
Large aphthous ulcer (Sutton’s ulcer) on the tongue of a child.
(William Weston Collection)
- •
Ulcers of the herpetiform variety occur in small crops of 10 to 100 ulcers in any one episode.
Physical Examination
- •
Painful, grayish white, oval ulcerations with red margins are seen inside the mouth.
Diagnostic Tests
- •
CBC
- •
Vitamin B 1 , B 2 , B 6 , and B 12 level; red blood cell (RBC) folate level
- •
Herpes simplex virus polymerase chain reaction (PCR)
 Differential Diagnosis
Differential Diagnosis
White Lesions
- •
Candidiasis (thrush)
- •
Leukoedema: filmy, opalescent-appearing mucosa that can be reverted to normal appearance by stretching; benign condition
- •
White sponge nevus: thick, white, corrugated folds involving buccal mucosa; appears in childhood as an autosomal dominant trait; benign condition
- •
Darier’s disease (keratosis follicularis): white papules on the gingivae, alveolar mucosa, and dorsal tongue; skin lesions also present (erythematous papules); inherited as an autosomal dominant trait
- •
Chemical injury: white sloughing mucosa
- •
Nicotine stomatitis: whitened palate with red papules
- •
Lichen planus: linear, reticular, slightly raised striae on buccal mucosa; skin is involved by pruritic, violaceous papules on forearms and inner thighs
- •
Discoid lupus erythematosus: lesion resembles lichen planus
- •
Leukoplakia: white lesions that cannot be scraped off; 20% are premalignant epithelial dysplasia or squamous cell carcinoma
- •
Hairy leukoplakia: shaggy white surface that cannot be wiped off; often seen in HIV infection; caused by Epstein-Barr virus (EBV)
Red Lesions
- •
Candidiasis: may present with red instead of more frequent white lesion (see “ White Lesions ”); median, rhomboid glossitis is chronic variant
- •
Benign migratory glossitis (geographic tongue): area of atrophic, depapillated mucosa surrounded by a keratotic border; benign lesion, no treatment required
- •
Hemangiomas
- •
Histoplasmosis: ill-defined irregular patch with a granulomatous surface, sometimes ulcerated
- •
Allergy
- •
Anemia: atrophic, reddened glossal mucosa seen with pernicious anemia
- •
Erythroplakia: red patch usually caused by epithelial dysplasia or squamous cell carcinoma
- •
Burning tongue (glossopyrosis): normal examination; sometimes associated with denture trauma, anemia, diabetes, vitamin B 12 deficiency, psychogenic problems
Dark Lesions (Brown, Blue, Black)
- •
Coated tongue: accumulation of keratin; harmless condition that can be treated by scraping
- •
Melanotic lesions: freckles, lentigines, lentigo, melanoma, Peutz-Jeghers syndrome, Addison’s disease
- •
Varices
- •
Kaposi’s sarcoma: red or purple macules that enlarge to form tumors; seen in patients with acquired immunodeficiency syndrome (AIDS)
Raised Lesions
- •
Papilloma
- •
Verruca vulgaris
- •
Condyloma acuminatum
- •
Fibroma
- •
Epulis
- •
Pyogenic granuloma
- •
Mucocele
- •
Retention cyst
Blisters
- •
Primary herpetic gingivostomatitis
- •
Pemphigus and pemphigoid
- •
Hand-foot-and-mouth disease: caused by coxsackievirus group A
- •
Erythema multiforme
- •
Herpangina: caused by echovirus
- •
Traumatic ulcer
- •
Primary syphilis
- •
Perlèche (or angular cheilitis)
- •
Recurrent aphthous stomatitis (canker sores)
- •
Behçet’s syndrome (aphthous ulcers, uveitis, genital ulcerations, arthritis, and aseptic meningitis)
- •
Reiter’s syndrome (conjunctivitis, urethritis, and arthritis with occasional oral ulcerations)
 Treatment
Treatment
First Line
- •
Topical corticosteroids
- •
Antimicrobial mouth rinses
- •
Intralesional corticosteroids
- •
Viscous lidocaine or other topical anesthetic
Second Line
- •
Oral corticosteroids (prednisone taper)
- •
Colchicine
- •
Sucralfate suspension
Third Line
- •
Pentoxifylline
- •
Oral acyclovir
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Some conditions often associated with the minor variant include Behçet’s syndrome, inflammatory bowel disease, and gluten sensitivity.
17
Atopic Dermatitis (Atopic Eczema)
 General Comments
General Comments
Definition
- •
Atopic dermatitis is a genetically determined eczematous eruption that is pruritic, symmetric, and associated with personal family history of allergic manifestations (atopy).
- •
Diagnosis is based on the presence of three of the following major features and three minor features.
Major Features
- •
Pruritus
- •
Personal or family history of atopy: asthma, allergic rhinitis, atopic dermatitis
- •
Facial and extensor involvement in infants and children
- •
Flexural lichenification in adults
Minor Features
- •
Elevated IgE
- •
Eczema-perifollicular accentuation
- •
Recurrent conjunctivitis
- •
Ichthyosis
- •
Nipple dermatitis
- •
Wool intolerance
- •
Cutaneous S. aureus infections or herpes simplex infections
- •
Food intolerance
- •
Hand dermatitis (nonallergic irritant)
- •
Facial pallor, facial erythema
- •
Cheilitis
- •
White dermographism
- •
Early age of onset (after 2 months of age)
Etiology
- •
Unknown. Elevated T-lymphocyte activation, defective cell immunity, and B-cell IgE overproduction may play a significant role.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
There are no specific cutaneous signs for atopic dermatitis, and a wide spectrum of presentations is possible, ranging from minimal flexural eczema to erythroderma.
- •
Inflammation in the flexural areas and lichenified skin is a very common presentation in children.
Physical Examination
- •
The primary lesions are a result of scratching caused by severe and chronic pruritus (“the itch that rashes”). The repeated scratching modifies the skin surface, producing lichenification, dry and scaly skin, and redness.
- •
In children, red scaling plaques are often confined to the cheeks ( Fig. 3.31 ) and the perioral and perinasal areas.

FIG. 3.31
Dermatitis on the face of an infant, a characteristic site for atopic dermatitis in infants and young children.
(William Weston Collection)
- •
Lesions are typically found on the neck, face, upper trunk, and bends of elbows ( Fig. 3.32 ) and knees (symmetric on flexural surfaces of extremities).

FIG. 3.32
Erythema with secondary excoriations in the antecubital fossa of an adolescent with atopic dermatitis.
(Fitzsimons Army Medical Center Collection)
- •
There is dryness, thickening of the involved areas, discoloration, blistering, and oozing.
- •
Papular lesions are frequently found in the antecubital and popliteal fossae.
- •
Constant scratching may result in areas of hypopigmentation or hyperpigmentation ( Fig. 3.33 ) (more common in dark-skinned patients).

FIG. 3.33
Chronic atopic dermatitis with darker skin demonstrating both hypopigmentation and hyperpigmentation.
(Fitzsimons Army Medical Center Collection)
- •
In adults, redness and scaling in the dorsal aspect of the hands or around the fingers is the most common manifestation of atopic dermatitis; oozing and crusting may be present ( Fig. 3.34 ).

FIG. 3.34
Chronic atopic dermatitis in the hand of an adult woman demonstrating dermatitis, loss of the cuticle, and mild nail dystrophy.
(Fitzsimons Army Medical Center Collection)
- •
Secondary skin infections may be present ( S. aureus, dermatophytosis, herpes simplex).
Diagnostic Tests
- •
Laboratory tests are generally not helpful.
- •
Elevated IgE levels are found in 80% to 90% of patients with atopic dermatitis.
- •
Blood eosinophilia correlates with disease severity.
 Differential Diagnosis
Differential Diagnosis
- •
Scabies
- •
Psoriasis
- •
Dermatitis herpetiform
- •
Contact dermatitis
- •
Photosensitivity
- •
Seborrheic dermatitis
- •
Candidiasis
- •
Lichen simplex chronicus
 Treatment
Treatment
First Line
- •
Avoidance of triggering factors:
- •
Sudden temperature changes, sweating, low humidity in the winter
- •
Contact with irritating substance (e.g., wool, cosmetics, some soaps and detergents, tobacco)
- •
Stressful situations
- •
Allergens and dust
- •
Excessive hand washing
- •
- •
Clip nails to decrease abrasion of skin.
- •
Emollients can be used to prevent dryness. Severely affected skin can be optimally hydrated by occlusion in addition to application of emollients.
- •
Low-to medium-potency topical steroids BID to affected areas.
- •
Oral antihistamines (nonsedating qAM, sedating qHS).
Second Line
- •
Crisaborole 2% ointment (eucrisa) is a phosphodiesterase type-4 (PDE 4 ) inhibitor effective topical treatment for mild to moderate atopic dermatitis in patients ≥2 years old. Cost is a major limiting factor. It is administered by subcutaneous injection.
- •
Topical immunomodulators pimecrolimus and tacrolimus are nonsteroid antiinflammatories that may be helpful in some patients.
Third Line
- •
Phototherapy (Narrowband UVB)
- •
Systemic immunomodulators and antiinflammatories (methotrexate, cyclosporine, mycophenolate mofetil)
- •
Systemic biologic therapy
- •
Dupilumab (dupixent) is a human monoclonal antibody FDA-approved for treatment of adults with moderate to severe atopic dermatitis that has not responded to topical therapies.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The highest incidence is among children (5%–10%). More than 50% of children with generalized atopic dermatitis develop asthma and allergic rhinitis by age 13 years.
- •
Systemic corticosteroids should be avoided for flares of atopic dermatitis. Long-term side effects and rebound flares of severe dermatitis after discontinuation are common.
18
Atypical Mole (Dysplastic Nevus)
 General Comments
General Comments
Definition
- •
Atypical moles are also commonly known as dysplastic nevi, atypical melanocytic nevi, Clark’s nevi, and dysplastic moles.
- •
The term refers to nevi that demonstrate atypical color, shape, and size.
Etiology
- •
They can occur sporadically in 5% to 10% of the general population or as a familial syndrome (autosomal dominant trait with incomplete penetrance).
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Atypical moles may be present on the scalp but are most commonly found on the trunk ( Fig. 3.35 ) and upper extremities.

FIG. 3.35
Atypical nevi located on the back of a patient with sporadic dysplastic nevus syndrome.
(John Aeling Collection)
- •
They may continue appearing into adulthood.
Physical Examination
- •
Diameter greater than 6 mm
- •
Irregular edge ( Fig. 3.36 ) that can fade into the surrounding skin

FIG. 3.36
Atypical nevus larger than 6 mm with irregular borders and two shades of brown. This lesion was biopsied and histologically was a mildly atypical nevus.
(John Aeling Collection)
- •
Asymmetrical shape with variations in pigmentation ( Fig. 3.37 )

FIG. 3.37
Atypical nevus larger than 6 mm with loss of symmetry, irregular borders, and variegation of color with an area that is focally red. This lesion was biopsied and histologically was a severely atypical nevus.
(Joanna Burch Collection)
- •
Irregular surface, raised areas
Diagnostic Tests
- •
Diagnostic biopsy if suspecting melanoma
- •
Ophthalmologic examination (increased risk of intraocular melanoma) and examination of other family members when suspecting familial syndrome
 Differential Diagnosis
Differential Diagnosis
- •
Melanoma
- •
Lentigo maligna
- •
Compound nevus
- •
Flat wart
- •
Seborrheic keratosis
 Treatment
Treatment
- •
Periodic follow up every 6 to 12 months with clinical examination and photographs
- •
Removal and histopathologic examination of any lesion with documented change
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The risk of melanoma is very high in patients with atypical mole syndrome or with a sibling or parent with a history of melanoma.
- •
The presence of atypically appearing nevi in sun-protected areas in children may be a clue to the presence of the atypical nevus/mole syndrome.
19
Bacillary Angiomatosis
 General Comments
General Comments
Definition
- •
Bacillary angiomatosis is a vasoproliferative lesion that may be readily confused with pyogenic granuloma or Kaposi’s sarcoma and is seen predominantly (but not exclusively) in the skin.
Etiology
- •
The condition may be caused either by Bartonella henselae (the organism responsible for cat scratch disease) or, less commonly, by Bartonella Quintana (the cause of trench fever).
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Patients may have systemic manifestations, including fever and malaise.
- •
Lesions have also been described in the bones, soft tissues, liver, lymph nodes, and spleen.
Physical Examination
- •
Patients present with widespread, numerous, blood-red, smooth, superficial papules and skin-colored or dusky subcutaneous nodules ( Fig. 3.38 )

FIG. 3.38
Bacillary angiomatosis: the primary lesions clinically resemble vascular lesion.
(Courtesy N. C. Dlova, MD, Nelson R. Mandela School of Medicine, University of KwaZulu-Natal, South Africa. From McKee PH, Calonje JE, Granter SR. Pathology of the skin , 3rd ed. St. Louis, MO: Mosby, 2005, Fig. 17.130.)
- •
Hepatosplenomegaly and lymphadenopathy are also seen.
Diagnostic Tests
- •
Biopsy and Warthin-Starry stain/electron microscopy, PCR of biopsy material, serology, indirect fluorescence assay (IFA), prolonged culture of blood and biopsy tissue
- •
Complete blood cell count (CBC), HIV, alanine aminotransferase (ALT), CD4 lymphocyte count
 Differential Diagnosis
Differential Diagnosis
- •
Pyogenic granuloma
- •
Angiokeratoma
- •
Kaposi’s sarcoma
- •
Hemangioma
- •
Melanoma
- •
Abscess
 Treatment
Treatment
First Line
- •
Clarithromycin, azithromycin, or ciprofloxacin
Second Line
- •
Erythromycin, doxycycline, rifampin
Third Line
- •
Gentamycin
- •
Third- and fourth-generation cephalosporins
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Although bacillary angiomatosis was originally thought to be a disease specific to AIDS, it has also been described in other immunocompromised states and even in apparently normal individuals.
20
Basal Cell Carcinoma
 General Comments
General Comments
Definition
- •
Basal cell carcinoma (BCC) is a malignant tumor of the skin arising from basal cells of the lower epidermis and adnexal structures. It may be classified as one of six types (nodular, superficial, pigmented, cystic, sclerosing or morpheaform, and nevoid). The most common type is nodular (21%); the least common is morpheaform (1%); a mixed pattern is present in approximately 40% of cases. Basal cell carcinoma advances by direct expansion and destroys normal tissue.
Etiology
- •
Risk factors include fair skin, increased sun exposure, use of tanning salons with ultraviolet A or B radiation, history of irradiation (e.g., Hodgkin’s disease), personal or family history of skin cancer, and impaired immune system.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Most common malignant cutaneous neoplasm:
- •
85% appear on the head and neck region
- •
Most common site is the nose (30%)
- •
Increased incidence with age
- •
Increased incidence in men
- •
Physical Examination
- •
Examination varies with the histologic type:
- •
Nodular ( Fig. 3.39 ) : Dome-shaped, painless lesion may become multilobular and frequently ulcerate (rodent ulcer) ( Fig. 3.40 ). Prominent telangiectatic vessels are noted on the surface. The border is translucent, elevated, and pearly white. Some nodular basal cell carcinomas may contain pigmentation ( Fig. 3.41 ) , giving an appearance similar to a melanoma, or they may be eroded on the surface and even resemble a pyogenic granuloma ( Fig. 3.42 ).

FIG. 3.39
Nodular basal cell carcinoma presenting as a pearly papule with well-demarcated borders and overlying telangiectasia.
(Fitzsimons Army Medical Center Collection)

FIG. 3.40
Nodulo-ulcerative basal cell carcinoma of the left ear.
(Fitzsimons Army Medical Center Collection)

FIG. 3.41
Pigmented basal cell carcinoma in the background of a patient with marked solar damage.

FIG. 3.42
Ulcerated exophytic basal cell carcinoma of the inguinal area. Although most basal carcinomas occur in sun-exposed sites, they can also occur in covered sites.
(William Weston Collection)
- •
Superficial: Circumscribed scaling, often black appearance with a thin, raised, pearly white border ( Fig. 3.43 ). Crust and erosions may be present. These are found most commonly on the trunk and extremities.

FIG. 3.43
Superficial spreading basal cell carcinoma demonstrating a horizontal growth pattern.
(Fitzsimons Army Medical Center Collection)
- •
Morpheaform: Flat or slightly raised and yellowish or white (similar to localized scleroderma), these appear similar to scars. The surface has a waxy consistency.
- •
Diagnostic Tests
- •
Biopsy to confirm diagnosis
 Differential Diagnosis
Differential Diagnosis
- •
Keratoacanthoma
- •
Squamous cell carcinoma
- •
Wart
- •
Seborrheic keratosis
- •
Melanoma (pigmented basal cell carcinoma)
- •
Xeroderma pigmentosa
- •
Basal cell nevus syndrome—patients may have hundreds of BCCS ( Fig. 3.44 ).

FIG. 3.44
Patient with basal cell nevus syndrome (Gorlin’s syndrome) demonstrating numerous basal cell carcinoma of the back with both superficial and nodular growth patterns.
(Fitzsimons Army Medical Center Collection)
- •
Molluscum contagiosum
- •
Sebaceous hyperplasia
- •
Psoriasis
 Treatment
Treatment
First Line
- •
Treatment is variable with tumor size, location, and cell type:
- •
Excision surgery: preferred method for large tumors with well-defined borders on the legs, cheeks, forehead, and trunk.
- •
Mohs micrographic surgery: preferred for lesions in high-risk areas (e.g., ears, nose, eyelid), very large primary tumors, recurrent basal cell carcinomas, and tumors with poorly defined clinical margins.
- •
Electrodesiccation and curettage: useful for small (<6 mm) nodular basal cell carcinomas.
- •
Cryosurgery with liquid nitrogen: useful in basal cell carcinomas of the superficial and nodular types with clearly definable margins; no clear advantages over the other forms of therapy; generally reserved for uncomplicated tumors.
- •
Second Line
- •
Radiation therapy: generally used for basal cell carcinomas in areas requiring preservation of normal surround tissues for cosmetic reasons (e.g., around lips); also useful in patients who cannot tolerate surgical procedures or for large lesions and surgical failures.
Third Line
- •
Imiquimod 5% cream can be used for treatment of small, superficial BCCs of the trunk and extremities. Efficacy rate is approximately 80%. Its main advantage is lack of scarring, which must be weighed against higher cure rates with surgical intervention.
- •
Vismodegib and sonidegib are orally active hedgehog pathway inhibitors recently FDA approved for metastatic BCC, recurrent basal cell carcinoma postsurgery, and locally advanced BCC in patients who are not candidates for surgery or radiation. Both medications are expensive and have medical formulary limitations.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
More than 90% of patients are cured; however, periodic evaluation for at least 5 years is necessary because of increased risk of recurrence (40% risk within 5 years of treatment).
- •
A lesion is considered low risk if it is less than 1.5 cm in diameter, is nodular or cystic, is not in a difficult to treat area (H zone of face), and has not been previously treated.
- •
Nodular and superficial basal cell carcinomas are the least aggressive.
- •
Morpheaform lesions have the highest incidence of positive tumor margins (30%) and the greatest recurrence rate.
21
Becker’s Nevus
 General Comments
General Comments
Definition
- •
Becker’s nevus is an androgen–dependent lesion that becomes more prominent after puberty.
Etiology
- •
Unknown. It is not a melanocytic nevus but a hamartoma composed of increased melanin, enlarged hair shafts, and variable smooth muscle hyperplasia of the arrectores pilorum.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
It usually presents in the second decade, initially as an asymptomatic light to dark brown enlarging macular lesion, which subsequently shows hypertrichosis.
- •
It most frequently involves the chest, shoulder, or upper arm.
- •
Usually, it is unilateral.
- •
Associated abnormalities may include unilateral breast hypoplasia, localized lipoatrophy, vertebral defects, shoulder girdle and pectoralis hypoplasia, accessory mammary tissue, and multiple leiomyomas.
Physical Examination
- •
Unilateral irregularly pigmented macular lesions are seen with associated hypertrichosis ( Fig. 3.45 ).

FIG. 3.45
Becker’s nevus. This example shows a characteristic distribution around the shoulder region with macular hyperpigmentation and hypertrichosis.
(John Aeling Collection)
Diagnostic Tests
- •
Skin biopsy may be performed if diagnosis is uncertain.
 Differential Diagnosis
Differential Diagnosis
- •
Melanoma
- •
Congenital melanocytic nevus
- •
Postinflammatory pigmentation
- •
Nevus spilus
- •
Café-au-lait macule
 Treatment
Treatment
First Line
- •
Clinical observation only. No treatment is necessary.
Second Line
- •
Q-switched ruby laser
- •
Normal mode ruby laser
Third Line
- •
Electrolysis
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The risk of malignant transformation is very low. Follow-up melanoma screening is unnecessary.
22
Behçet’s Syndrome
 General Comments
General Comments
Definition
- •
Behçet’s syndrome is a chronic, relapsing, inflammatory disorder characterized by the presence of recurrent oral aphthous ulcers, genital ulcers, uveitis, and skin lesions. According to the International Study Group for Behçet’s Disease, the diagnosis of Behçet’s syndrome is established when recurrent oral ulceration is present along with at least two of the following in the absence of other systemic diseases:
- •
Recurrent genital ulceration
- •
Eye lesions
- •
Skin lesions
- •
Positive pathergy test (enlarging papules at sterile needle injection sites)
- •
Etiology
- •
The etiology of Behçet’s syndrome is unknown. An immune-related vasculitis is thought to lead to many of the manifestations of Behçet’s syndrome. What triggers the immune response and activation is not yet known.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Behçet’s syndrome typically affects individuals in the third to fourth decade of life and primarily presents with painful aphthous oral ulcers. The ulcers occur in crops measuring 2 to 10 mm in size and are found on the mucous membrane of the cheek, gingiva, tongue, pharynx, and soft palate.
- •
Genital ulcers are similar to the oral ulcers.
- •
Decreased vision secondary to uveitis, keratitis, or vitreous hemorrhage, or occlusion of the retinal artery or vein may occur.
- •
Skin findings include nodular lesions, which are histologically equally divided to erythema nodosum-like lesions ( Fig. 3.46 ) , superficial thrombophlebitis, and acneiform lesions; acneiform lesions are also presented at sites uncommon for ordinary acneiform (arms and legs).

FIG. 3.46
Erythematous painful nodules on the lower extremity, consistent with erythema nodosum, appeared in this patient with Behçet’s syndrome who also had recurrent aphthous ulcers and uveitis.
- •
Arthritis and arthralgias are common.
- •
Central nervous system (CNS): meningeal findings, including headache, fever, and stiff neck, can occur. Cerebellar ataxia and pseudobulbar palsy occur with involvement of the brainstem.
- •
Vasculitis leading to both arterial and venous inflammation or occlusion can result in signs and symptoms of a myocardial infarction, intermittent claudication, deep vein thrombosis, hemoptysis, and aneurysm formation.
Physical Examination
- •
Papulopustular lesions are the most commonly encountered skin manifestations.
- •
Recurrent oral ulceration ( Fig. 3.47 ) is an invariable feature of this condition.

FIG. 3.47
Recurrent, painful, well-demarcated, oral aphthous ulcers are hallmark findings in patients with Behçet’s syndrome.
(William Weston Collection)
- •
The ulcers measure up to 1 cm across and develop anywhere in the oral cavity, pharynx, and even the larynx. They are painful and usually regress spontaneously within 14 days. A yellow, necrotic crust typically covers the ulcer floor.
- •
Typical of Behcet’s syndrome and an important diagnostic clue is the development of sterile pustules at sites of mild skin trauma such as injection sites (pathergy).
- •
Genital lesions, similar in appearance to those of the oral mucosa, occur on the scrotum ( Fig. 3.48 ) , penis, vagina, and vulva ( Fig. 3.49 ).

FIG. 3.48
Punched-out ulcers on the scrotum, penis, or other areas of the genitalia, in the presence of oral aphthae are consistent with a diagnosis of Behçet’s syndrome.
(Fitzsimons Army Medical Center Collection)

FIG. 3.49
Large ulcer of the female genitalia in a woman with Behçet’s syndrome.
(Joanna Burch Collection)
Diagnostic Tests
- •
The diagnosis of Behçet’s syndrome is a clinical diagnosis. Laboratory tests and x-ray imaging may be helpful in evaluating the complications of Behçet’s syndrome or excluding other diseases in the differential.
- •
There are no diagnostic laboratory tests for Behçet’s syndrome.
- •
Computed tomography (CT) scan, magnetic resonance imaging (MRI), and angiography are useful for detecting CNS and vascular lesions.
 Differential Diagnosis
Differential Diagnosis
- •
Ulcerative colitis
- •
Crohn’s disease
- •
Lichen planus
- •
Pemphigoid
- •
Herpes simplex infection
- •
Benign aphthous stomatitis
- •
SLE
- •
Reiter’s syndrome
- •
Ankylosing spondylitis
- •
AIDS
- •
Hypereosinophilic syndrome
- •
Sweet’s syndrome
 Treatment
Treatment
Oral and Genital Ulcers
- •
Topical corticosteroids
- •
Tetracycline tablets 250 mg dissolved in 5 mL water and applied to the ulcer for 2 to 3 minutes
- •
Colchicine
- •
Thalidomide
- •
Dapsone
- •
Pentoxifylline
- •
Azathioprine
- •
Methotrexate
Ocular Lesions
- •
Anterior uveitis treated by ophthalmologist with topical corticosteroids (e.g., betamethasone 1 to 2 drops TID); topical injection with dexamethasone has also been utilized
- •
Infliximab 5 mg/kg single dose
CNS Disease
- •
Chlorambucil for treatment of posterior uveitis, retinal vasculitis, or CNS disease; patients not responding can be given cyclosporine
- •
In CNS vasculitis, cyclophosphamide may be useful; prednisone is an alternative
Arthritis
- •
Nonsteroidal antiinflammatory drugs (NSAIDs, e.g., ibuprofen or indomethacin)
- •
Alternative treatment: Sulfasalazine
GI Lesions
- •
Sulfasalazine
- •
Prednisone
Vascular Lesions
- •
Prednisone
- •
Cytotoxic agents as mentioned previously
- •
Heparin 5000 to 20,000 U/day followed by oral warfarin
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The aphthous oral ulcers last 1 to 2 weeks, recurring more frequently than genital ulcers.
- •
Approximately 25% of patients with ocular lesions become blind.
23
Blastomycosis (North American Blastomycosis)
 General Comments
General Comments
Definition
- •
Blastomycosis is a systemic pyogranulomatous disease caused by a dimorphic fungus, Blastomyces dermatitidis ( Fig. 3.50 ).
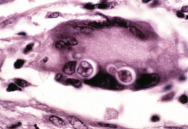
FIG. 3.50
North American blastomycosis demonstrating thick-walled, budding yeast with a multinucleated giant cell.
(Fitzsimons Army Medical Center Collection)
Etiology
- •
Blastomyces dermatitidis exists in warm, moist soil that is rich in organic material. Most patients reside in the southeastern and south central states, especially those bordering the Mississippi and Ohio River valleys, the Midwestern states, and Canadian provinces bordering the Great Lakes. When these microfoci are disturbed, the aerosolized spores or conidia are inhaled into the lungs. Disease at other sites is a result of dissemination from the initial pulmonary infection; the latter may be acute or chronic.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Widely disseminated disease is most common in immunocompromised hosts, especially those with AIDS.
- •
Initial infections result from inhalation of conidia into the lungs, although primary cutaneous blastomycosis has been reported after dog bites.
- •
Acute infection: Fewer than 50% of patients are symptomatic. The median incubation period is 30 to 45 days. Symptoms are nonspecific and mimic influenza or bacterial infection with abrupt onset of myalgias, arthralgias, chills, and fever; transient pleuritic pain; and cough that is initially nonproductive. Resolution within 4 weeks is usual.
Physical Examination
- •
Cutaneous is most common and may occur with or without pulmonary disease. Two different lesions may develop:
- 1.
Verrucous ( Fig. 3.51 ) : This begins as a small papulopustular lesion on exposed body areas and may develop into an eschar with peripheral microabscesses.

FIG. 3.51
Verrucous lesions of North American blastomycosis acquired in Colorado.
(Fitzsimons Army Medical Center Collection)
- 2.
Ulcerative ( Fig. 3.52 ) : Subcutaneous nodules (cold abscesses) and, rarely, cutaneous inoculation blastomycosis may occur.

FIG. 3.52
Ulcerated lesion of the foot in a patient with blastomycosis acquired in Kentucky.
(Fitzsimons Army Medical Center Collection)
- 1.
Diagnostic Tests
- •
Presumptive diagnosis can be made by visualizing the distinctive yeast forms in clinical specimens.
- •
Culture is done on Sabouraud’s or more enriched media.
- •
Aspirated material from abscesses
- •
Skin scrapings
- •
Prostatic secretions (urine culture with prostatic massage)
- •
Direct examination of specimens can be performed.
- •
Wet preparation with 10% KOH
- •
Histopathology: typically demonstrates pyogranulomas; yeast identification requires special stains
 Differential Diagnosis
Differential Diagnosis
- •
Bromoderma
- •
Pyoderma gangrenosum
- •
Mycobacterium marinum infection
- •
Squamous cell carcinoma
- •
Giant keratoacanthoma
 Treatment
Treatment
First Line
- •
Itraconazole is the drug of choice except for patients with CNS disease or with fulminant illness who require amphotericin B.
- •
Amphotericin is recommended in immunocompromised patients, those with life-threatening disease or CNS disease, or those who have failed azole treatment. This is the only drug approved for treating blastomycosis in pregnant women.
Second Line
- •
Fluconazole can be given if the patient is unable to tolerate itraconazole or amphotericin.
Third Line
- •
Ketoconazole for 6 months is an option in mild-to-moderate disease.
- •
Surgery may be indicated for drainage of large abscesses.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Colonization does not occur with blastomycosis as with Candida and Aspergillus species.
24
Blue Nevus
 General Comments
General Comments
Definition
- •
Blue nevi represent a heterogeneous group of well-defined blue papules or nodules.
Etiology
- •
Arrested embryonal migration of melanocytes bound for the dermal–epidermal junction
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
The nevus appears blue gray clinically due to the deep dermal location of the melanin pigment and the Tyndall effect (the brown segment absorbs the longer wavelengths of light and scatters blue light).
Physical Examination
- •
Round or oval, bluish black or dark blue, sharply circumscribed, slightly elevated dome-shaped papule, nodule, or plaque ( Fig. 3.53 )

FIG. 3.53
Large, blue nevus, lateral to the eye in a child.
(Joanna Burch Collection)
- •
Usually less than 0.5 cm diameter
- •
Most common on the extremities and dorsum of hands
Diagnostic Tests
- •
None necessary
 Differential Diagnosis
Differential Diagnosis
- •
Melanoma
- •
Nevus of Ota
- •
Spitz nevus
 Treatment
Treatment
First Line
- •
Benign-appearing blue nevi do not require excision.
Second Line
- •
Excision in rare cases of malignant transformation
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The term “malignant blue nevus” refers to melanomas arising in a blue nevus.
25
Bowen’s Disease (Squamous Cell Carcinoma In Situ)
 General Comments
General Comments
Definition
- •
Bowen’s disease is a type of in situ carcinoma also known as intraepithelial carcinoma, Bowen’s carcinoma, or squamous carcinoma in situ, or as erythroplasia of Queyrat when involving the glans penis under the foreskin of an uncircumcised penis.
Etiology
- •
UV light
- •
Human papillomavirus (HPV)
- •
Chemicals (arsenic)
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Insidious onset with slowly enlarging asymptomatic lesion
- •
May arise in sun-exposed (head and neck) and sun-protected areas
Physical Examination
- •
Scaly patch ( Fig. 3.54 ) is sharply demarcated and erythematous in appearance.

FIG. 3.54
Bowen’s disease, or in situ squamous cell carcinoma, often appears as a scaly, eczematous plaque on the extremities.
(Fitzsimons Army Medical Center Collection)
- •
Lesions may be up to several centimeters.
- •
Lesions are usually solitary but may be multiple in 20% of cases.
- •
When involving the penis, there is a red well-demarcated patch often said to be velvety but that may be quite shiny and moist appearing. Maceration may cause a white appearance and may be mistaken for candidiasis until evaporation brings out the true color.
Diagnostic Tests
- •
Skin biopsy
- •
Immunoperoxidase studies for HPV (selected cases)
 Differential Diagnosis
Differential Diagnosis
- •
Psoriasis
- •
Basal cell carcinoma
- •
Lupus
- •
Actinic keratosis
- •
Seborrheic keratosis
- •
Paget’s disease
 Treatment
Treatment
First Line
- •
Surgical excision (for well-defined and small lesions) or Mohs micrographic surgery (for ill-defined, large lesions)
Second Line
- •
5-fluorouracil cream or topical imiquimod (useful in patients with multiple lesions)
- •
Electrodessication and curettage
- •
Liquid nitrogen cryosurgery
- •
Photodynamic therapy (PDT)
Third Line
- •
Laser ablation
- •
Radiation therapy
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Erythroplasia of Queyrat is a more aggressive lesion with propensity for invasion and metastases.
26
Bullous Pemphigoid
 General Comments
General Comments
Definition
- •
Bullous pemphigoid refers to an autoimmune, subepidermal blistering disease that is most commonly seen in the elderly. It is the most common of the autoimmune bullous dermatoses.
Etiology
- •
Bullous pemphigoid is an autoimmune disease with IgG and/or C3 complement component reacting with antigens located in the basement membrane zone.
- •
Drug-induced pemphigoid, although rare, can occur in patients taking penicillamine, furosemide, captopril, penicillin, and sulfasalazine.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Bullous pemphigoid typically starts as an eczematous or urticarial lesion, with the lower extremities being the most common location. Blisters form between one week and several months.
- •
Anatomic distribution involves the flexor surfaces of the arms, legs, groin, axilla, and lower abdomen ( Fig. 3.55 ). The head and neck are generally spared. The lesions are irregularly grouped but sometimes can be serpiginous. Oral lesions can be found occasionally.

FIG. 3.55
Urticarial, inflammatory plaques can appear before bulla formation in bullous pemphigoid. This elderly man demonstrates both types of lesions.
(Fitzsimons Army Medical Center Collection)
Physical Examination
- •
The typical blistering bullae measure from 5 mm to 2 cm in diameter and contain clear or bloody fluid ( Fig. 3.56 ). They may arise from normal skin or from an erythematous base and heal without scarring if denuded.

FIG. 3.56
Severe bullous pemphigoid with numerous tense blisters on the lower leg, a common site for lesions of bullous pemphigoid.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
Skin biopsy staining with hematoxylin and eosin reveals subepidermal blisters.
- •
Direct and indirect immunofluorescence studies can be done to detect the presence of IgG and C3 immune complexes ( Fig. 3.57 ).
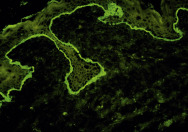
FIG. 3.57
Direct immunofluorescent study of perilesional skin in bullous pemphigoid demonstrating a strong linear band of IgG directed against the basement membrane zone.
- •
Immunoelectron microscopy also reveals immune deposits on the basement membrane zone.
 Differential Diagnosis
Differential Diagnosis
- •
Cicatricial pemphigoid
- •
Epidermolysis bullosa acquisita
- •
Pemphigus
- •
Pemphigoid nodularis
- •
Bullous lupus erythematosus
- •
Herpes gestationis
- •
Erythema multiforme
 Treatment
Treatment
First Line
- •
Treatment of bullous pemphigoid is based on the degree of involvement and rate of disease’s progression.
- •
Topical steroids in general have been used in patients with localized bullous pemphigoid.
- •
Systemic corticosteroids are considered the standard treatment for more advanced bullous pemphigoid.
Second Line
- •
Azathioprine
- •
Mycophenolate mofetil
- •
Methotrexate
Third Line
- •
Cyclophosphamide
- •
Dapsone
- •
Plasmapheresis
- •
IVIG
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Antibodies to the basement membrane zone are detected in the serum in 70% of patients with bullous pemphigoid.
27
Burns
 General Comments
General Comments
Definition
- •
Burns are defined as thermal, radiation, chemical, or electrical injury to the skin.
Etiology
- •
Burns can be caused by excessive sun exposure ( Fig. 3.58 ) , flames, scalds ( Fig. 3.59 ) , and cigarettes, as well as chemical ( Fig 3.60 ) , electrical, and radiation sources.

FIG. 3.58
First-degree burn, confined to the epidermis, with erythema and pain. This patient suffered severe sunburn because of incomplete application of sunscreen.
(William Weston Collection)

FIG. 3.59
Severe blistering with disruption of the dermis caused by a second-degree burn from boiling water.
(William Weston Collection)

FIG. 3.60
Second-degree chemical burn in child requiring hospitalization and intubation.
(William Weston Collection)
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Classification of burns is as follows:
Major Burns
- •
Partial-thickness burns covering more than 25% of total body surface area (TBSA) or 20% if younger than 10 or older than 50 years
- •
Full-thickness burns covering more than 10% TBSA
- •
Burns crossing major joints or involving the hands, face, feet, or perineum
- •
Electrical or chemical burns
- •
Burns complicated by inhalation injury or involving high-risk patients (extremes of age/comorbid diseases)
Moderate Burns
- •
Partial-thickness burns covering 15% to 25% TBSA (or 10% in children and older adults)
- •
Full-thickness burns covering 2% to 10% TBSA and not involving the specific conditions of major burns
Minor Burns
- •
Partial-thickness burns covering less than 15% TBSA or full-thickness burns covering less than 2% TBSA
Physical Examination
- •
Burns are defined by size and depth.
- •
First-degree burns (superficial) involve the epidermis only and appear painful and red.
- •
Second-degree burns involve the dermis and appear blistered, moist, and red with two-point discrimination intact (superficial partial thickness) or red and blanched white with only sensation of pressure intact (deep partial thickness).
- •
Third-degree burns (full thickness) extend through the dermis with associated destruction of hair follicles and sweat glands. The skin is charred, pale, painless, and leathery. These burns are caused by flames, immersion scalds, chemicals, and high-voltage injuries.
- •
The extent of a burn is described as a percentage of the total body surface area.
- •
Scars ( Fig. 3.61 ) may develop depending on the depth of the burn. Radiation burns may develop persistent ulcers that are difficult to heal ( Fig. 3.62 ).

FIG. 3.61
Scar at the angle of mouth from biting an electrical cord.
(William Weston Collection)

FIG. 3.62
Recalcitrant ulceration of the chest wall from radiation therapy.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
Chest radiographs and bronchoscopy if smoke inhalation suspected
- •
CBC, electrolytes, blood urea nitrogen (BUN), creatinine, albumin, and glucose
- •
Serial arterial blood gas (ABG) and carboxyhemoglobin if smoke inhalation suspected
- •
Urinalysis, urine myoglobin, and creatine phosphokinase (CPK) levels if concern for rhabdomyolysis
 Differential Diagnosis
Differential Diagnosis
- •
Cellulitis/abscess
- •
Insect bite (spider bite)
- •
Bullous erysipelas
- •
Carbuncle/furuncle
- •
Anthrax
 Treatment
Treatment
- •
Minor burns are amenable to outpatient treatment with cool compresses, silver sulfadiazine, and nonadherent dressing followed by a sterile gauze wrap. Ruptured blisters should be sharply debrided (except palms and soles). Unruptured blisters should be left intact. Moderate and major burns should be treated in specialized burn care facilities according to the principles described below:
- •
Establish airway: inspect for inhalation injury and intubate for suspected airway edema (often seen 12–24 hr later); administer supplemental O 2 .
- •
Remove jewelry and clothing and place one or two large-bore peripheral intravenous lines (if TBSA affected is >20%).
- •
Provide fluid resuscitation with Ringer’s lactate at 2 to 4 mL/kg/%TBSA/24 hr with half the calculated fluid given in the first 8 hours.
- •
Insert Foley catheter and nasogastric (NG) tube (20% of patients develop an ileus).
- •
Update tetanus if needed.
- •
Provide medications for pain control.
- •
Provide stress ulcer prophylaxis in high-risk patients.
- •
Prophylactic antibiotics are not recommended; however, burn patients should be considered immunosuppressed.
- •
 Clinical Pearl(s)
Clinical Pearl(s)
- •
High-voltage burn patients should have electrocardiographic (ECG) monitoring because they are at increased risk for arrhythmia.
28
Café Au Lait Macule
 General Comments
General Comments
Definition
- •
Café au lait macules are well-circumscribed brownish macules caused by an increased number of functionally hyperactive melanocytes.
Etiology
- •
They may be found at birth in up to 10% of the population.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Asymptomatic
- •
Generally, there no associated abnormalities, but they can be markers for neurofibromatosis I, centrofacial lentigines syndrome, and Watson syndrome.
Physical Examination
- •
Discrete tan macules 2 to 20 mm diameter ( Fig. 3.63 ) that may be brown in darker skin ( Fig. 3.64 )

FIG. 3.63
Isolated 3-cm × 5-cm, light brown macule with irregular borders.

FIG. 3.64
Large, dark brown, café-au-lait macule in an infant. Café-au-lait macules are darker brown in patients with darker skin types.
(Joanna Burch Collection)
Diagnostic Tests
- •
None necessary
 Differential Diagnosis
Differential Diagnosis
- •
Seborrheic keratosis
- •
Multiple lentigines syndrome
- •
Lentigo
- •
Nevi
 Treatment
Treatment
First Line
- •
No treatment necessary
Second Line
- •
Laser ablation
Third Line
- •
Hydroquinone 4% cream
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The presence of more than six macules measuring greater than 5 mm in diameter is suggestive of neurofibromatosis I.
29
Candidiasis
 General Comments
General Comments
Definition
- •
Candidiasis is a cutaneous or mucous membrane infection.
Etiology
- •
The condition is caused by the yeast Candida albicans.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
The intertriginous skin folds such as the inner thighs, axillae ( Fig. 3.65 ) , or other moist, occluded sites such as underneath the breasts or in diaper area in infants ( Fig. 3.66 ) are most commonly affected.

FIG. 3.65
Candida intertrigo of the axilla demonstrating intensely erythematous papules.
(Fitzsimons Army Medical Center Collection)

FIG. 3.66
Candidiasis often occurs in moist areas such as the diaper area in children.
(William Weston Collection)
- •
The infection may affect the foreskin and glans penis (candidal balanitis [ Fig. 3.67 ]) and the scrotum ( Fig. 3.68 ).

FIG. 3.67
Candidiasis of the penis appearing as a diffuse, moist, erythematous dermatitis.
(John Aeling Collection)

FIG. 3.68
Candidiasis appearing as a confluent, erythematous dermatitis involving the lower abdomen, penis, and scrotum with peripheral satellite lesions, a characteristic finding in candidiasis.
(Fitzsimons Army Medical Center Collection)
Physical Examination
- •
The affected area has a red, glistening surface with an advancing border and cigarette paper–like scaling.
Diagnostic Tests
- •
Diagnosis is usually made on clinical grounds.
- •
Presence of pseudohyphae and yeast forms on KOH preparation or other stains confirms the diagnosis.
- •
Serum glucose and HIV serology can be performed in recurrent cases.
 Differential Diagnosis
Differential Diagnosis
- •
Tinea
- •
Eczema
- •
Seborrheic dermatitis
- •
Psoriasis
- •
Cellulitis
 Treatment
Treatment
First Line
- •
Affected skin sites that are moist should be dried out with wet-to-dry soaks and exposed to air.
- •
Topical antifungal products (miconazole, clotrimazole, econazole) are generally effective.
Second Line
- •
Oral therapy (fluconazole, itraconazole) is reserved for resistant cases.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Factors that predispose to infection include diabetes mellitus, obesity, increasing moisture, use of systemic corticosteroids or antibiotics, and immunocompromised status.
30
Cellulitis
 General Comments
General Comments
Definition
- •
Cellulitis is an infection of the subcutaneous tissues.
Etiology
- •
Group A beta-hemolytic streptococci (may follow a streptococcal infection of the upper respiratory tract)
- •
Staphylococcal cellulitis
- •
Haemophilus influenzae
- •
Vibrio vulnificus: higher incidence in patients with liver disease (75%) and in immunocompromised hosts (corticosteroid use, diabetes mellitus, leukemia, renal failure)
- •
Erysipelothrix rhusiopathiae: common in people handling poultry, fish, or meat
- •
Aeromonas hydrophila: generally occurring in contaminated open wound in fresh water
- •
Fungi ( Cryptococcus neoformans ): immunocompromised granulopenic patients
- •
Gram-negative rods ( Serratia, Enterobacter, Proteus, Pseudomonas species): immunocompromised or granulopenic patients
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Cellulitis is generally characterized by erythema, warmth, and tenderness of the area involved ( Fig. 3.69 ).

FIG. 3.69
Cellulitis presenting as sharply demarcated, erythematous, edematous lesion of the buttock.
(John Aeling Collection)
Physical Examination
- •
Erysipelas: A superficial, spreading, warm, erythematous lesion is distinguished by its indurated and elevated margin. Lymphatic involvement and vesicle formation are common.
- •
Staphylococcal cellulitis: The area involved is erythematous, hot, and swollen; it can be differentiated from erysipelas by nonelevated, poorly demarcated margins. Local tenderness and regional adenopathy are common. Up to 85% of cases occur on the legs ( Fig. 3.70 ) and feet.

FIG. 3.70
Edematous, warm, erythematous left calf present for 3 days. This chronically edematous leg was especially vulnerable to recurrent cellulitis because it had been the site for donor graft vein harvesting several years ago for coronary artery bypass grafting (CABG) surgery.
- •
H. influenzae cellulitis: The area involved is a blue-red/purple-red. It occurs mainly in children and generally involves the face in children and the neck or upper chest in adults.
- •
Vibrio vulnificus: This is characterized by larger hemorrhagic bullae, cellulitis, lymphadenitis, and myositis. It is often found in critically ill patients in septic shock.
Diagnostic Tests
- •
Gram stain and culture (aerobic and anaerobic)
- •
Skin scrapings for mycology
- •
Blood cultures in hospitalized patients, in patients who have cellulitis superimposed on lymphedema, in patients with buccal or periorbital cellulitis, and in patients suspected of having a saltwater or freshwater source of infection
 Differential Diagnosis
Differential Diagnosis
- •
Erythrasma
- •
Septic arthritis
- •
DVT
- •
Peripheral vascular insufficiency
- •
Paget’s disease of the breast
- •
Thrombophlebitis
- •
Acute gout
- •
Psoriasis
- •
Candida intertrigo
- •
Pseudogout
- •
Osteomyelitis
- •
Insect bite
- •
Lymphedema
 Treatment
Treatment
- •
Immobilization and elevation of the involved limb; cool sterile saline dressings to remove purulence from any open lesion
- •
Erysipelas: dicloxacillin PO or nafcillin or cefazolin IV
- •
Staphylococcus cellulitis: dicloxacillin PO or nafcillin or cefazolin IV
- •
H. influenzae cellulitis: dicloxacillin PO or nafcillin or cefazolin IV
- •
V. vulnificus: doxycycline or third-generation cephalosporin
- •
Erysipelothrix: penicillin
- •
Aeromonas hydrophila: aminoglycosides, chloramphenicol
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Bacteremia is uncommon in cellulitis (positive blood cultures in only 4% of patients). Culture of aspirates of bullae may be useful to identify causative organisms. Surface swabs are generally unhelpful.
31
Chancroid
 General Comments
General Comments
Definition
- •
Chancroid is a sexually transmitted disease characterized by painful genital ulceration and inflammatory inguinal adenopathy.
Etiology
- •
Chancroid is caused by Haemophilus ducreyi, a gram-negative facultative anaerobic bacillus.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Chancroid occurs more commonly in men (male-to-female ratio of 10:1).
- •
There is a higher incidence in uncircumcised men and in tropical and subtropical regions.
- •
The incubation period is 3 to 7 days but may take up to 3 weeks.
Physical Examination
- •
Primary lesion is one to three extremely painful, often ragged ulcers ( Fig. 3.71 ).

FIG. 3.71
Chancroid. Painful, nonindurated ulcer of the penis acquired from a prostitute.
(Fitzsimons Army Medical Center Collection)
- •
In men, the ulcer is most commonly located on the penis.
- •
In women, the initial lesion is seen in the fourchette, labia minora, urethra, cervix, or anus, followed by an inflammatory pustule or papule that ruptures, leaving a shallow, nonindurated ulceration, usually 1 to 2 cm in diameter with ragged, undermined edges.
- •
Unilateral, often fluctuant lymphadenopathy develops 1 week later in 50% of patients ( Fig. 3.72 ).

FIG. 3.72
Chancroid. Ragged, tender ulcer with tender regional lymphadenopathy.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
Darkfield microscopy of smears or aspirate
- •
Rapid plasma reagin (RPR)
- •
Herpes simplex virus (HSV) cultures
- •
H. ducreyi culture (difficult to culture)
- •
HIV testing
 Differential Diagnosis
Differential Diagnosis
- •
Syphilis
- •
HSV
- •
Lymphogranuloma venereum (LGV)
- •
Granuloma inguinale
- •
Traumatic ulceration
- •
Behçet’s syndrome
- •
Crohn’s disease
 Treatment
Treatment
First Line
- •
A single dose of ceftriaxone 250 mg IM can be given.
- •
A single dose of azithromycin 1 g PO can be given.
- •
HIV-infected patients may need more prolonged therapy.
- •
Fluctuant nodes should be aspirated through healthy adjacent skin to prevent formation of draining sinus. Incision and drainage (I&D) is not recommended because it delays healing. Use warm compresses to remove necrotic material.
Second Line
- •
Ciprofloxacin 500 mg PO BID for 3 days
- •
Erythromycin 500 mg PO QID for 7 days
Note: Ciprofloxacin is contraindicated in patients who are pregnant, lactating, or younger than 18 years old.
Third Line
- •
Thiamphenicol
- •
Spectinomycin
 Clinical Pearl(s)
Clinical Pearl(s)
- •
All sexual partners should be treated.
- •
A high incidence of HIV infection is associated with chancroid.
32
Chondrodermatitis Nodularis
 General Comments
General Comments
Definition
- •
Chronic inflammatory lesion found on the helix of the ear
Etiology
- •
Unknown. Chronic sun exposure and/or chronic mechanical pressure may be contributing factors.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
More than 90% of cases occur in men over age 40.
- •
Base may become red and swollen and produce significant pain.
Physical Examination
- •
Dull and red-white nodular mass on the helix of the ear ( Fig. 3.73 ) ; less commonly on the antihelix ( Fig. 3.74 )

FIG. 3.73
Chondrodermatitis nodularis helicus on the helix, by far the most common site.
(Fitzsimons Army Medical Center Collection)

FIG. 3.74
Chondrodermatitis nodularis helicus on the antihelix, the second most common site. This location is particularly common in patients with hearing aids and those that use telephones or headsets for prolonged periods.
(Fitzsimons Army Medical Center Collection)
- •
Lesions are 2 to 6 mm in diameter and well defined.
- •
A central scale may be present, and removal of the scale may reveal a central erosion.
Diagnostic Tests
- •
Biopsy of lesion if suspecting squamous cell carcinoma
 Differential Diagnosis
Differential Diagnosis
- •
Squamous cell carcinoma
- •
Chronic trauma
 Treatment
Treatment
First Line
- •
Use of special pillow to reduce pressure on area when sleeping
- •
Topical nitroglycerin
Second Line
- •
Excision of nodule
Third Line
- •
CO 2 laser
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Ischemic necrosis of the dermis occurs often on the side the patient favors during sleep.
33
Cicatricial Pemphigoid
 General Comments
General Comments
Definition
- •
Cicatricial pemphigoid is a rare blistering disorder (incidence 1:15,000) often presenting in females in the seventh decade.
Etiology
- •
This is an autoimmune disorder due to autoantibodies directed against components of the basement membrane zone.
- •
Oral lesions occur in 85% to 95% of patients and commonly follow mild trauma.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Insidious onset of painful blisters occurs in mucous membranes, usually in elderly patients.
- •
The oral cavity is affected in 90% of cases and the conjunctiva in 70%. Other sites of involvement include the upper airway (45%), skin (30%), and genitalia (15%).
- •
Desquamative gingivitis is the most common manifestation. Lesions present as painful areas of erosion, erythema, and ulceration.
- •
Patients with this condition present with painful, swollen, erythematous lesions of the gums, which may be associated with bleeding, blistering, erosions, and ulcerations.
Physical Examination
- •
Bullae, erosions, and erythema most commonly affect the gingival or buccal mucosa, but the hard and soft palate ( Fig. 3.75 ) , tongue, and lips are also often involved.

FIG. 3.75
Cicatricial pemphigoid presenting as erosions of the palate. Bullous lesions are not typically seen on mucosal sites but are characteristically present if there is cutaneous involvement.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
Biopsy and direct immunofluorescence studies will demonstrate autoantibodies (usually IgG and/or IgA) directed against the basement membrane zone ( Fig. 3.76 )
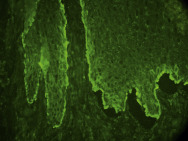
FIG. 3.76
Direct immunofluorescent study of perilesional mucosa in cicatricial pemphigoid demonstrating linear deposition of IgG along the basement membrane zone. Linear C3 and sometimes linear IgA may also be present.
 Differential Diagnosis
Differential Diagnosis
- •
Bullous pemphigoid
- •
Erythema multiforme
- •
Dermatitis herpetiformis
- •
Linear IgA dermatosis
- •
Pemphigus
- •
Stevens-Johnson syndrome
- •
HSV, herpes zoster
 Treatment
Treatment
First Line
- •
Topical corticosteroids (fluocinonide 0.05% gel applied QID to mucous membranes)
Second Line
- •
Systemic corticosteroids
Third Line
- •
Dapsone
- •
Cyclophosphamide
- •
Azathioprine
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Cicatricial pemphigoid is often associated with severe morbidity, largely due to the effects of the associated scarring.
34
Cold Urticaria
 General Comments
General Comments
Definition
- •
Edema and whealing of exposed skin areas following exposure to cold temperatures
Etiology
- •
Cold urticaria may be primary (essential, not associated with underlying systemic diseases or cold-reactive proteins), secondary (associated with other disorders such as cryoglobulinemia, cryofibrinogenemia hepatitis, syphilis, mononucleosis, multiple myeloma), and familial
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Fatal shock may occur in patients with primary cold urticarial when swimming in cold water or taking cold showers
- •
Urticaria may occur in the nasopharynx after a cold drink
- •
Cold urticarial often begins after an infection
- •
Familial cold urticarial produces a burning sensation rather than itching and may be accompanied by fever, chills, myalgias
Physical Examination
- •
Presence of hive within minutes of exposure to cold
Diagnostic Tests
- •
Induction of hive on skin area occurs following contact with plastic-wrapped ice cube for 5 to 15 min ( Fig. 3.77 ).

FIG. 3.77
Wheal produced by an ice cube in a patient with cold urticaria.
(Fitzsimons Army Medical Center Collection)
- •
Urticaria does not develop during chilling but upon rewarming.
- •
The wheal typically lasts about 30 min.
- •
Cryoglobulins, ANA, ESR, RPR, cold agglutinins, RF, monospot test in suspected secondary cold urticaria
 Differential Diagnosis
Differential Diagnosis
- •
Dermatographism
- •
Cholinergic urticaria
- •
Adrenergic urticaria
- •
Aquagenic pruritus
- •
Pressure urticaria
 Treatment
Treatment
First Line
- •
Protection from sudden drop in temperature
- •
Desensitization by repeated increased exposure to cold
Second Line
- •
Antihistamines (cetirizine, loratadine)
Third Line
- •
Doxepin, cyproheptadine
- •
Antibiotics (penicillin)
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Ice cube test will be negative in familial cold urticarial.
35
Compound Nevi
 General Comments
General Comments
Definition
- •
Benign melanocytic proliferation composed of nevomelanocytes at the dermoepidermal junction and in the dermis
Etiology
- •
Unknown
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
More common in older children and adults but may also be present in younger children
Physical Examination
- •
Flesh-colored to brown papule ( Fig. 3.78 )
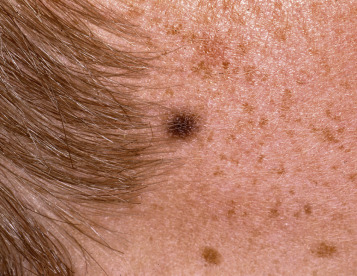
FIG. 3.78
Compound nevus. Brown, symmetric papule with no atypical features in a patient with numerous smaller freckles.
(William Weston Collection)
- •
Elevated, uniformly round, oval, and symmetric
- •
Surface may be smooth or verrucous and may contain dark coarse hairs
Diagnostic Tests
- •
None
- •
Biopsy for histologic examination
 Differential Diagnosis
Differential Diagnosis
- •
Junctional nevus
- •
Dermal nevus
- •
Melanoma
 Treatment
Treatment
First Line
- •
Observation and reassurance, no treatment needed
 Clinical Pearl(s)
Clinical Pearl(s)
- •
If a white area of depigmentation is present on the periphery of the lesion, it is referred to as a “halo nevus.” This represents lymphocytic destruction of melanocytes in the area.
36
Condyloma Acuminatum (Genital Warts)
 General Comments
General Comments
Definition
- •
Condyloma acuminatum is a sexually transmitted viral disease of the vulva, vagina, cervix, and perianal area in women and on the penis, perianal area, and scrotum in men.
Etiology
- •
HPV infection: more than 150 types of viral DNA have been identified. Transmission of warts is by direct contact. Approximately 40 different types of HPV are transmitted through sexual contact.
- •
Genital warts: 90% are caused by HPV types 6 or 11. HPV types 16, 18, 31, 33, and 35 are found occasionally in visible genital warts (usually as coinfections with HPV 6 or 11) and can be associated with foci of high-grade, intraepithelial neoplasia, particularly in persons who are infected with HIV infection. In addition to warts on genital areas, HPV types 6 and 11 have been associated with conjunctival, nasal, oral, and laryngeal warts.
- •
Virus is shed from both macroscopic and microscopic lesions.
- •
Predisposing conditions include diabetes, pregnancy, local trauma, and immunosuppression (e.g., transplant patients, those with HIV infection).
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Condyloma acuminatum is seen mostly in young adults, with a mean age of onset of 16 to 25 years.
- •
The average incubation time is 2 months (range: 1–8 months).
- •
Lesions are usually found in the genital area ( Fig. 3.79 ) or perianal area ( Fig. 3.80 ) but can be present elsewhere.

FIG. 3.79
Extensive condylomata acuminata (venereal wart) of the penis.
(John Aeling Collection)

FIG. 3.80
Multiple, perianal condylomata acuminata in child. Although sexually transmitted HPV infection should be considered, most of condylomata acuminata in children are not acquired from sexual abuse.
(William Weston Collection)
- •
Lesions are usually in similar positions on both sides of perineum.
- •
The condition is usually asymptomatic, but the lesions can cause pain, odor, or bleeding.
- •
Vulvar condyloma is more common than vaginal and cervical.
Physical Examination
- •
Initial lesions are pedunculated, soft papules about 2 to 3 mm in diameter, 10 to 20 mm long; they may occur as a single papule or in clusters. There are four morphologic types: condylomatous, keratotic, papular, and flat warts.
- •
Size of the lesions varies from pinhead to large cauliflowerlike masses.
- •
Intraanal warts occur predominantly in patients who have had receptive anal intercourse, in contrast with perianal warts, which may occur in men and women without a history of anal sex.
Diagnostic Tests
- •
Colposcopic examination of the lower genital tract from cervix to perianal skin with 3% to 5% acetic acid
- •
Biopsy of vulvar lesions that lack the classic appearance of warts and that become ulcerated or fail to respond to treatment
- •
Biopsy of flat white or ulcerated cervical lesions
 Differential Diagnosis
Differential Diagnosis
- •
Molluscum contagiosum
- •
Condyloma latum
- •
Acrochordon (skin tags) or seborrheic keratosis
- •
Epidermal nevi
- •
Hypertrophic actinic keratosis
- •
Squamous cell carcinomas
- •
Acquired digital fibrokeratoma
- •
Varicella-zoster virus in patients with AIDS
- •
Recurrent infantile digital fibroma
- •
Plantar corns (may be mistaken for plantar warts)
- •
Abnormal anatomic variants or skin tags around labia minora and introitus
- •
Pearly penile papules
- •
Dysplastic warts
- •
Seborrheic keratosis
- •
Erythroplasia of Queyrat
- •
Lichen planus
- •
Verrucous carcinoma
- •
Bowenoid papulosis
 Treatment
Treatment
First Line
- •
Cryosurgery with liquid nitrogen delivered with a probe or as a spray is effective for treating smaller genital warts.
- •
Twenty percent podophyllin resin in compound tincture of benzoin is applied with a cotton tip applicator by the treating physician and allowed to air dry. The treatment can be repeated weekly if necessary. Podofilox (Condylox 0.5% gel) is available for application by the patient. Local adverse effects include pain, burning, and inflammation at the site.
Second Line
- •
Imiquimod cream is a patient-applied immune response modifier effective in the treatment of external genital and perianal warts (complete clearing of genital warts in >70% of females and >30% of males in 4–16 weeks). Sexual contact should be avoided while the cream is on the skin. It is applied three times per week before normal sleeping hours and is left on the skin for 6 to 10 hours.
Third Line
- •
CO 2 laser ablation
- •
Sinecatechins (Veregen), a botanical drug product, is also effective for treatment of external genital and perianal warts. Formulation is a 15% ointment applied to affected area tid for up to 16 weeks.
- •
Application of trichloroacetic acid or bichloracetic acid 80% to 90% is also effective for external genital warts. A small amount should be applied only to warts and allowed to dry, at which time a white “frosting” develops. This treatment can be repeated weekly if necessary.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
This condition is highly contagious, with 25% to 65% of sexual partners developing it.
- •
Two HPV vaccines (Gardasil, Cervarix) have been licensed in the United States. ACIP recommends routine vaccination with HPV4 or HPV2 for females aged 11 to 12 years and HPV4 for males aged 11 to 12 years. Vaccination is also recommended for females aged 13 to 26 years and for males aged 13 through 21 years who were not vaccinated previously. Males aged 22 through 26 may be vaccinated. ACIP recommends vaccination of men who have sex with men and immunocompromised persons (including those with infection) through age 26 years if not previously vaccinated. The FDA has also approved a 9-Valent HPV vaccine (Gardasil-9) for use in girls and women 9 to 26 years old and boys 9 to 15 years old.
37
Contact Dermatitis (Contact Eczema)
 General Comments
General Comments
Definition
- •
Contact dermatitis is an acute or chronic skin inflammation or dermatitis resulting from exposure to substances in the environment. It can be subdivided into “irritant” contact dermatitis (nonimmunologic physical and chemical alteration of the epidermis) and “allergic” contact dermatitis (delayed hypersensitivity reaction).
Etiology
- •
Irritant contact dermatitis: cement (construction workers), rubber, ragweed, malathion (farmers), orange and lemon peels (chefs, bartenders), hair tints, shampoos (beauticians), soaps, rubber gloves (medical, surgical personnel), depilatories ( Fig. 3.81 ) .

FIG. 3.81
Acute irritant contact from improper use of a depilatory cream.
(Fitzsimons Army Medical Center Collection)
- •
Allergic contact dermatitis: poison ivy, poison oak, poison sumac, belt buckles ( Fig. 3.82 ) , other nickel (jewelry), oils, balsam of Peru (hand and face dermatitis), neomycin ( Fig. 3.83 ) , formaldehyde (cosmetics), acrylic in adhesive tape, rubber (shoe dermatitis) ( Fig. 3.84 ).

FIG. 3.82
Classic, erythematous, pruritic confluent papules of contact dermatitis caused by a nickel allergy from a metal belt buckle.
(William Weston Collection)

FIG. 3.83
Allergic contact dermatitis due to neomycin presenting a pruritic, erythematous dermatitis with erosions.
(Joanna Burch Collection)

FIG. 3.84
Chronic, allergic contact dermatitis to components of a lumberjack’s boots.
(John Aeling Collection)
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Mild exposure may result in dryness, erythema, and fissuring of the affected area (e.g., hand involvement in irritant dermatitis caused by exposure to soap; genital area involvement in irritant dermatitis caused by prolonged exposure to wet diapers).
- •
Poison ivy dermatitis can present with vesicles and blisters; linear lesions (as a result of dragging of the resins over the surface of the skin by scratching) are a classic presentation.
Physical Examination
- •
The pattern of lesions is asymmetric; itching, burning, and stinging may be present.
- •
The involved areas are erythematous, warm to touch, and swollen and may be confused with cellulitis.
Diagnostic Tests
- •
A diagnosis of contact dermatitis is made from the history and distribution of lesions and is confirmed by patch testing to the suspected allergen ( Fig. 3.85 ).

FIG. 3.85
Bullous patch test results to thiuram, which is found in rubber. The patient also has multiple other weaker positive patch test results.
(Fitzsimons Army Medical Center Collection)
- •
Patch testing is useful to confirm the diagnosis of contact dermatitis; it is indicated particularly when inflammation persists despite appropriate topical therapy and avoidance of suspected causative agent. Patch testing should not be used for irritant contact dermatitis because this is a nonimmunologic-mediated inflammatory reaction.
- •
Dermoscopy and microscopy may be useful when suspecting scabies.
- •
A potassium hydroxide (KOH) preparation may be useful if suspecting tinea or Candida infection.
 Differential Diagnosis
Differential Diagnosis
- •
Impetigo
- •
Lichen simplex chronicus
- •
Atopic dermatitis
- •
Nummular eczema
- •
Seborrheic dermatitis
- •
Psoriasis
- •
Scabies
- •
Insect bites
- •
Sunburn
- •
Candidiasis
 Treatment
Treatment
First Line
- •
Removal of the irritant substance by washing the skin with plain water or mild soap within 15 minutes of exposure is helpful in patients with poison ivy, poison oak, or poison sumac dermatitis.
- •
Patients with shoe allergy should change their socks at least once a day; use of aluminum chloride hexahydrate in a 20% solution QHS will also help control perspiration.
- •
Use hypoallergenic surgical gloves in patients with rubber and surgical glove allergy.
- •
Cold or cool water compresses for 20 to 30 minutes five to six times a day for the initial 72 hours are effective during the acute blistering stage.
- •
Colloidal oatmeal (Aveeno) baths can also provide symptomatic relief.
- •
Patients with mild to moderate erythema may respond to topical steroid ointments or creams.
- •
Oral antihistamines will control pruritus, especially at night. Calamine lotion is also useful for pruritus; however, it can lead to excessive drying.
Second Line
- •
Oral corticosteroids are generally reserved for severe, widespread dermatitis.
- •
Intramuscular steroids are used for severe reactions and in patients requiring systemic corticosteroids but unable to tolerate them by mouth.
Third Line
- •
Phototherapy
- •
Azathioprine
- •
Cyclosporine
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Chemical irritants (e.g., cutting fluids used in machining, solvents) account for most cases of irritant contact dermatitis. Occupational skin diseases are second only to traumatic injuries as the most common types of occupational disease.
38
Corns (Clavus)
 General Comments
General Comments
Definition
- •
A corn is a circumscribed horny, conical thickening (also known as clavus) that forms over or under weight-bearing surfaces.
Etiology
- •
Mechanically induced lesions due to repetitive pressure or friction
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Pain when pressure is applied to central core
Physical Examination
- •
Plantar corns have a hard, painful, well-demarcated central core ( Fig. 3.86 ).

FIG. 3.86
Clavus with central, hard, keratotic core.
(From Habif TP, Clinical dermatology, 6th ed. Philadelphia: Saunders, 2016, Figure 12-21A, pages 448–486.)
Diagnostic Tests
- •
None
 Differential Diagnosis
Differential Diagnosis
- •
Callus
- •
Plantar wart
- •
Pressure ulcer
- •
Black heel
- •
Friction blister
 Treatment
Treatment
First Line
- •
Corrective footwear to reduce pressure or friction
- •
Application of a ring of soft felt wadding around the region of the corn
- •
Soaking the feet in hot water and paring of surface with scalpel blade or pumice stone followed by application of 40% salicylic acid plaster
Second Line
- •
Surgical correction of the osseous deformity creating the mechanical pressure point
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Frequently, a bony spur or exostosis is present beneath both hard and soft corns.
39
Cryoglobulinemia
 General Comments
General Comments
Definition
- •
Cryoglobulins are immunoglobulins that precipitate at low temperatures (4° C) and that resolve with rewarming.
Etiology
- •
Cryoglobulins may be divided into three classes:
- 1.
Type I—composed solely of monoclonal immunoglobulin (either kappa or lambda) and usually associated with lymphoproliferative disorders (multiple myeloma, Waldenstrom’s macroglobulinemia)
- 2.
Type II (mixed) cryoglobulin—composed of monoclonal (usually IgM) immunoglobulin
- 3.
Type III (polyclonal) cryoglobulin—composed of immunoglobulins IgG and IgM
- 1.
- •
The last two subtypes (mixed cryoglobulins) function as immune complexes and clinical manifestations are due, at least in part, to allergic vasculitis.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
The eponym Meltzer’s triad has been applied to the combined features of purpura, arthralgias, and weakness, which are often present.
- •
Cutaneous manifestations are common to all classes of cryoglobulinemia and are often the presenting complaint.
- •
Type I cryoglobulinemia is usually characterized by purpuric lesions, including inflammatory macules and papules on the extremities, accompanied by foci of ulceration.
- •
Mixed cryoglobulinemia is characterized by joint involvement (arthralgia and arthritis), Raynaud’s phenomenon, fever, purpura, weakness, renal involvement, hepatosplenomegaly, necrosis of extremities, and general vasculitis. Cutaneous manifestations include palpable purpura, inflammatory macules and papules, necrotizing vasculitis, and, occasionally, cold urticaria. Renal involvement may be identified by proteinuria, hematuria, and red cell casts. Patients may also have polyneuropathies.
Physical Examination
- •
Purpura ( Fig. 3.87 ) is the most common initial sign.

FIG. 3.87
Purpura and ulceration in a patient with monoclonal cryoglobulinemia due to an underlying chronic lymphocytic leukemia.
(Fitzsimons Army Medical Center Collection)
- •
Additional features may include livedo reticularis, Raynaud’s phenomenon, scarring, ulceration, and infarction, which particularly affects the digits, ears, and nose.
Diagnostic Tests
- •
Serum cryoglobulin level
- •
Skin biopsy
 Differential Diagnosis
Differential Diagnosis
- •
Serum sickness
- •
Antiphospholipid antibody syndrome
- •
Sarcoidosis
- •
Waldenstrom’s hyperglobulinemia
- •
Septic vasculitis
- •
Polyarteritis nodosa
- •
Goodpasture syndrome
- •
SLE
 Treatment
Treatment
First Line
- •
Elimination of triggers by minimizing cold exposure
- •
Systemic corticosteroids
- •
NSAIDs
Second Line
- •
Rituximab
- •
Azathioprine
- •
Mycophenolate mofetil
- •
Dapsone
Third Line
- •
Methotrexate
- •
Cyclophosphamide
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Cryoglobulins may be associated with hepatitis C, hepatitis B, SLE, lymphoreticular neoplasms, and infective processes (e.g., infective endocarditis).
- •
Prognosis is variable. Renal involvement, which occurs in 50% of cases, is associated with high morbidity and mortality.
40
Cutaneous T Cell Lymphomas (CTCLs)
 General Comments
General Comments
Definition
- •
CTCL encompasses a large group of lymphomatous neoplasms of T helper cells. They are initially present in the skin but may later involve lymph nodes and peripheral blood cells. Its most common form is mycosis fungoides, which is covered separately in more detail in this book. Most dermatologists use the WHO-EORTC classification for cutaneous lymphoma.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation
- •
Biopsy and histologic examination. Once an atypical lymphoid is identified, the initial immunoperoxidase studies usually include CD3 (T cell) or CD8 (B cell) or other markers to establish the cell line. Once identified as being of T cell origin, the next step in evaluation is to do a panel of immunoperoxidase studies (e.g., CD4, CD5, CD8, CD30).
- •
Important types of T-cell lymphoma that may present in the skin include:
- •
Sezary syndrome (SS) is characterized clinically by pruritic erythroderma ( Fig. 3.88 ) , generalized lymphadenopathy, and the presence of circulating malignant T lymphocytes with cerebriform morphology. Diagnostic criteria include the presence of the same monoclonal population of T lymphocytes within the peripheral blood and the skin; of at least 1000 circulating Sézary cells/mm 3 and an expanded CD4+ population in the peripheral blood resulting in a markedly increased CD4:CD8 ratio; of an increased population of CD4+/CD7 cells or CD4+/CD26 in the peripheral blood; and of the loss of T-cell antigens such as CD2, CD3, and CD5.

FIG. 3.88
Sézary syndrome presenting as erythroderma.
(Fitzsimons Army Medical Center Collection)
- •
Primary cutaneous anaplastic large cell lymphoma is type CD30+ cutaneous T-cell lymphoma that typically presents as a single or several skin lesions that have a tendency to ulcerate (50%), spontaneously regress (50%), and relapse. Lesions are usually firm, red to violaceous tumors up to 10 cm in diameter ( Fig. 3.89 ). Tumors may grow in a matter of weeks. They are rare in children and occur with slightly greater frequency in males.

FIG. 3.89
Primary cutaneous, anaplastic large cell lymphoma presenting as papules and nodules that frequently become necrotic.
(Fitzsimons Army Medical Center Collection)
- •
Lymphomatoid papulosis is a chronic CD30+ proliferative disorder characterized by papules, necrotic papules, and/or nodular lesions that demonstrate a malignant histologic appearance; however, a benign clinical course with individual lesions may demonstrate spontaneous resolution over a period of 1 to 4 months. New crops of lesions may continue to appear for years or decades.
- •
Subcutaneous panniculitis-like T-cell lymphoma most commonly presents in young adults who present with subcutaneous nodules, usually on the lower extremities. The alpha/beta phenotype is generally associated with indolent disease, and gamma/delta lymphoma, which is associated with a more aggressive course, is now considered a separate provisional entity in the WHO classification. Weight loss, fever, and fatigue are common.
- •
Primary cutaneous peripheral T-cell lymphoma, not otherwise specified is a heterogeneous group of T-cell lymphomas that do not fit into the classic well-defined malignancies.
- •
41
Cutis Laxa
 General Comments
General Comments
Definition
- •
Cutis laxa is a genetic disorder of elastic fibers resulting in decreased or absent elastic fibers in the skin.
Etiology
- •
Defects in at least six genes will produce congenital cutis laxa.
- •
Less commonly, it may be acquired and occur in association with paraneoplastic disorders, or following long-term penicillamine therapy.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
The affected individual appears much older than chronologic age.
- •
Associated involvement of internal organs may result in GI diverticula, hernias, emphysema, aortic aneurysms, and ligamentous laxity.
- •
Severe involvement of internal organs may be fatal.
Physical Examination
- •
Skin is inelastic, loose, wrinkling, and sagging ( Figs. 3.90 and 3.91 ).

FIG. 3.90
Cutis laxa is characterized by skin that is loose, hanging, and lacking in elasticity as seen in this newborn. The patient developed emphysema leading to cor pulmonale and died in the first few months of life.
(William Weston Collection)

FIG. 3.91
Severe decrease in elastic recoil of the skin in this patient with cutis laxa.
Diagnostic Tests
- •
A biopsy of skin will demonstrate a decrease in or absence of elastic fibers with special stains.
 Differential Diagnosis
Differential Diagnosis
- •
Anetoderma (localized area of lax skin, often with herniation of underlying tissues)
- •
Morphea
- •
Atrophoderma (disorders characterized by a depression in the skin’s surface)
- •
Pseudoxanthoma elasticum
- •
Ehlers-Danlos syndrome
- •
Marfan syndrome
 Treatment
Treatment
- •
There is no effective treatment.
- •
Reconstructive surgery may be attempted.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Surgical approaches are generally disappointing and not permanent.
42
Cylindroma
 General Comments
General Comments
Definition
- •
Cylindroma is a skin lesion often found on the scalp and also known as a “turban tumor” or “tomato tumor” due to its appearance.
Etiology
- •
Unknown
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Lesions may be solitary (most common) ( Fig. 3.92 ) or multiple ( Fig. 3.93 ).

FIG. 3.92
Large solitary cylindromas presenting as a benign, firm, rubbery nodules on the head.
(Joanna Burch Collection)

FIG. 3.93
This patient developed multiple facial cylindromas beginning in adolescence, which is consistent with an autosomal dominant pattern of inheritance.
- •
Lesions are most often found on the scalp, face, and neck.
Physical Examination
- •
Purplish to red nodule(s) with a smooth surface are present.
- •
Prominent surface vessels may be present.
- •
A rounded mass is seen, and skin may appear stretched.
Diagnostic Tests
- •
Biopsy of lesion
 Differential Diagnosis
Differential Diagnosis
- •
Basal cell carcinoma
- •
Pilar cyst
- •
Pilomatricoma
- •
Follicular neoplasm
- •
Eccrine spiradenoma
 Treatment
Treatment
First Line
- •
Excision of lesion
Second Line
- •
CO 2 laser ablation
 Clinical Pearl(s)
Clinical Pearl(s)
- •
There is a familial association with multiple facial trichoepitheliomas (Spiegler-Brooke syndrome).
43
Cysticercosis
 General Comments
General Comments
Definition
- •
Cysticercosis is an infection caused by the tissue deposition of larval forms of the pork tapeworm Taenia solium.
Etiology
- •
Humans acquire cysticercosis through fecal-oral transmission of T. solium eggs from human tapeworm carriers, often by ingesting tapeworm eggs or cysts in contaminated food or water. The eggs hatch in the gastrointestinal tract, and larvae migrate hematogenously to tissues and then encyst, forming cysticerci. T. solium cysts, or cysticerci, may accumulate in any tissue, including the eyes, spinal cord, skin, muscle, heart, and brain. Central nervous system involvement is common and is known as neurocysticercosis.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Following ingestion of T. solium eggs or cysts, humans may remain asymptomatic for several years.
- •
The symptoms are varied and depend on the location of cysticerci. Cysticerci in muscles and skin may form “cold” nodules, which are usually asymptomatic but may calcify.
Physical Examination
- •
The cutaneous manifestations consist primarily of subcutaneous nodules.
Diagnostic Tests
- •
Definitive diagnosis is based on the histopathologic demonstration of cysticerci in the tissue involved ( Fig. 3.94 ).
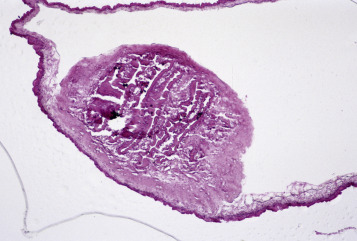
FIG. 3.94
Section through the scolex of a cystericercus removed from the back of an immigrant from Mexico. The patient had presented to the emergency room with a seizure.
(Fitzsimons Army Medical Center Collection)
- •
Peripheral eosinophilia is absent.
 Differential Diagnosis
Differential Diagnosis
- •
Epidermoid cysts
- •
Sarcoidosis
- •
Toxoplasmosis
- •
CNS neoplasm
- •
Tuberculosis
 Treatment
Treatment
First Line
- •
Asymptomatic cysticercosis: There is no evidence that administering antiparasitic therapy is beneficial.
- •
Symptomatic cysticercosis: Patients with active lesions, with evidence of surrounding edema, and/or inflammation generally warrant treatment with antiparasitics (albendazole, praziquantel), corticosteroids, and anticonvulsants.
Second Line
- •
Surgical excision can remove solitary lesions.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Undercooked pork is the most commonly identified food source.
44
Darier’s Disease
 General Comments
General Comments
Definition
- •
Darier’s disease is a rare skin disorder characterized by abnormal keratinocyte adhesion.
Etiology
- •
Darier’s disease is a dominantly inherited disorder of keratinization caused by mutations in the ATP2A2 gene.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Lesions may be induced or exacerbated by stress, heat, sweating, and maceration.
Physical Examination
- •
The nail changes in Darier’s disease include longitudinal red and/or white streaks that terminate in a notch on the free margin of the nail plate, splitting, and subungual hyperkeratosis with associated wedge-shaped onycholysis ( Fig. 3.95 ).

FIG. 3.95
Darier’s disease of the nail presenting a linear red streaks and subungual white hyperkeratotic lesions.
(William Weston Collection)
- •
The skin lesions are often itchy and characterized by greasy, crusted, keratotic yellow-brown papules and plaques found particularly on the scalp, forehead, ears, nasolabial folds, upper chest, back, and supraclavicular fossae.
- •
In some cases the lesions can be photoaccentuated ( Fig. 3.96 ).

FIG. 3.96
Photosensitive Darier’s disease with confluent lesions in photoexposed areas.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
Skin biopsy reveals focal acantholytic dyskeratosis.
 Differential Diagnosis
Differential Diagnosis
- •
Pemphigus foliaceus
- •
Transient acantholytic dermatosis
- •
Seborrheic dermatitis
- •
Follicular eczema
- •
Folliculitis
 Treatment
Treatment
First Line
- •
Emollients, cool cotton clothing
- •
Topical retinoids (tretinoin 0.025% cream HS)
Second Line
- •
Oral retinoids (isotretinoin 0.3-0.5 mg/kg QD)
- •
Topical tazarotene gel
Third Line
- •
Topical 5-fluorouracil
- •
Cyclosporine
- •
Oral contraceptives
- •
Laser
- •
Dermabrasion
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Patients with Darier’s disease are susceptible to bacterial (particularly S. aureus ), dermatophyte, and viral infections.
45
Decubitus Ulcer
 General Comments
General Comments
Definition
- •
Decubitus ulcers (pressure ulcers or bed sores) are defined by any damage to the skin and the underlying tissue or both that results from pressure, friction, or shearing forces.
Etiology
- •
Decubitus ulcers are caused by pressure, friction, or shearing forces that usually occur over bony prominences such as the sacrum or heels.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
All pressure ulcers should be staged according to depth and type of tissue damage (see “ Physical Examination ”).

FIG. 3.97
Stage II decubitus or pressure sore of the great toe with incipient shallow ulcer and necrosis of the dermis as evidenced by black discoloration.

FIG. 3.98
The uppermost decubitus ulcer has caused necrosis to the level of subcutaneous tissue (but not into the underlying fascia) and is assessed as stage III.

FIG. 3.99
Stage IV decubitus ulcer with necrosis extending from skin through subcutaneous tissue, muscle, and finally to bone. Treatment included debridement of necrotic tissue and removal of infected area of sacral bone.

FIG. 3.100
Stage IV ulcer, lateral foot, with dark eschar extending to the level of bone in a bedridden stroke patient.
Physical Examination
| Stage I | Nonblanchable erythema of intact skin or boggy, mushy feeling of skin |
| Stage II | Partial-thickness skin loss involving the epidermis, dermis, or both ( Fig. 3.97 ) |
| Stage III | Full-thickness skin loss involving damage or necrosis of subcutaneous tissue that may extend down to, but not through, underlying fascia or muscle ( Fig. 3.98 ) |
| Stage IV | Full-thickness skin loss with extensive destruction and tissue damage to muscle, bone, or supporting structures (e.g., tendons, joint capsule) ( Figs. 3.99 and 3.100 ) |
Diagnostic Tests
- •
Tests are directed at identifying the cause of risk factors or any complications arising from the pressure ulcer (e.g., abscess or osteomyelitis); cultures of the wound bed are not helpful and should not be performed.
- •
Nutritional laboratory tests may reveal malnutrition.
- •
CBC should be obtained if infection is suspected.
- •
MRI or bone scans may help identify osteomyelitis when clinically suspected.
 Differential Diagnosis
Differential Diagnosis
- •
Venous insufficiency ulcers
- •
Arterio-occlusive ulcers
- •
Diabetic ulcers
- •
Cellulitis
- •
Incontinence associated dermatitis
- •
Neuropathic ulcers
- •
Burns
- •
Contact dermatitis
- •
Pyoderma gangrenosum
- •
Squamous cell carcinoma
- •
Bullous pemphigoid
 Treatment
Treatment
First Line
- •
The area should be cleaned at each dressing change; necrotic tissue should be removed.
- •
Debridement should be performed quickly because it delays wound healing. Whirlpool debridement may be useful.
- •
The wound should be irrigated.
- •
No one dressing or product is clearly superior; dressing should be used to keep the ulcer bed moist and protect it from urine/stool. Hydrocolloid dressings are useful for stage II ulcers. Wet dressings, xerogels, or hydrogels can be used for stage III and IV ulcers. Avoid agents that are cytotoxic to epithelial cells (e.g., iodine, iodophor, sodium hypochlorite, hydrogen peroxide, acetic acid, and alcohol).
- •
Reduce pressure by using a foam mattress, alternating pressure mattress, or dynamic support surface (e.g., low-air-loss bed) and by frequent repositioning (e.g., Q2H).
- •
Correct malnutrition.
- •
Minimize urinary/fecal incontinence.
- •
Use a standardized assessment tool (e.g., Pressure Ulcer Scale for Healing [PUSH] tool) to monitor wound healing on weekly basis.
Second Line
- •
Negative pressure devices (vacuum-assisted closure [VAC] devices) may help for wounds that have significant drainage.
Third Line
- •
Hyperbaric oxygen, ultrasound, and ultraviolet and low-energy radiation are either ineffective or have not been extensively evaluated for efficacy.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The initial manifestation of a decubitus ulcer is erythema (blanchable and nonblanchable).
46
Dermatitis Herpetiformis
 General Comments
General Comments
Definition
- •
Dermatitis herpetiformis (DH) is a chronic skin disorder characterized by an intensely burning, pruritic, vesicular rash.
Etiology
- •
Unknown. Increased incidence in association with HLA DRw3, B8, and DQw2, and in patients with celiac disease.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Pruritic, burning vesicles are seen initially; the vesicles are frequently grouped (hence the name herpetiform ).
- •
It may evolve in time to intensely burning urticarial papules, vesicles, and, rarely, bullae ( Fig. 3.101 ).

FIG. 3.101
Intensely pruritic, grouped vesicles and excoriated papules on a red, inflamed upper arm.
(Fitzsimons Army Medical Center Collection)
- •
Celiac-type permanent-tooth enamel defects are found in 53% of patients.
Physical Examination
- •
Symmetrically distributed vesicles and papules are seen on extensor surfaces, such as elbows, knees, scalp, nuchal area, shoulder, and buttocks, but are rarely found in the mouth.
Diagnostic Tests
- •
Skin biopsy of lesional skin for histologic examination characteristically demonstrates a subepidermal blister with neutrophils in the blister cavity. This pattern, although suggestive of DH, is not specific.
- •
A skin biopsy of uninvolved perilesional skin should be taken for direct immunofluorescence studies. Diagnosis is confirmed by granular or fibrillary IgA deposits along the subepidermal basement membrane ( Fig. 3.102 ). Biopsies should be taken from adjacent normal skin because the diagnostic Ig deposits are usually destroyed by the blistering process.
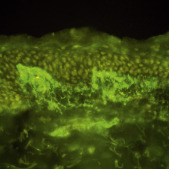
FIG. 3.102
Dermatitis herpetiformis. Direct immunofluorescence of perilesional uninvolved skin showing granular deposits of granular IgA in the dermal papillae.
- •
Circulating antibodies include IgA antiendomysial antibody, IgA antigliadin antibodies, IgA reticulin antibody, and IgA antitissue transglutaminase.
 Differential Diagnosis
Differential Diagnosis
- •
Linear IgA bullous dermatosis (not associated with gluten-sensitive enteropathy)
- •
Herpes simplex infection
- •
Herpes zoster infection
- •
Erythema multiforme
- •
Bullous pemphigoid
- •
Scabies
- •
Arthropod bites
- •
Herpes simplex or zoster
- •
 Treatment
Treatment
First Line
- •
Adherence to a gluten-free diet has been associated with sustained remission of DH. Spontaneous remission of DH in patients on a normal diet can occur in up to 15% of cases.
- •
Dapsone
Second Line
- •
Sulfapyridine
- •
Systemic corticosteroids
Third Line
- •
Tetracycline and nicotinamide
- •
Cyclosporine
- •
Colchicine
 Clinical Pearl(s)
Clinical Pearl(s)
- •
DH is strongly associated with gluten-sensitive enteropathy. Up to 70% of patients with DH will have gastrointestinal symptoms, whereas approximately 10% of patients with celiac sprue will have DH.
47
Dermatofibroma
 General Comments
General Comments
Definition
- •
Dermatofibroma is an extremely common benign, slow-growing, asymptomatic dermal papule, also known as histiocytoma.
Etiology
- •
Unknown. The condition may occur spontaneously.
- •
Dermatofibroma may be associated with history of trauma (ruptured cyst, insect bite).
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Papules are most often found on extremities (lower more commonly than upper) and scapulas.
- •
Papules are generally not tender but may be mildly tender on palpation.
- •
The condition is usually asymptomatic, but localized pruritus may be present when the lesion is initially detected.
Physical Examination
- •
Discrete firm dermal papules are 3 to 10 mm in diameter.
- •
Papules are flesh colored to violaceous to brown ( Fig. 3.103 ).
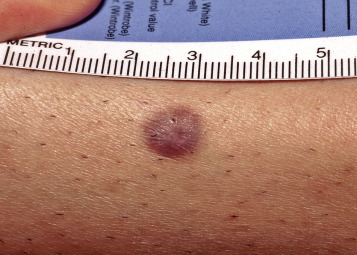
FIG. 3.103
Dermatofibroma. Asymptomatic, dome-configured, 5-mm, violaceous-brown, firm nodule.
(William Weston Collection)
- •
The lesion dimples into the surrounding skin with lateral pinching.
Diagnostic Tests
- •
Biopsy of pigmented lesions to rule out melanoma
 Differential Diagnosis
Differential Diagnosis
- •
Insect bite
- •
Foreign body reaction
- •
Angioma
- •
Melanoma
- •
Wart
- •
Prurigo nodularis
- •
Basal cell carcinoma
- •
Scar
- •
Keloid
- •
Nevus
 Treatment
Treatment
First Line
- •
This is a benign neoplasm that does not require treatment.
Second Line
- •
Surgical excision with primary closure can be performed for symptomatic lesions.
- •
Surgery for cosmetic reasons is best avoided because the scar from surgery may be more prominent than original lesion.
Third Line
- •
Intralesional corticosteroids have been used with variable results
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Eruption of large numbers of dermatofibromas can be seen with HIV infection and SLE.
48
Dermatographism
 General Comments
General Comments
Definition
- •
Dermatographism is a physical urticaria manifesting with briefly lasting linear wheals at the site of stroking of the skin ( Fig. 3.104 ).

FIG. 3.104
Dermatographism is caused by the release of excessive amount of histamine in certain predisposed individuals following gentle “writing” on the skin.
(From Fitzpatrick J and Morelli J, Dermatology Secrets Plus , 5th ed. Philadelphia: Elsevier, 2016.)
Etiology
- •
Unknown. The condition may be associated with emotional upset, viral infections, drug reactions (antibiotics, postscabies treatment), or extreme temperature changes.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
There is pruritus and scratching of the involved skin.
- •
Attacks may last from a few minutes to several hours.
Physical Examination
- •
Linear wheals and redness are seen at the site of stroking of the skin.
Diagnostic Tests
- •
Stroking of the skin with a tongue blade will elicit whealing within a few minutes.
 Differential Diagnosis
Differential Diagnosis
- •
Cholinergic urticaria
- •
Solar urticaria
- •
Heat urticaria
- •
Exercise-induced urticaria
- •
Cold urticaria
- •
Lupus
- •
Aquagenic urticaria
- •
Polymorphous light eruption
 Treatment
Treatment
First Line
- •
Elimination of potential offending agent
Second Line
- •
Antihistamines
Third Line
- •
H2 blockers
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Although H2 blockers are sometimes added to antihistamines to treat dermatographism, some H2 blockers, such as famotidine, have been reported to cause dermatographism.
49
Dermatomyositis
 General Comments
General Comments
Definition
- •
Dermatomyositis is an inflammatory eruption of the skin associated with myositis.
Etiology
- •
The cause is unknown, but an autoimmune etiology is suspected.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Proximal muscle weakness, generalized pruritus, fatigue
- •
Itching or scaling of scalp
- •
Dysphagia
Physical Examination
- •
The two most important clinical findings are the presence of a violaceous or faint lilac “heliotrope” discoloration around eyes ( Fig. 3.105 ) and erythema of the elbows, knees, and dorsum of phalanges (Gottron’s sign) ( Fig. 3.106 ). When lesions of the extensor knuckles evolve into flat-topped papules on the fingers, these are referred to as Gottron’s papules ( Fig. 3.107 ).

FIG. 3.105
Heliotrope eyelids of dermatomyositis are a characteristic clinical clue to the diagnosis.
(Fitzsimons Army Medical Center Collection)

FIG. 3.106
Erythema over the elbows and knees is pattern of erythema suggestive of dermatomyositis. It is sometimes referred to as Gottron’s sign.
(Fitzsimons Army Medical Center Collection)

FIG. 3.107
Flat-topped papules over the knuckles are known as Gottron’s papules. Although not specific, this is strongly supportive of a diagnosis of dermatomyositis.
(William Weston Collection)
- •
Lesions may present around neck and upper shoulders (“shawl” sign).
- •
Malar and eyelid edema and erythema
- •
Telangiectasia of nailfolds
- •
Calcinosis of skin (especially in juvenile disease) may occur late in the disease ( Fig. 3.108 ).

FIG. 3.108
Dystrophic calcinosis cutis on the elbow in a patient with dermatomyositis. This is usually a late cutaneous finding.
(William Weston Collection)
- •
Proximal muscle weakness
Diagnostic Tests
- •
Skin biopsy
- •
Muscle biopsy
- •
CPK, serum aldolase
- •
Presence of Jo-1 antibodies correlates with high risk for myositis, pulmonary disease, and arthritis
- •
Anti-MDA-5, anti-Mi-2, Anti-TIF1, and anti-NXP-2 (implicated in cancer-associated dermatomyositis)
- •
Electromyography (EMG)
- •
CT of chest, abdomen, and pelvis to screen for underlying neoplasm (e.g., ovarian cancer)
 Differential Diagnosis
Differential Diagnosis
- •
Lupus
- •
Scleroderma
- •
Sarcoidosis
- •
Lichen planus
- •
Trichinosis
- •
Drug eruption
- •
Psoriasis
- •
Mycosis fungoides
- •
Toxoplasmosis
 Treatment
Treatment
First Line
- •
Cutaneous disease: sunscreens, topical corticosteroids, topical pimecrolimus or tacrolimus, antimalarials (hydroxychloroquine or chloroquine)
- •
Muscle disease: systemic corticosteroids, immunosuppressants (methotrexate, azathioprine)
Second Line
- •
Cutaneous disease: methotrexate, mycophenolate, IVIG
- •
Muscle disease: mycophenolate, cyclosporine, cyclophosphamide, IVIG
Third Line
- •
Dapsone for cutaneous disease; diltiazem for calcinosis; infliximab, etanercept
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Approximately 25% to 40% of patients with dermatomyositis have an underlying malignancy.
- •
Removal of underlying malignancy (when present) may improve dermatomyositis manifestations.
50
Dermatosis Papulosa Nigra
 General Comments
General Comments
Definition
- •
Black-brown papules found on the face
Etiology
- •
May represent a type of seborrheic keratosis
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
It is most common among young and middle-aged black females (average age of onset is 22 years).
- •
There is a family predisposition and female predisposition.
Physical Examination
- •
Two to 3 mm smooth, dome-shaped brown or black stuck-on papules seen on face, especially near the eyes ( Fig. 3.109 )

FIG. 3.109
Dermatosis papulosa nigra. Numerous small papules below and lateral to the eye.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
None
 Differential Diagnosis
Differential Diagnosis
- •
Seborrheic keratosis
- •
Melanoma
- •
Actinic keratosis
- •
Epidermal nevus
- •
Syringoma
 Treatment
Treatment
First Line
- •
Observation
Second Line
- •
Snipping lesions off with scissors, curettage, or cryotherapy of lesions.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
White, hypopigmented scarring may develop following treatment.
51
Dermoid Cyst
 General Comments
General Comments
Definition
- •
Dermoid cysts are congenital lesions resulting from sequestration of cutaneous tissues along embryonal lines of closure.
Etiology
- •
Unknown
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Generally asymptomatic
Physical Examination
- •
The most common clinical appearance is that of a single, nontender, small, subcutaneous nodule at birth on the lateral aspect of the upper eyelid ( Fig. 3.110 ).

FIG. 3.110
Dermoid cyst. Note the cystic swelling lateral and above the eye in an infant. This is a characteristic location for this hamartoma.
(William Weston Collection)
- •
Other potential sites of dermoid cysts include the midline of the neck, nasal root, forehead, mastoid area, and scalp. The last is a particularly important site because the lesion may occasionally show intracranial extension (dumbbell dermoid).
Diagnostic Tests
- •
Preoperative imaging of lesions on the nose, midline scalp, or posterior axis can exclude CNS extension.
 Differential Diagnosis
Differential Diagnosis
- •
Epidermoid cyst
- •
Nevus sebaceus
- •
Enlarged lymph node
- •
Pilomatricoma
 Treatment
Treatment
- •
Clinical observation only
- •
Surgical excision
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Dermoid cysts on the nose or midline scalp have a higher likelihood of intracranial extension than those in periocular locations.
52
Discoid Lupus Erythematosus
 General Comments
General Comments
Definition
- •
Discoid lupus erythematosus (DLE) is a chronic inflammatory autoimmune skin disorder. It is sometimes associated with systemic lupus erythematosus (SLE).
Etiology
- •
DLE is an immune complex–mediated disorder.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
DLE manifests with the appearance of single or multiple asymptomatic plaques ( Fig. 3.111 ).

FIG. 3.111
Fixed, indurated, erythematous scaly plaques in photodistributed areas of the face.
(John Aeling Collection)
- •
Alopecia can occur and may produce a permanent scarring alopecia ( Fig. 3.112 ).

FIG. 3.112
Extensive scarring alopecia with dyspigmentation in discoid lupus erythematosus.
(Fitzsimons Army Medical Center Collection)
- •
Urticaria is present in 5% of cases.
- •
DLE may be associated with other criteria for SLE (e.g., oral ulcers, arthritis, pleuritis, pericarditis).
Physical Examination
- •
Anatomic distribution: commonly involves the scalp, face, and ears, especially the conchal bowl ( Fig. 3.113 ) , but involvement is not limited to these areas

FIG. 3.113
Red, scaly plaque with white atrophic area in the conchal bowl. This is a characteristic site of discoid lupus erythematosus.
(Fitzsimons Army Medical Center Collection)
- •
Lesion configuration: irregularly grouped
- •
Lesion morphology:
- •
Plaque lesions with scale
- •
Follicular plugging
- •
Atrophy
- •
Scarring
- •
Telangiectasia
- •
- •
Color: red to violaceous
- •
Hyperpigmentation or hypopigmentation
Diagnostic Tests
- •
Skin biopsy for H&E
- •
Skin biopsy of lesional skin for direct immunofluorescence often demonstrates a linear granular deposition of multiple immunoreactants (IgG, IgA, C3, fibrin) ( Fig. 3.114 ).
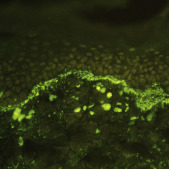
FIG. 3.114
Direct immunofluorescent study of lesional skin demonstrating linear granular C1q along the basement membrane zone. This patient also had deposits of IgG, IgM, C3, and fibrin.
(Fitzsimons Army Medical Center Collection)
 Differential Diagnosis
Differential Diagnosis
- •
Psoriasis
- •
Lichen planus
- •
Secondary syphilis
- •
Superficial fungal infections
- •
Photosensitivity eruption
- •
Sarcoidosis
- •
Subacute cutaneous lupus erythematosus
- •
Rosacea
- •
Keratoacanthoma
- •
Actinic keratosis
- •
Dermatomyositis
 Treatment
Treatment
First Line
- •
Sunscreens
- •
Topical steroids: intermediate rather than high potency should be used on areas such as the face
- •
Intralesional steroids
Second Line
- •
Hydroxychloroquine
- •
Dapsone
- •
Isotretinoin
Third Line
- •
Methotrexate
- •
Thalidomide
- •
Azathioprine
- •
Mycophenolate
 Clinical Pearl(s)
Clinical Pearl(s)
- •
DLE is more common in females, with a peak incidence in the fourth decade of life.
- •
Approximately 10% to 20% of patients with SLE will also have discoid lupus.
- •
Involvement of the conchal bowl is a characteristic site for DLE.
53
Drug Eruptions
 General Comments
General Comments
Definition
- •
Generally, drug eruptions are morbilliform- or urticarial-type reactions to drug therapy. Drug eruptions are the most commonly encountered adverse drug reactions. Patients who have infectious mononucleosis are particularly at risk of developing an exanthematous reaction after therapy with ampicillin or amoxicillin.
Etiology
- •
The mechanism may be immunologic or nonimmunologic. Drug eruptions most commonly develop within 1 to 2 weeks of starting the drug.
- •
Penicillins, sulfonamides, trimethoprim, and phenytoin are frequently implicated.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
In addition to the rash, pruritus, low-grade fever, and eosinophilia are sometimes present.
- •
The eruption is often morbilliform ( Fig. 3.115 ) and symmetrical and usually presents on the trunk and extremities or sites of pressure and trauma.

FIG. 3.115
Morbilliform eruption due to ampicillin in a child.
(Fitzsimons Army Medical Center Collection)
Physical Examination
- •
Erythematous macules and papules are seen that, with progression, may become confluent into red plaques or even acquire gyrate/polycyclic features ( Fig. 3.116 ).

FIG. 3.116
Gyrate and reticulated drug eruption due to cefaclor.
(Fitzsimons Army Medical Center Collection)
- •
Generalized pruritic urticarial reactions in addition to medications ( Fig. 3.117 ) are common after ingestion of shellfish.

FIG. 3.117
Urticaria secondary to ampicillin a child.
(Fitzsimons Army Medical Center Collection)
- •
More severe manifestations may include erythema multiforme, toxic epidermal necrolysis reactions, and exfoliative erythroderma and vessel-necrotizing vasculitis.
Diagnostic Tests
- •
No tests are necessary for morbilliform or urticarial reactions.
 Differential Diagnosis
Differential Diagnosis
- •
Scarlet fever
- •
Measles
- •
Rubella
- •
Viral exanthem such as enterovirus, echovirus, cytomegalovirus
- •
Kawasaki syndrome
- •
Juvenile rheumatoid arthritis
- •
Secondary syphilis
- •
Primary HIV disease
 Treatment
Treatment
First Line
- •
Removal of offending agent
- •
Oral antihistamines
- •
Cooling lotions
Second Line
- •
Systemic corticosteroids
Third Line
- •
Epinephrine may be needed for severe drug-induced urticaria.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Cutaneous drug reactions are seen in 3% to 5% of hospitalized patients, most of whom are on multiple medications.
54
Dyshidrotic Eczema (Pompholyx)
 General Comments
General Comments
Definition
- •
Dyshidrotic eczema is a recurrent, pruritic, vesicular eruption of the palms, soles, or digits.
Etiology
- •
Unknown. Atopy, heat, and emotional stress may be contributing factors. An increased incidence of allergic contact dermatitis to nickel has also been reported.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Sudden eruptions of symmetric vesicles appear on the palms of hands and plantar feet.
- •
Intense pruritus often precedes and accompanies the eruptions.
- •
Because of the increased thickness of the keratin layer at these sites, the vesicles appear as small, pale papules before rupturing.
- •
With the passage of time, the affected parts may show scaling and cracking.
- •
Slow resolution of vesicles occurs over 2- to 3-week period.
Physical Examination
- •
Fluid-filled vesicles 2 to 5 mm in diameter can be seen on the palms, soles, and digits ( Fig. 3.118 ).

FIG. 3.118
Acute severe dyshidrotic hand dermatitis.
(Fitzsimons Army Medical Center Collection)
- •
Rings of scale, peeling, and brown spots may all be present from previous vesiculation.
Diagnostic Tests
- •
Specific investigations include patch testing for contact allergens, potassium hydroxide preparation, and bacterial culture.
 Differential Diagnosis
Differential Diagnosis
- •
Contact dermatitis
- •
Pustular psoriasis
- •
Inflammatory tinea
- •
Bullous pemphigoid
- •
Id reaction
 Treatment
Treatment
First Line
- •
Cold wet dressings
- •
Topical corticosteroids
- •
Oral antihistamines to alleviate pruritus
Second Line
- •
Oral corticosteroids
Third Line
- •
Phototherapy with NBUVB or bath PUVA
- •
Azathioprine
- •
Methotrexate
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Increased sweating often accompanies and may worsen this disorder.
55
Ecthyma Gangrenosum
 General Comments
General Comments
Definition
- •
Deep necrotic ulcers that are usually seen in malnourished, immunocompromised, and debilitated hosts
Etiology
- •
Ecthyma gangrenosum most commonly occurs when patients develop low white blood cell counts. While most commonly due to Pseudomonas aeroginosa , other bacteria including Proteus species, Escherichia coli , and Staphylococcus species have been implicated.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Gradual development of edematous plaques, which evolve into hemorrhagic bullae and necrotic ulcers ( Fig. 3.119 )

FIG. 3.119
Painful, tender eschar surrounded by erythema in an immunocompromised patient. Cultures demonstrate a polymicrobial sepsis.
(Fitzsimons Army Medical Center Collection)
Physical Examination
- •
Deep necrotic ulcers are often seen on lower extremities.
Diagnostic Tests
- •
Wound cultures may yield mixed bacterial flora.
- •
Blood cultures
 Differential Diagnosis
Differential Diagnosis
- •
Necrotizing fasciitis
- •
Pyoderma gangrenosum
- •
Trauma
- •
Nocardiosis, sporotrichosis
 Treatment
Treatment
- •
Systemic antipseudomonal antibiotics
- •
Nutritional support
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The mortality rate is nearly 100% if left untreated.
56
Eczema Herpeticum
 General Comments
General Comments
Definition
- •
Eczema herpeticum, also known as Kapsiform varicelliform eruption, is a widespread infection due to herpes simplex virus that occurs in patients with atopic dermatitis.
Etiology
- •
Herpes simplex virus
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
This condition is most common in areas of atopic dermatitis, often the face ( Fig. 3.120 ).

FIG. 3.120
Acute onset of a burning, vesicular, rapidly spreading facial eruption causing facial edema and inflammation in this patient with atopic dermatitis.
(Fitzsimons Army Medical Center Collection)
- •
Secondary bacterial infections may occur.
Physical Examination
- •
Umbilicated vesicles and pustules in various stages
- •
“Punched out” hemorrhagic ulcers
- •
Crusts may coalesce and form eroded plaques ( Fig. 3.121 ).

FIG. 3.121
Patient atopic dermatitis with resolving eczema herpeticum that healed without scarring. This patient had a history of a previous episode and was placed on suppressive antiviral therapy.
(Fitzsimons Army Medical Center Collection)
- •
Secondary bacterial infections may occur.
Diagnostic Tests
- •
Herpesvirus cultures of fluid from intact vesicles
 Differential Diagnosis
Differential Diagnosis
- •
Impetigo
- •
Contact dermatitis
- •
Pemphigus
- •
Dermatitis herpetiformis
- •
Bullous pemphigoid
 Treatment
Treatment
- •
Systemic antiviral agents (acyclovir, valacyclovir, famciclovir)
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Eczema herpeticum occurs more commonly in corticosteroid-treated skin and in immunocompromised hosts.
57
Ehlers-Danlos Syndrome
 General Comments
General Comments
Definition
- •
Ehlers-Danlos syndrome (EDS) is a group of inherited, clinically variable, and genetically heterogeneous connective tissue disorders. EDS is characterized by skin hyperextensibility, skin fragility, joint laxity, and joint hyperextensibility.
Etiology
- •
Defects of collagen in extracellular matrices of multiple tissues (skin, tendons, blood vessels, and viscera) underlie all forms of EDS.
- •
Classic EDS is associated with defects in type V collagen, corresponding to mutations of the COL5A genes.
- •
Vascular EDS involves a deficiency in type III collagen, and several studies suggest that mutations of gene COL3A1 lead to this deficiency.
- •
Arthrochalasia EDS results from a defect in type I collagen, caused by mutations in the COL1A1 and COL1A2 genes.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Diagnosis is based solely on clinical criteria. It is important to identify patients with vascular EDS because of the grave potential complications of the disease.
- •
Clinical criteria for vascular EDS: Two of four major diagnostic criteria establish the diagnosis. One or more minor criteria support but are not sufficient to establish the diagnosis.
- •
Major criteria:
- 1.
Easy bruising
- 2.
Arterial, intestinal, or uterine fragility
- 3.
Thin, translucent skin
- 4.
Characteristic facial features (thin, delicate, and pinched nose; hollow cheeks; prominent staring eyes in 30% of patients with vascular EDS)
- 1.
- •
Minor criteria:
- 1.
Small joint hypermobility
- 2.
Skin hyperextensibility
- 3.
Spontaneous pneumothorax/hemothorax
- 4.
Tendon or muscle rupture
- 5.
Early-onset varicose veins
- 6.
Carotid-cavernous fistula
- 7.
Talipes equinovarus (clubfoot)
- 1.
Physical Examination
- •
Classic (previously types I and II): skin hyperextensibility ( Fig. 3.122 ) ; positive Gorlin’s sign (ability to touch tip of tongue to nose) ( Fig. 3.123 ) ; easy scarring with abnormal scars ( Fig. 3.124 ) and bruising (“cigarette-paper scars”); smooth, velvety skin; subcutaneous spheroids (small, firm, cystlike nodules) along shins or forearms

FIG. 3.122
Velvety, soft, thin skin at the elbow with “rubber bandlike” hyperextensibility.
(Fitzsimons Army Medical Center Collection)

FIG. 3.123
The ability to touch the tip of the nose with the tongue (Gorlin’s sign) is frequently seen in Ehlers-Danlos syndrome, but only 10% of patients who do not have this syndrome can do this.
(Fitzsimons Army Medical Center Collection)

FIG. 3.124
Patient with benign hypermobile variant of Ehlers-Danlos syndrome demonstrating amazing joint flexibility.
(Fitzsimons Army Medical Center Collection)
- •
Hypermobility (type III): joint hypermobility and some skin hypermobility ( Fig. 3.125 ) with or without very smooth skin

FIG. 3.125
These enlarged and widely spread hypertrophic scars from repeated trauma are commonly seen with Ehlers-Danlos syndrome.
(Fitzsimons Army Medical Center Collection)
- •
Vascular (type IV): thin, translucent skin with visible veins; marked bruising; pinched nose; acrogeria; generalized tissue friability; spontaneous dissection and rupture of medium and large arteries; spontaneous rupture of organs, especially sigmoid colon, spleen, liver, and uterus
- •
Kyphoscoliotic (type VI): joint hypermobility, progressive scoliosis, ocular fragility and possible globe rupture, mitral valve prolapse, aortic dilation
- •
Arthrochalasia (types VIIA and VIIB): prominent joint hypermobility with subluxations, congenital hip dislocation, skin hyperextensibility, tissue fragility
- •
Dermatosparaxis (type VIIC): severe skin fragility with decreased elasticity, bruising, hernias
- •
Unclassified types: types V and IX—classic characteristics; type VIII—classic characteristics and periodontal disease; type X—mild classic characteristics, mitral valve prolapse; type XI—joint instability.
Diagnostic Tests
- •
Biochemical and gene testing for known molecular defects is recommended to confirm the diagnosis of vascular EDS.
- •
Plain radiographs may reveal calcified nodules along the shin or forearms, corresponding to the subcutaneous spheroids.
- •
Echocardiogram can identify mitral valve prolapse (MVP) and aortic dilation.
 Differential Diagnosis
Differential Diagnosis
- •
Marfan syndrome
- •
Osteogenesis imperfecta
- •
Autosomal dominant cutis laxa
- •
Familial joint hypermobility
- •
Pseudoxanthoma elasticum
 Treatment
Treatment
- •
Management of most skin and joint problems should be conservative and preventive. Joint hypermobility and pain in EDS usually does not require surgical intervention. Physical therapy to strengthen muscles is helpful. Surgical repair and tightening of joint ligaments can be performed, but ligaments often will not hold sutures. Surgical intervention should be considered on an individual basis.
- •
For patients with vascular EDS:
- •
Special surgical care is required because of increased tissue friability.
- •
Patients should be advised to avoid contact sports.
- •
Elevated blood pressure should be aggressively treated with beta blockers given the risk of arterial dissection.
- •
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Women with vascular EDS should be counseled about the risk of uterine, intestinal, and arterial rupture. Pregnancy is associated with an 11% mortality rate, and there is a 50% chance that the child will be affected.
58
Ephelides (Freckles)
 General Comments
General Comments
Definition
- •
Ephelides are extremely common lesions that present as clusters of small (approximately 2 mm in diameter), uniformly pigmented macules.
Etiology
- •
They are directly related to exposure to sunlight and are much more conspicuous in summer than in winter.
- •
They are more common and more numerous in individuals with red hair and blue eyes, in whom there is probably an autosomal mode of inheritance.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Sites of predilection include the nose, cheeks, shoulders, and dorsal aspects of the hands and arms.
- •
Ephelides present in childhood, increasing in frequency in adults, and typically regressing in the elderly. There is a predilection for females.
Physical Examination
- •
Clusters of small (approximately 2 mm in diameter), uniformly pigmented macules ( Fig. 3.126 )

FIG. 3.126
Severe freckling across the cheeks and nose in a young boy.
(Joanna Burch Collection)
Diagnostic Tests
- •
None necessary
 Differential Diagnosis
Differential Diagnosis
- •
Melanocytic nevus
- •
Lentigo
- •
Tinea versicolor
- •
Seborrheic keratosis
- •
Café-au-lait spots
 Treatment
Treatment
First Line
- •
Although a cosmetic nuisance, they are of no clinical importance, and no treatment is necessary.
Second Line
- •
Hydroquinone solutions
- •
Tretinoin
- •
Glycolic acid peels
- •
Azelaic acid
Third Line
- •
Cryosurgery
 Clinical Pearl(s)
Clinical Pearl(s)
- •
High levels of freckling may indicate a raised susceptibility to the later development of melanoma. Similarly, increasing numbers of freckles correlate with a higher frequency of acquired melanocytic nevi.
59
Epidermal Nevus
 General Comments
General Comments
Definition
- •
Epidermal nevi (EN) are benign congenital lesions characterized by hyperplasia of epidermal structures. They are also known by several descriptive names, including nevus verrucosus, nevus unius lateris, and ichthyosis hystrix. The epidermal nevi can be classified according to their predominant component: nevus sebaceus (sebaceous glands); nevus comedonicus (hair follicles); nevus syringocystadenoma papilliferum (apocrine glands); and nevus verrucosus (keratinocytes).
Etiology
- •
Activating fibroblast growth factor receptor 3 (FGFR3) mutations have been demonstrated in some, as have mutations in the p110 α-subunit of PI3K ( PIK3CA ), HRAS, KRAS, and NRAS.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
EN is usually distributed in a mosaic pattern of alternating stripes of involved and uninvolved skin. This pattern is termed Blaschko lines and occurs as a result of migration of skin cells during embryogenesis. Disorders that occur along the Blaschko lines usually reveal a linear pattern on the extremities and a wavy or arcuate pattern on the trunk ( Fig. 3.127 ).

FIG. 3.127
Large, brown, linear epidermal nevus following the lines of Blaschko.
- •
Larger lesions, more widespread lesions, and lesions of the head and neck are more likely to have associated internal complications.
Physical Examination
- •
EN are round, oval, or oblong; elevated; flat-topped; yellow-tan to dark brown; and have a uniformly warty or velvety surface with sharp borders.
- •
They appear more commonly on the head and neck.
Diagnostic Tests
- •
None necessary
- •
Excisional or incisional biopsy for confirmation of diagnosis if needed
 Differential Diagnosis
Differential Diagnosis
- •
Melanoma
- •
Nevus comedonicus
- •
Dysplastic nevus
- •
Basal cell carcinoma
- •
Squamous cell carcinoma
- •
Basal cell nevus syndrome
- •
Verruca vulgaris
 Treatment
Treatment
First Line
- •
Full-thickness surgical excision
Second Line
- •
Dermabrasion, cryotherapy, laser therapy
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The combination of an epidermal nevus and an associated internal abnormality (usually ophthalmologic, neural, or bony defect) is called “epidermal nevus syndrome.”
60
Epidermoid Cyst (Sebaceous Cyst, Epidermal Inclusion Cyst)
 General Comments
General Comments
Definition
- •
An epidermoid cyst is a smooth, dome-shaped swelling occurring predominantly on the face, neck, and upper trunk, resulting from damage to the pilosebaceous units. A punctum is usually present.
- •
Histologically, the cysts are lined by an epidermis-like epithelium, including a granular cell layer. The cysts contain laminated keratin.
Etiology
- •
Damage to the pilosebaceous units can cause epidermoid cysts.
- •
Epidermoid inclusion cysts may also complicate penetrating trauma to the skin, such as by a sewing needle, with resultant implantation of squamous epithelium into the dermis.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
This condition is usually asymptomatic.
- •
Acute inflammation, usually due to bacteria, may result in the subsequent disruption of the cyst wall, with the development of an intense, foreign body, giant cell reaction.
- •
Young and middle-aged adults are most often affected.
Physical Examination
- •
White or pale yellow, smooth, dome-shaped swellings occur predominantly on the face, neck, and upper trunk. A punctum is usually present ( Fig. 3.128 ).

FIG. 3.128
Small, firm, subcutaneous, dome-shaped white cyst that has a comedonal opening to the surface. Keratinaceous, odorous (like “rancid cheese”) material can be expressed from the cyst by application of firm lateral pressure.
(William Weston Collection)
- •
Cheeselike, foul-smelling material will exude from it with lateral pressure.
Diagnostic Tests
- •
None necessary
 Differential Diagnosis
Differential Diagnosis
- •
Insect bite
- •
Cylindroma
- •
Trichilemmoma
- •
Pylar cyst
- •
Granuloma annulare
- •
Dermoid cyst
- •
Lipoma
- •
Milia
 Treatment
Treatment
First Line
- •
Excision with narrow margins
Second Line
- •
Intralesional corticosteroid (for inflamed lesion)
Third Line
- •
Simple drainage (may lead to recurrence)
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The presence of multiple lesions may suggest the possibility of Gardner’s syndrome, which includes polyposis coli, jaw osteomas, and intestinal fibromatoses in addition to cutaneous cysts.
61
Epidermolysis Bullosa
 General Comments
General Comments
Definition
- •
Epidermolysis bullosa is a rare genetic disorder (50 cases per million live births) presenting with the development of cutaneous blisters following mild trauma. There are three major types based on the level of blister formation: dystrophic (dermolytic); junctional; and simplex (epidermolytic). Ninety-two percent of cases are epidermolysis bullosa simplex.
Etiology
- •
This is an inherited disorder. It is autosomal dominant for epidermolysis bullosa simplex, autosomal recessive for junctional type, and can be either autosomal dominant or recessive for dystrophic type.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
The condition is marked by development of painful blisters on the hands, feet, elbows, and knees following mild trauma ( Fig. 3.129 ).

FIG. 3.129
Epidermolysis bullosa dystrophica, recessive type, demonstrating hemorrhagic blisters on the ankle and foot.
(William Weston Collection)
- •
It may be complicated by atrophic scarring, milia formation, and nail dystrophy ( Fig. 3.130 ).

FIG. 3.130
Epidermolysis bullosa dystrophica, autosomal dominant type, demonstrating scarring and milia over the knuckles.
(William Weston Collection)
- •
Severely affected individuals may have esophageal and other gastrointestinal blistering.
Physical Examination
- •
Blisters on the hands, feet, elbows, and knees are seen.
Diagnostic Tests
- •
Skin biopsy and serum for direct and indirect immunofluorescence can detect skin basement membrane-specific autoantibodies and the level of the split.
- •
Genetic testing on serum can identify the specific subtype and gene defect.
 Differential Diagnosis
Differential Diagnosis
- •
Bullous pemphigoid
- •
Pemphigus vulgaris
- •
Linear IgA bullous dermatosis
- •
Porphyria cutanea tarda
- •
Chemical burn
- •
Thermal burn
- •
Blisters due to trauma (friction blisters)
- •
Cicatricial pemphigoid
 Treatment
Treatment
First Line
- •
Nutritional support, avoidance of trauma
- •
Topical antibiotics, sterile dressings, aggressive wound care, and analgesia
Second Line
- •
Bone marrow transplant
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Frequent skin surveillance is warranted to evaluate for squamous cell carcinoma, as metastatic squamous cell carcinoma is the most common cause of death in some subtypes of EB.
62
Erysipelas
 General Comments
General Comments
Definition
- •
Erysipelas is a clinical variant of bacterial cellulitis characterized by marked edema and a sharply demarcated edge.
Etiology
- •
Usually group A beta-hemolytic streptococci
- •
Less often group B, C, or G streptococci
- •
Rarely S. aureus or Hemophilus influenzae
- •
Risk factors: impaired lymphatic or venous drainage (mastectomy, saphenous vein harvesting), immunocompromised state; athlete’s foot is a common portal of entry.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
The most characteristic site is the face.
- •
Systemic signs of infection (fever) are often present.
Physical Examination
- •
Distinctive red, warm, tender skin lesion with induration and a sharply defined, advancing, raised border is present ( Fig. 3.131 ).
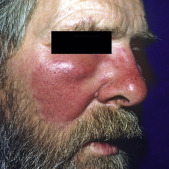
FIG. 3.131
Superficial, rapidly spreading, tender plaque of erysipelas involving the right cheek and nose with a raised, advancing border.
(William Weston Collection)
- •
Vesicles, bullae, and pustules ( Fig. 3.132 ) may develop.

FIG. 3.132
Erysipelas. Rapidly spreading, tender plaque of the nose studded with small, follicular pustules.
(Fitzsimons Army Medical Center Collection)
- •
After several days, lesions may appear ecchymotic.
- •
After 7 to 10 days, desquamation of the affected area may occur.
Diagnostic Tests
- •
Diagnosis is usually made by characteristic clinical setting and appearance.
- •
CBC and white blood cell count (WBC) often elevated.
- •
Blood cultures are positive in 5% of patients.
- •
Gram’s stain and culture of any drainage from skin lesions should be performed.
- •
Culture of aspirated fluid from the leading edge of skin lesion has a low yield.
 Differential Diagnosis
Differential Diagnosis
- •
Other types of cellulitis
- •
Necrotizing fasciitis
- •
DVT
- •
Contact dermatitis
- •
Erythema migrans (Lyme disease)
- •
Insect bite
- •
Herpes zoster
- •
Erysipeloid
- •
Acute gout
- •
Pseudogout
 Treatment
Treatment
- •
For typical erysipelas of the extremity in a nondiabetic patient, treat as follows:
- •
PO: penicillin V 250 mg to 500 mg QID
- •
IV: penicillin G (aqueous) 1 to 2 million units Q6H
- •
Note : Use erythromycin or cephalosporin in patients allergic to penicillin.
- •
For facial erysipelas (include coverage for S. aureus ), treat as follows:
- •
Mild cases can be treated with oral cephalexin, dicloxacillin, erythromycin, clarithromycin, or azithromycin.
- •
Severe cases are treated with nafcillin or oxacillin 2 g IV Q4H
- •
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Consider early surgical referral when necrotizing fasciitis is suspected.
- •
Consider skin biopsy when the patient does not respond to appropriate antibiotics.
63
Erythema Infectiosum (Fifth Disease)
 General Comments
General Comments
Definition
- •
Erythema infectiosum, also known as “fifth disease,” is a viral exanthem caused by parvovirus B 19 , affecting primarily school-age children. Erythema infectiosum was the “fifth” in a series of described viral exanthems of childhood.
Etiology
- •
Erythema infectiosum is the most common clinical syndrome associated with parvovirus B 19 .
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
This is a self-limited disease lasting 1 to 2 weeks.
- •
Polyarthritis and arthralgias are commonly seen in older patients but are less common in children. Arthritis involves small joints of extremities in symmetric fashion.
- •
Mild fever is seen in up to one third of patients.
Physical Examination
- •
In children, a typical bright red, nontender, maxillary rash with circumoral pallor over cheeks produces the classic “slapped cheek” appearance ( Fig. 3.133 ).

FIG. 3.133
Erythema infectiosum. Typical slapped cheeks in a child.
(William Weston Collection)
- •
In adults, a reticular, nonpruritic, lacy, erythematous, maculopapular rash over trunk ( Fig. 3.134 ) and extremities may last for up to several weeks after the acute episode. It may be worsened by heat or sunlight.

FIG. 3.134
Lacelike erythema on the arms of a child with erythema infectiosum.
(William Weston Collection)
- •
Polyarthritis and arthralgias are commonly seen in older patients but are less common in children. Arthritis involves small joints of extremities in symmetric fashion.
- •
Mild fever is present in up to one third of patients.
Diagnostic Tests
- •
None necessary
 Differential Diagnosis
Differential Diagnosis
- •
Juvenile rheumatoid arthritis (Still’s disease)
- •
Rubella, measles (rubeola), and other childhood viral exanthems
- •
Mononucleosis
- •
Lyme disease
- •
Acute HIV infection
- •
Drug eruption
 Treatment
Treatment
First Line
- •
Treatment is supportive only.
- •
NSAIDs may be given for arthralgias/arthritis.
Second Line
- •
Intravenous immunoglobulin and transfusion support may be used in patients with an immunocompromised state with red cell aplasia.
- •
Consider immunoglobulin treatment or prophylaxis in pregnancy.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Symmetric arthritis involving the small joints is common in adults, whereas facial rash is common in children.
- •
The virus may cause transient aplastic crisis in patients with underlying hematologic disorders such as sickle cell disease, in immunocompromised patients, and after transplantation.
- •
Infection may be a cause of hydrops fetalis in early pregnancy.
64
Erythema Multiforme
 General Comments
General Comments
Definition
- •
Erythema multiforme (EM) is an inflammatory disease due to a type IV hypersensitivity reaction to infection or drugs. It is often associated with herpes simplex and other infectious agents, drugs, and connective tissue diseases.
Etiology
- •
The majority of EM cases follow outbreaks of herpes simplex virus 1 and 2.
- •
Patients with herpes-associated EM demonstrate viral antigens in the basal keratinocytes that induce a T-cell mediated host response.
- •
Mycoplasma pneumoniae, fungal infections, and medications (bupropion, sulfonamides, penicillins, NSAIDs, barbiturates, phenothiazines, hydantoins) are also possible causes.
- •
In more than 50% of patients, no specific cause is identified.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Prodromal symptoms are mild or absent. Itching or burning at the site of eruption may occur.
- •
Lesions are most common in the back of the hands and feet and extensor aspect of the forearms and legs. Trunk involvement can occur in severe cases.
- •
Individual lesions heal in 1 or 2 weeks without scarring.
Physical Examination
- •
Symmetric skin lesions with a classic “target” appearance (caused by the centrifugal spread of red maculopapules to circumference of 1 to 3 cm with a purpuric, cyanotic, or vesicular center) are present ( Fig. 3.135 ). The papules may enlarge into plaques measuring a few centimeters in diameter with a dark or red central portion. Target lesions may not be apparent for several days.

FIG. 3.135
Erythema multiforme secondary to herpes simplex infection. Classic targetoid lesions with central bullae in some lesions.
(William Weston Collection)
- •
Urticarial papules, vesicles, and bullae may also be present and generally indicate a more severe form of the disease.
- •
Bullae and erosions may also be present in the oral cavity ( Fig. 3.136 ).

FIG. 3.136
Recurrent mucosal erythema multiforme secondary to herpes simplex infection.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
Medical history with emphasis on drug ingestion
- •
Laboratory evaluation in patients with suspected collagen-vascular diseases
- •
Skin biopsy when diagnosis is unclear
- •
CBC with differential
- •
ANA
- •
Serology for M. pneumoniae, HSV-1, HSV-2
- •
Urinalysis
 Differential Diagnosis
Differential Diagnosis
- •
Chronic urticaria
- •
Secondary syphilis
- •
Pityriasis rosea
- •
Contact dermatitis
- •
Pemphigus vulgaris
- •
Lichen planus
- •
Serum sickness
- •
Drug eruption
- •
Granuloma annulare
- •
Polymorphic light eruption
- •
Viral exanthema
- •
Leukocytoclastic vasculitis
- •
SLE
- •
Secondary syphilis
 Treatment
Treatment
First Line
- •
Mild cases generally do not require treatment; lesions resolve spontaneously within 1 month.
- •
Potential drug precipitants should be removed.
- •
Treatment of the precipitating disease, if known (e.g., valacyclovir or famciclovir for herpes simplex, erythromycin for Mycoplasma infection) is indicated.
Second Line
- •
Dapsone, antimalarials, azathioprine, or cyclosporine use is reserved for cases resistant to antivirals.
Third Line
- •
Prednisone may be tried in patients with many target lesions; however, the role of systemic steroids remains controversial.
- •
Levamisole, an immunomodulator, may be effective in treatment of patients with chronic or recurrent oral lesions (dose is 150 mg/day for 3 consecutive days used alone or in combination with prednisone).
- •
IV immunoglobulins in severe cases.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The rash of EM generally evolves over a 2-week period and resolves within 3 to 4 weeks without scarring.
- •
The risk of recurrence of erythema multiforme exceeds 30%.
65
Erythema Nodosum
 General Comments
General Comments
Definition
- •
Erythema nodosum is characterized by panniculitis, manifesting with tender erythematous nodules on the lower extremities.
Etiology
- •
This cell-mediated hypersensitivity reaction is seen more frequently in persons with human leukocyte antigen (HLA) B8. The lesion results from an exaggerated interaction between an antigen and cell-mediated immune mechanisms leading to granuloma formation. Up to 55% of cases of erythema nodosum are idiopathic. Other causes include: sarcoidosis (39% of sarcoidosis cases); infections (bacteria, fungi, viruses); drugs (sulfonamides, penicillin, oral contraceptives); cancer, usually lymphoma; ankylosing spondylosis; and reactive arthropathies (e.g., associated with inflammatory bowel disease).
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Erythema nodosum manifests with an acute onset of tender nodules that are typically located on shins ( Fig. 3.137 ) and occasionally seen on thighs and forearms.

FIG. 3.137
Tender, pink-to-red nodules on the anterior tibia of young woman. The cause was never established.
(Fitzsimons Army Medical Center Collection)
- •
Associated findings include the following:
- •
Fever
- •
Lymphadenopathy
- •
Arthralgia
- •
Signs of the underlying illness
- •
Physical Examination
- •
The nodules are usually 1 ⁄ 8 inch to 1 inch in diameter but can be as large as 4 inches. They begin as light red lesions, then become darker and often ecchymotic. The nodules heal within 8 weeks without ulceration.
Diagnostic Tests
- •
ESR
- •
Throat culture and antistreptolysin O titer
- •
Purified protein derivative (PPD)
- •
Chest x-ray
- •
Others depending on index of suspicion (e.g., stool culture and evaluation for ova and parasites in patients with diarrhea and GI symptoms)
- •
Skin biopsy in doubtful cases:
- •
Early lesion: inflammation and hemorrhage in subcutaneous tissue
- •
Late lesion: giant cells and granulomata
- •
 Differential Diagnosis
Differential Diagnosis
- •
Insect bites
- •
Posttraumatic ecchymoses
- •
Vasculitis
- •
Weber-Christian disease
- •
Fat necrosis associated with pancreatitis
- •
Necrobiosis lipoidica
- •
Scleroderma
- •
Lupus panniculitis
- •
Subcutaneous granuloma
- •
Alpha-1 antitrypsin deficiency
 Treatment
Treatment
First Line
- •
Treatment of underlying disorders
- •
Avoidance of contact irritation of affected areas
- •
NSAIDs for pain
Second Line
- •
Systemic steroids (prednisone 1 mg/kg of body weight/day, tapered over several days) may be useful in severe cases if the underlying risk of sepsis and malignancy has been excluded.
Third Line
- •
Potassium iodide given as tablet 300 mg tid or as a supersaturated solution (5 drops, 3 times/day in orange juice) has been reported as effective for symptom control.
- •
Intralesional corticosteroid injections for persistent lesions
- •
Dapsone
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The disease is self-limited and treatment is symptomatic. Erythema nodosum nodules develop in pretibial locations and resolve spontaneously over several weeks without scarring or ulceration.
66
Erythroderma
 General Comments
General Comments
Definition
- •
Erythroderma is a persistent severe generalized inflammation of the skin. When it is associated with increased scale, it is called exfoliative dermatitis or exfoliative erythroderma.
Etiology
- •
Eczema
- •
Psoriasis
- •
Drug eruptions
- •
Sezary syndrome, cutaneous lymphomas
- •
Pemphigus foliaceus
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
The skin becomes reddened, thickened, inflamed, and exfoliated continuously.
- •
Onset can be slowly progressive or rapid.
- •
Systemic symptoms such as generalized malaise, shivering, fever, impaired sweating, fatigue, and tachycardia may be present.
- •
Rapid onset with high rate of skin loss can lead to protein malnutrition, dehydration, and high-output cardiac failure.
Physical Examination
- •
Skin appears red, thickened, and inflamed ( Fig. 3.138 ).

FIG. 3.138
Erythroderma of unknown cause in an elderly woman.
(John Aeling Collection)
- •
Persistent exfoliation of skin may be present.
Diagnostic Tests
- •
Skin biopsy is helpful for suspected T-cell lymphoma.
 Differential Diagnosis
Differential Diagnosis
- •
Atopic eczema
- •
Seborrheic dermatitis
- •
Drug eruption (sulfonamides, allopurinol, anticonvulsants, penicillins)
- •
Cutaneous T-cell lymphoma (Sézary syndrome)
- •
Pityriasis rubra pilaris
- •
Norwegian (crusted) scabies
- •
Fungal infection
- •
Lichen planus
 Treatment
Treatment
First Line
- •
Treatment of underlying etiology (e.g., immediate removal of any suspected drugs)
- •
Application of bland emollients (e.g., petroleum) to soothe skin and partially restore skin barrier
- •
Nutritional support; intravenous hydration
Second Line
- •
Topical corticosteroids
- •
Phototherapy
Third Line
- •
Cyclosporine, cytotoxic drugs, antimetabolites
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Fulminant erythroderma is a life-threatening condition.
- •
Systemic steroids are best avoided in erythrodermic psoriasis due to risk of pustular psoriasis on withdrawal.
67
Erythrasma
 General Comments
General Comments
Definition
- •
Erythrasma is a bacterial skin infection.
Etiology
- •
The condition is caused by Corynebacterium minutissimum, a gram-positive bacillus.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
It characteristically manifests as symptomatic, well-defined, scaly brownish-red patches under the breasts, inguinal skin ( Fig. 3.139 ) , and intergluteal skin.

FIG. 3.139
Erythrasma. Asymptomatic, slightly scaly, tan-red patches of the groin in a young man.
(Fitzsimons Army Medical Center Collection)
Physical Examination
- •
Well-defined reddish-brown flexural plaques are seen on examination.
Diagnostic Tests
- •
Coral-red fluorescence can be demonstrated under Wood’s light ( Fig. 3.140 ). It is due to production of coproporphyrin II by the organism.

FIG. 3.140
Wood’s light examination of erythrasma demonstrates diagnostic coral red fluorescence due to porphyrins produced by the bacteria.
(Fitzsimons Army Medical Center Collection)
- •
A skin biopsy can also reveal the organism in the stratum corneum.
 Differential Diagnosis
Differential Diagnosis
- •
Intertrigo
- •
Tinea
- •
Contact dermatitis
- •
Eczema
- •
Pityriasis rosea
 Treatment
Treatment
First Line
- •
Topical creams (miconazole, clotrimazole, econazole)
- •
Topical clindamycin lotion or solution
Second Line
- •
Oral erythromycin
Third Line
- •
Oral clarithromycin or tetracycline
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Erythrasma has a predilection for obese and diabetic patients and is more common in areas with a humid and hot climate.
68
Erythroplasia of Queyrat
 General Comments
General Comments
Definition
- •
Erythroplasia of Queyrat is the term that has been historically used for squamous cell carcinoma in situ occurring on the glans penis, the prepuce, or urethral meatus.
Etiology
- •
HPV types 16, 18, 31, 35
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Occurs most commonly in middle-aged and elderly uncircumcised men
Physical Examination
- •
Single or multiple, fixed, well-circumscribed, erythematous, moist, velvety or smooth, red-surfaced plaques on the glans penis ( Fig. 3.141 )

FIG. 3.141
Erythroplasia of Queyrat (squamous cell carcinoma in situ) presenting as fixed, well-circumscribed, erythematous, moist, red plaques on the glans penis and corona.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
Biopsy
 Differential Diagnosis
Differential Diagnosis
- •
Zoon’s balanitis
- •
Penile psoriasis
- •
Extramammary Paget’s disease
- •
Irritant balanitis
- •
Candidiasis
 Treatment
Treatment
First Line
- •
Topical 5-FU cream applied daily
- •
Imiquimod cream applied daily
Second Line
- •
Neodymium: YAG or carbon dioxide laser therapy
- •
Excision
Third Line
- •
Radiation therapy
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Sexual partners of men with SCC of the penis are more likely to develop preinvasive and invasive cancer of the cervix or anus.
69
Folliculitis
 General Comments
General Comments
Definition
- •
Folliculitis is inflammation of the hair follicle as a result of infection, physical injury, or chemical irritation.
Etiology
- •
Bacterial folliculitis: Staphylococcus infection ( Fig. 3.142 ) , Pseudomonas aeruginosa (“hot tub” folliculitis) ( Fig. 3.143 ) , gram-negative folliculitis ( Klebsiella, Enterobacter, Proteus ) associated with antibiotic treatment of acne

FIG. 3.142
Staphylococcal, follicular infection (impetigo of Bockhart) with distinct, folliculocentric pustules with surrounding erythema.
(John Aeling Collection)

FIG. 3.143
“Hot tub” folliculitis consisting of numerous erythematous, purulent follicles appearing 1 to 4 days after hot tub exposure.
(Fitzsimons Army Medical Center Collection)
- •
Fungal folliculitis: dermatophytes, Candida, Pityrosporum orbiculare ( Fig. 3.144 )

FIG. 3.144
Pityrosporum folliculitis of the shoulder and arm. Pityrosporum folliculitis most commonly affects the trunk followed by the face.
(Walter Reed Army Medical Center Collection)
- •
Mechanical folliculitis: chronic irritation of the hair follicle (use of cocoa butter or coconut oil, chronic chafing from clothing, irritation from workplace), shaving (syscosis barbae)
- •
Medication induced folliculitis: initial use of systemic corticosteroid therapy (steroid acne) ( Fig. 3.145 ) , isoniazid therapy, chemotherapy

FIG. 3.145
Steroid acne presenting as an acute folliculitis of the trunk precipitated by the administration of high dose, oral prednisone.
(Fitzsimons Army Medical Center Collection)
- •
Inflammatory folliculitis: eosinophilic folliculitis (HIV-related; childhood variant) , follicular atopic dermatitis
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Patients with sycosis barbae may initially present with small follicular papules or pustules that increase in size with continued shaving; deep follicular pustules may occur surrounded by erythema and swelling; the upper lip is frequently involved.
- •
“Hot tub” folliculitis occurs within 1 to 4 days following use of hot tub with poor chlorination, and it is characterized by pustules with surrounding erythema generally affecting torso, buttocks, and limbs.
Physical Examination
- •
The lesions generally consist of painful yellow pustules ( Fig. 3.119 ) surrounded by erythema; a central hair is present in the pustules.
Diagnostic Tests
- •
Gram stain is useful to identify the infective organisms in infectious folliculitis and to differentiate infectious folliculitis from noninfectious.
 Differential Diagnosis
Differential Diagnosis
- •
Pseudofolliculitis barbae (ingrown hairs)
- •
Acne vulgaris
- •
Dermatophyte fungal infections
- •
Keratosis biliaris
- •
Cutaneous candidiasis
- •
Superficial fungal infections
- •
Miliaris
 Treatment
Treatment
First Line
- •
Prevention of chemical or mechanical skin irritation
- •
Glycemic control in diabetics
- •
Proper chlorination of hot tubs and spas for hot tub folliculitis
- •
Shaving with a clean razor for sycosis barbae
- •
Cleansing of the area with chlorhexidine and application of saline compresses to the involved area
- •
Application of 2% mupirocin ointment for bacterial folliculitis affecting a limited area (e.g., sycosis barbae)
Second Line
- •
Treatment of Pseudomonas folliculitis with oral ciprofloxacin
- •
Treatment of S. aureus folliculitis with dicloxacillin 250 mg QID for 10 days
Third Line
- •
Chronic nasal or perineal S. aureus carriers with frequent folliculitis can be treated with rifampin 300 mg BID for 5 days.
- •
Mupirocin applied to nares BID is also effective for nasal carriers.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Staphylococcal folliculitis is the most common form of infectious folliculitis; it occurs most commonly in persons with diabetes.
70
Frostbite
 General Comments
General Comments
Definition
- •
Frostbite represents tissue injury (or death) from freezing and vasoconstriction induced by severe environmental cold exposure.
Etiology
- •
Two distinct mechanisms are responsible for tissue injury in frostbite:
- 1.
Cellular death occurring at time of exposure from ice crystal damage to cells
- 2.
Deterioration and necrosis attributable to progressive dermal ischemia after rewarming through inflammatory mediators
- 1.
- •
Environmental factors include wind chill factor, temperature, duration of exposure, altitude, and degree of wetness. Hands and feet account for 90% of injuries; earlobes, nose, and male genitalia are also more susceptible. Host factors include extremes of age, immobility, history of cold injuries, skin damage, psychiatric illness, neuroleptic and sedative drugs (especially alcohol), atherosclerosis, malnutrition, tobacco use, peripheral neuropathy, hypothyroidism, fatigue, and wearing constricting clothing/footwear.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Patients initially experience numbness, prickling, and itching. More severe injury can produce paresthesias and stiffness, with burning or throbbing pain upon thawing.
Physical Examination
- •
Frostbite may be classified into degrees of injury or, more practically, into superficial and deep groups.
- •
Superficial frostbite involves the skin and subcutaneous tissue. The frozen part is waxy, white, and firm but soft and resilient below the surface when gently depressed. After rewarming, the frostbitten area may appear mottled and swollen, and superficial blisters ( Fig. 3.146 ) with clear or milky fluid may form within 6 to 24 hours. There is no ultimate tissue loss.

FIG. 3.146
Bulla formation of the right fifth toe with edema and early necrotic changes characteristic of frostbite.
- •
Deep frostbite extends into subcutaneous tissues and may involve muscles, nerves, tendons, or bones. The skin may be hard or wooden, without tissue resilience. Edema, cyanosis, hemorrhagic blisters (after 3–7 days), tissue necrosis ( Fig. 3.147 ) , and gangrene may develop. Affected tissue has a poor prognosis, and debridement or amputation is generally required.

FIG. 3.147
Minimal frostbite or frostnip presenting as erythema and minimal edema of the distal second toe after cold exposure.
- •
Diagnostic Tests
- •
Wound and blood cultures may be needed in more severe cases.
- •
Technetium scintigraphy, MRI, and magnetic resonance angiography (MRA) are the most promising modalities for assessment of tissue viability, but delay of 5 days is required to distinguish a level of debridement or amputation. (Some centers perform angiography within 24 hours and give thrombolytics to those with impaired blood flow.)
 Differential Diagnosis
Differential Diagnosis
Other induced cold injuries include the following:
- •
Frostnip ( Fig. 3.148 ) : transient tingling and numbness without associated permanent tissue damage

FIG. 3.148
Distal erythema with punctate areas of early necrosis involving all toes of the left foot after a long walk in subzero temperatures.
- •
Pernio (chilblains): a self-limited, cold-induced lymphocytic vasculitis of dermal vessels associated with purple plaques or nodules, often affecting dorsum of hands and feet and seen with prolonged cold exposure to above-freezing temperatures
- •
Cold immersion (trench) foot: caused by ischemic injury resulting from sustained severe vasoconstriction in appendages exposed to wet cold at temperatures above freezing
 Treatment
Treatment
First Line
- •
Remove constricting or wet clothing and gently insulate, immobilize, and elevate the affected area.
- •
Avoid thawing if there is any risk of refreezing.
- •
Do not rub or massage the affected area.
- •
If there is associated hypothermia, core temperature must first be stabilized with warmed, humidified oxygen, heated intravenous saline (45°–65° C), and warming blankets before thawing of frostbitten extremities.
- •
Immerse affected area in circulating warm water bath with a mild antibacterial agent (e.g., hexachlorophene or povidone-iodine) maintained at 40° to 42° C for 15 to 30 minutes. Repeat until capillary refill returns and tissue is supple. Active motion during rewarming is advisable; massage is not.
- •
Administer intravenous narcotics for pain during thawing.
Second Line
- •
Tetanus prophylaxis and topical antibiotics should be given if there is a potentially contaminated skin wound.
- •
Streptococcal prophylaxis with intravenous penicillin for 48 to 72 hours may be advisable for severe cases.
Third Line
- •
Thrombolytic therapy
- •
Dextran, vasodilators, hyperbaric oxygen, reserpine, and sympathectomy are of unproven benefit.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Continuous ECG monitoring is indicated. J (Osborn) waves may be noted on ECG.
71
Furuncle
 General Comments
General Comments
Definition
- •
A furuncle (boil) is a deep infection of the hair follicle.
Etiology
- •
Most infections are caused by S. aureus.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Furuncles are more common in young adults and usually affect the skin of the face, neck, buttocks, and axillae.
- •
After discharge of the pustular necrotic core, the lesion heals rapidly but with scarring.
Physical Examination
- •
Furuncles are characterize by a firm, very tender, red hot nodule that may not initially demonstrate a central keratotic plug ( Fig. 3.149 ) but later often demonstrates a draining central necrotic plug ( Fig. 3.150 ).

FIG. 3.149
An acute furuncle presenting as a firm, very tender, hot nodule, warm to the touch.
(William Weston Collection)

FIG. 3.150
Draining exquisitely painful, firm abscess on the posterior thigh with considerable edema and redness. Note the centrally located pustular opening.
(William Weston Collection.)
- •
Lesions are tender and can be up to 2 cm across. The inflammation is not confined within the follicle but is associated with much surrounding erythema and, often, systemic symptoms.
Diagnostic Tests
- •
Culture and sensitivity of pus
- •
Nasal swab
- •
CBC
 Differential Diagnosis
Differential Diagnosis
- •
Folliculitis
- •
Pseudofolliculitis
- •
Foreign body reaction
- •
Acne
- •
Hidradenitis suppurativa
- •
Epidermoid cyst
 Treatment
Treatment
First Line
- •
Incision and drainage and oral antibiotics
Second Line
- •
Topical antibiotics (2% mupirocin ointment)
- •
Systemic antibiotics (dicloxacillin, cephalexin, azithromycin)
 Clinical Pearl(s)
Clinical Pearl(s)
- •
A “carbuncle” is a cluster of furuncles, usually infected with staphylococcus or group A streptococcus. It can be life-threatening if untreated, particularly in diabetic patients or other immunocompromised states.
72
Glomus Tumor
 General Comments
General Comments
Definition
- •
A glomus tumor is a benign lesion arising from glomus bodies, which are specialized arteriovenous anastomoses found most often in the fingers and palm and thought to serve as thermoregulatory receptors.
Etiology
- •
Unknown. The lesions arise from the neuromyoarterial apparatus.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Glomus tumors classically present with paroxysmal severe pain, which is precipitated by cold, pressure, or dependency.
Physical Examination
- •
Typically the tumors are small (<1 cm in diameter), reddish-blue nodules.
- •
The nodules may be flesh-colored but may become purple with hemorrhage ( Fig. 3.151 ).
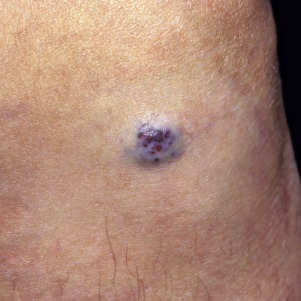
FIG. 3.151
Glomus tumor: close-up view of violaceous, vascular tumor.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
Excisional biopsy
 Differential Diagnosis
Differential Diagnosis
- •
Schwannoma (neurilemmona)
- •
Eccrine spiradenoma
- •
Hemangioma
- •
Arteriovenous malformation (AVM)
- •
Blue nevus
- •
Melanoma
- •
Angiolipoma
 Treatment
Treatment
- •
Surgical excision is required. Subungal lesions will usually require removal of the nail.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Sometimes the nodules erode the bone of the phalanx and cause pressure dystrophy of the overlying nail.
73
Gonorrhea and Gonococcemia
 General Comments
General Comments
Definition
- •
Gonorrhea is a sexually transmitted bacterial infection. It commonly manifests as urethritis, cervicitis, or salpingitis. Infection may be asymptomatic. Gonococcemia is a disseminated infection due to bacteremia.
Etiology
- •
Gonorrhea is caused by Neisseria gonorrhoeae. The infection differs in males and females in course, severity, and ease of recognition.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Males: Purulent discharge from anterior urethra with dysuria will appear 2 to 7 days after infecting exposure. Homosexual men may also have rectal infection causing pruritus, tenesmus, and discharge, or may be asymptomatic.
- •
Females: Mild urethritis or cervicitis may occur a few days after exposure. In about 20% of cases, uterine invasion occurs after menstrual period with signs and symptoms of endometritis, salpingitis, or pelvic peritonitis. The patient may have purulent discharge and inflamed Skene’s or Bartholin’s glands.
- •
Classic presentation of acute gonococcal pelvic inflammatory disease (PID) is fever and abdominal and adnexal tenderness, often absent of purulent discharge. Physical examination may be normal if the patient is asymptomatic.
Physical Examination
- •
Purulent discharge from the anterior urethra is seen in males ( Fig. 3.152 ). Females may have purulent discharge and inflamed Skene’s or Bartholin’s glands.

FIG. 3.152
Acute gonorrhea with urethral discharge. The patient also has a chancre of primary syphilis.
(Fitzsimons Army Medical Center Collection)
- •
The infection may not be limited to the genitalia. Tender, hemorrhagic pustules on a red-to-purple base may present on the palms and soles ( Fig. 3.153 ) in gonococcemia.

FIG. 3.153
Tender, hemorrhagic pustule and necrotic papule on a violaceous base present on the palm and hand of this woman with gonococcemia.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
NAAT of voided urine or self-collected vaginal or urethral swabs have largely replaced culture for diagnosis.
- •
Gonorrhea culture on Thayer-Martin medium (organism is fastidious, requires aerobic conditions with increased carbon dioxide atmosphere; incubate as soon as possible)
- •
Serologic testing for syphilis on all patients
- •
Chlamydia testing on all patients
- •
Offer of HIV counseling and testing
 Differential Diagnosis
Differential Diagnosis
- •
Nongonococcal urethritis (NGU)
- •
Nongonococcal mucopurulent cervicitis
- •
Chlamydia trachomatis
 Treatment
Treatment
- •
For uncomplicated infections of the cervix, urethra, and rectum:
- •
Ceftriaxone 125 mg IM × 1 dose plus Azithromycin 1 g PO dose. Doxycycline 100 mg PO bid can be substituted for azithromycin in patients allergic to azithromycin.
- •
- •
Alternatives:
- •
In patients allergic to cephalosporins: Azithromycin 2 g PO plus single dose gemifloxacin 320 mg PO or gentamicin 240 mg IM
- •
 Clinical Pearl(s)
Clinical Pearl(s)
- •
A rising number of cases of quinolone-resistant N. gonorrhoeae have been reported. Fluoroquinolones are no longer recommended to treat gonorrhea.
- •
Sexual partners should be identified, examined, cultured, and receive presumptive treatment.
74
Granuloma Annulare
 General Comments
General Comments
Definition
- •
Granuloma annulare (GA) is a chronic, usually self-limited, inflammatory disorder of the dermis and/or subcutis that classically presents as arciform to annular plaques located on the extremities.
Etiology
- •
The cause is unknown, but it may be related to vasculitis, trauma, monocyte activation, or delayed hypersensitivity.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
The four main clinical variants of granuloma annulare are: localized (75%); disseminated (>10 lesions); subcutaneous (occurring primarily in children 2–5 years of age); and perforating (rare form manifesting with 1- to 4-mm papules with a central crust).
- •
Most lesions resolve spontaneously after several months.
Physical Examination
- •
Localized granuloma annulare starts as a small ring of colored skin or pale erythematous dermal papules.
- •
Lesions coalesce and evolve into annular plaques over several weeks.
- •
Plaques undergo central involution and increase in diameter over several months (0.5–5 cm).
- •
It is most commonly found on the lateral and dorsal surfaces of the hands ( Fig. 3.154 ) and feet.

FIG. 3.154
Granuloma annulare. Annular, confluent, brownish-red plaques and papules, resembling ringworm, on the ankle.
(William Weston Collection)
- •
The generalized form of GA is characterized by hundreds to thousands of small, red to reddish-brown to reddish-violaceous papules in a symmetric distribution on the trunk and extremities ( Fig. 3.155 ).

FIG. 3.155
Generalized granuloma annulare presenting as numerous violaceous papules.
(William Weston Collection)
- •
Deep dermal (subcutaneous GA) presents as large, painless, skin-colored nodules that are often mistaken for rheumatoid nodules or bony prominences.
Diagnostic Tests
- •
No laboratory tests will help confirm the diagnosis.
- •
Biopsy shows focal degeneration of collagen and elastic fibers, mucin deposition, and perivascular and interstitial lymphohistiocytic infiltrate in the upper and middermis.
 Differential Diagnosis
Differential Diagnosis
- •
Tinea corporis
- •
Lichen planus
- •
Necrobiosis lipoidica diabeticorum
- •
Sarcoidosis
- •
Rheumatoid nodules
- •
Late secondary or tertiary syphilis
- •
Arcuate and annular plaques of mycosis fungoides
- •
Annular elastolytic giant cell granuloma
- •
Papular GA can simulate insect bites, secondary syphilis, and xanthoma.
 Treatment
Treatment
First Line
- •
No treatment is necessary; spontaneous resolution is expected.
- •
High-potency topical corticosteroids with or without occlusion
- •
Intralesional steroid injection into elevated border
- •
Cryosurgery
Second Line
- •
Phototherapy
- •
Ablative laser
Third Line
- •
Systemic agents (e.g., niacinamide, hydroxychloroquine, chloroquine, cyclosporine, dapsone) are generally reserved for severe cases.
- •
Recent case reports indicate positive outcomes with topical tacrolimus and pimecrolimus, and with systemic infliximab.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
GA has been described as a paraneoplastic granulomatous reaction to Hodgkin’s disease, non-Hodgkin’s lymphoma (NHL), solid organ tumors, and mycosis fungoides.
- •
The disseminated form of GA is sometimes associated with diabetes mellitus.
75
Granuloma Inguinale
 General Comments
General Comments
Definition
- •
Granuloma inguinale is an infection manifesting with granulomatous ulcerations.
Etiology
- •
It is caused by a gram-negative bacterium, Klebsiella granulomatis, formerly called Calymmatobacterium granulomatis, which may be sexually transmitted. It can also be spread through close, chronic nonsexual contact.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Lesions bleed easily. They are sharply defined and painless.
- •
Secondary infection may ensue.
- •
Inguinal involvement may cause pseudobuboes.
- •
Elephantiasis can result from obstruction of lymphatics.
Physical Examination
- •
An indurated nodule is the primary lesion and is usually painless.
- •
The lesion erodes to granulomatous heaped ulcer and progresses slowly ( Fig 3.156 ).

FIG. 3.156
Granuloma inguinale presenting as a large penile ulcer with granulation tissue at the base.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
Microscopic examination of either biopsy specimen or tissue smears
- •
Wright stain: observation of Donovan bodies (intracellular bacteria); organisms in vacuoles within macrophages
- •
HIV testing in all patients
 Differential Diagnosis
Differential Diagnosis
- •
Carcinoma
- •
Secondary syphilis: condylomata lata
- •
Amebiasis: necrotic ulceration
- •
Concurrent infections
- •
Lymphogranuloma venereum
- •
Chancroid
- •
Genital herpes
 Treatment
Treatment
- •
Recommended regimen:
- •
Azithromycin 500 mg PO daily or 1 g PO/week × at least 3 weeks and until lesions have completely healed
- •
- •
Alternative regimens:
- •
Doxycycline 100 mg PO BID for 3 weeks minimum
- •
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Sexual partners should be examined and offered therapy.
76
Grover’s Disease (Transient Acantholytic Dermatosis)
 General Comments
General Comments
Definition
- •
Grover’s disease (GD), also known as transient acantholytic dermatosis (TAD), is a skin disorder characterized by the presence of pruritic papules and vesicles that turn into crusted and keratotic lesions.
Etiology
- •
Unknown. There is a significant association with atopy and dry skin. Impairment of keratinocytic cholinergic receptors has been suggested as a pathogenic mechanism. TAD has been reported with cetuximab.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
The distribution is predominantly limited to the chest or shoulder girdle area and upper abdomen. There is a strong male predominance, and it is seen most commonly in the elderly.
- •
The condition often appears or flares during periods of heat, sweating, or hospitalization.
- •
Pruritus may be present, but patients are often asymptomatic.
Physical Examination
- •
Fragile vesicles that rapidly turn into crusted red to reddish brown keratotic erosions and papules ( Fig. 3.157 )

FIG. 3.157
Transient acantholytic dermatosis (Grover’s disease) presenting as small, tan-brown, hyperkeratotic papules on the trunk of an older man.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
Biopsy reveals focal acantholysis and abnormalities of keratinization
 Differential Diagnosis
Differential Diagnosis
- •
Folliculitis
- •
Darier’s disease
- •
Spongiotic dermatitis
- •
Benign familial pemphigus
- •
Galli-Galli disease
 Treatment
Treatment
First Line
- •
Control of fever, hospital discharge, and avoidance of sun and sweating
- •
Baths with emollient bath oils or colloidal oatmeal
- •
Often transient and resolves without treatment
Second Line
- •
Topical steroids
- •
Phototherapy
- •
Systemic corticosteroids
Third Line
- •
Isotretinoin or acitretin
- •
Dapsone
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Rituximab has produced clearing of TAD in patients being treated for lymphoma.
77
Hairy Tongue
 General Comments
General Comments
Definition
- •
Asymptomatic discoloration of tongue
Etiology
- •
Tobacco abuse, poor oral hygiene
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Chronic, asymptomatic discoloration of dorsal surface of tongue ( Fig. 3.158 )
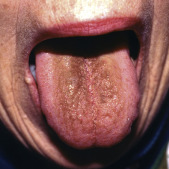
FIG. 3.158
Brownish-yellow, painless thickening on the dorsum of the tongue following a recent course of antibiotics.
(William Weston Collection)
Physical Examination
- •
Brown-blackish discoloration and elongation of papillae on tongue ( Fig. 3.159 )

FIG. 3.159
Severe black hairy tongue in a patient who was a heavy smoker.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
None
 Differential Diagnosis
Differential Diagnosis
- •
Oral hairy leukoplakia
- •
Candidiasis
- •
Lichen planus
- •
Stomatitis
 Treatment
Treatment
First Line
- •
Mechanical debridement of elongated papillae with toothbrush or tongue blade
- •
Removal of etiology (e.g., avoidance of tobacco products)
Second Line
- •
Mouthwashes
Third Line
- •
Electrodesiccation and curettage
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Improvement in mouth hygiene is essential to prevent recurrence.
78
Halo Nevi
 General Comments
General Comments
Definition
- •
Halo nevus, also known as Sutton nevus, perinevoid vitiligo, or leukoderma acquisitum centrifugum, is a pigmented nevus with a surrounding depigmented zone.
Etiology
- •
Immunologic destruction of melanocytes and nevus cells. Patients demonstrate antibodies to melanocytes and cell-mediated immunity to nevus cells. There may be associated vitiligo.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Most common in children (average age of onset is 15 years)
- •
Predilection of most lesions is the trunk, particularly the back
Physical Examination
- •
Centrally placed pigmented nevus is surrounded by a 1-mm to 5-mm halo of hypopigmentation or depigmentation ( Fig. 3.160 ).

FIG. 3.160
Close-up of a halo nevus demonstrating a reddish-brown, compound nevus surrounded by a halo of depigmentation.
(William Weston Collection)
Diagnostic Tests
- •
Biopsy: Histologically, halo nevi demonstrate a band of lymphocytes that extends throughout the lesion, intimately mingling with the melanocytes. There may be complete loss of melanocytes in the “haloed” area.
 Differential Diagnosis
Differential Diagnosis
- •
Benign melanocytic nevus
- •
Pseudomelanoma
- •
Atypical nevus
- •
Melanoma
 Treatment
Treatment
First Line
- •
Observation
Second Line
- •
Excision
 Clinical Pearl(s)
Clinical Pearl(s)
- •
In most patients, eventual repigmentation of the halo occurs over a period of months to years.
79
Hand-Foot-Mouth Disease
 General Comments
General Comments
Definition
- •
Hand-foot-and-mouth (HFM) disease is a viral illness that is characterized by superficial lesions of the oral mucosa and of the skin of the extremities.
Etiology
- •
Coxsackievirus Group A, Type 16, was the first and is the most common viral agent isolated.
- •
Enterovirus 71 is the second leading cause of HFMD.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
After a 4- to 6-day incubation period, patients may complain of odynophagia, sore throat, malaise, and fever (38.3–40° C).
- •
One to two days later the characteristic oral lesions appear.
- •
In 75% of cases, skin lesions on the extremities accompany these oral manifestations.
- •
Cutaneous symptoms are found in 11% of adults.
- •
Lesions appear over the course of 1 or 2 days.
- •
Involvement of the buttocks and perineum is present in 31% of cases.
- •
In rare cases, encephalitis, meningitis, myocarditis, poliomyelitislike paralysis, and pulmonary edema may develop. Sporadic acute paralysis has been reported with enterovirus 71.
- •
Although information is limited, there is no clear evidence that pregnancy outcomes are affected.
Physical Examination
- •
Oral lesions, usually between 5 and 10, are commonly found on the tongue, buccal mucosa, gingivae, and hard palate.
- •
Oral lesions initially start as 1- to 3-mm erythematous macules and evolve into gray vesicles on an erythematous base.
- •
Vesicles are often broken by the time of presentation and appear as superficial gray ulcers with surrounding erythema.
- •
Skin lesions of the hands ( Fig. 3.161 ) and feet ( Fig. 3.162 ) start as oval erythematous papules (3–10 mm in diameter) that evolve into gray vesicles that may be mildly painful. These vesicles are usually intact at presentation and remain so until they desquamate within 2 weeks.

FIG. 3.161
Painless, vesicular lesion on palmar surface of the index finger.
(William Weston Collection)

FIG. 3.162
Three vesicular lesion of HFM disease of the foot.
(William Weston Collection)
Diagnostic Tests
- •
No tests are indicated unless the diagnosis is in doubt.
- •
Throat culture or stool specimen may be obtained for viral testing, but results may take 2 to 4 weeks.
 Differential Diagnosis
Differential Diagnosis
- •
Aphthous stomatitis
- •
Herpes simplex infection
- •
Herpangina
- •
Behçet’s syndrome
- •
Erythema multiforme
- •
Pemphigus
- •
Gonorrhea
- •
Acute leukemia
- •
Lymphoma
- •
Allergic contact dermatitis
 Treatment
Treatment
First Line
- •
Palliative therapy is given for this usually self-limited disease.
Second Line
- •
Limited data suggest acyclovir may have a role in treatment of certain cases.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
HFM is transmitted primarily by the fecal-oral route and is highly contagious. Although children are predominantly affected, adults are also at risk. This disease is usually self-limited and benign.
- •
Frequent hand washing, disinfection of contaminated surfaces, and washing of soiled articles of clothing can help reduce transmission.
- •
HFM has no relationship to hoof-and-mouth disease in cattle.
- •
Onychomadesis (proximal nail shedding) may be seen weeks after the other cutaneous symptoms have resolved. It is harmless and self-limited.
80
Henoch-Schönlein Purpura
 General Comments
General Comments
Definition
- •
Henoch-Schönlein purpura (HSP) is a systemic, small-vessel, IgA immune complex–mediated leukocytoclastic vasculitis characterized by a triad of palpable purpura, abdominal pain, and arthritis. It may also present with gastrointestinal bleeding, arthralgias, and renal involvement.
Etiology
- •
Presumptive etiology is exposure to a trigger antigen that causes antibody formation.
- •
Antigen-antibody (immune) complex deposition then occurs in the arteriole and capillary walls of skin, renal mesangium, and GI tract. IgA deposition is most common.
- •
Antigen triggers postulated include drugs, foods, immunization, and upper respiratory and other viral illnesses. Group A streptococcal infection is the most common precipitant in children, seen in up to one third of cases.
- •
Serologic and pathologic evidence suggests an association between parvovirus B 19 and HSP, which may explain observed cases of HSP that do not respond to corticosteroids or other immunosuppressive therapy.
- •
Case reports describing development of HSP following treatment with immunosuppressive agents such as etanercept have been published.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Skin manifestations are most common.
- •
Palpable purpura ( Fig. 3.163 ) is seen in 70% of adult patients, whereas GI complaints are more common in children.

FIG. 3.163
Classic palpable purpura on the lower extremities of a child with Henoch-Schönlein purpura.
- •
Arthralgias and arthritis are seen in 80% of patients.
- •
GI symptoms are seen in approximately one third of patients. Common findings are nausea, vomiting, diarrhea, cramping, abdominal pain, hematochezia, and melena.
- •
Renal involvement is seen in up to 80% of older children, usually within the first month of illness. Less than 5% progress to end-stage renal failure, which is a major cause of morbidity.
Physical Examination
- •
Palpable purpura is seen in dependent areas, especially the lower extremities, and areas subjected to pressure such as the beltline.
- •
Subcutaneous edema is common.
Diagnostic Tests
- •
Diagnosis is clinical.
- •
Skin biopsy will show leukocytoclastic vasculitis.
- •
Direct immunofluorescent studies will demonstrate IgA ( Fig. 3.164 ) , C3, and fibrin in and around small blood vessels.
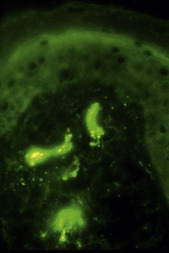
FIG. 3.164
Direct immunofluorescent study of lesional skin demonstrating marked granular deposition of IgA in three small blood vessels. Fibrin and C3 were also positive.
(Fitzsimons Army Medical Center Collection)
- •
Blood pressure and urinalysis should be obtained in all patients to assess for renal disease.
 Differential Diagnosis
Differential Diagnosis
- •
Polyarteritis nodosa
- •
Meningococcemia
- •
Thrombocytopenic purpura
- •
Hypersensitivity vasculitis
- •
Microscopic polyangiitis
 Treatment
Treatment
- •
Prednisone may be administered if there is renal or severe GI disease, although the benefits are not clear. Early treatment with prednisone reduces abdominal pain and joint symptoms but does not appear to prevent development of renal disease.
- •
Corticosteroids and azathioprine may be beneficial if rapidly progressive glomerulonephritis is present. Pulse methylprednisolone therapy has also been proposed in patients with glomerulonephritis, mesenteric vasculitis, or pulmonary involvement.
- •
NSAIDs may be used for arthritis and arthralgias.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Prognosis is excellent, with most patients experiencing spontaneous recovery within 4 weeks.
- •
End-stage renal disease occurs in 5% of patients. Chronic renal insufficiency is the most common long-term morbidity.
- •
GI complications include mesenteric infarction, perforation, and intussusception.
- •
Testicular torsion has also been reported.
- •
Recurrence is seen in up to one third of patients, especially within first 4 to 6 months after the initial episode, and most commonly in patients with renal involvement.
- •
Blood pressure should be monitored for several months after symptom resolution.
81
Herpes Simplex
 General Comments
General Comments
Definition
- •
Herpes simplex is a viral infection caused by the herpes simplex virus (HSV). HSV-1 is associated primarily with oral infections, whereas HSV-2 causes mainly genital infections; however, each type can infect any site.
Etiology
- •
HSV-1 and HSV-2 are both DNA viruses. Following the primary infection, the virus enters the nerve endings in the skin directly below the lesions and ascends to the dorsal root ganglia, where it remains in a latent stage until it is reactivated.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Primary infection:
- •
Symptoms occur from 3 to 7 days after contact (respiratory droplets, direct contact).
- •
Constitutional symptoms include low-grade fever, headache and myalgias, regional lymphadenopathy, and localized pain.
- •
Pain, burning, itching, and tingling last several hours.
- •
Grouped vesicles, usually with surrounding erythema, appear and generally ulcerate or crust within 48 hours ( Fig. 3.165 ).

FIG. 3.165
Primary HSV infection of both the upper and lower lips. In contrast to recurrent HSV that is usually very localized, primary infections usually involve a larger area and are more likely to demonstrate regional lymphadenopathy.
(John Aeling Collection)
- •
During the acute eruption the patient is uncomfortable; involvement of lips and inside of mouth may make it unpleasant for the patient to eat; urinary retention may complicate involvement of the genital area.
- •
Lesions generally last from 2 to 6 weeks and heal without scarring.
- •
- •
Recurrent infection:
- •
Recurrent infection is generally caused by alteration in the immune system; fatigue, stress, menses, local skin trauma, and exposure to sunlight are contributing factors.
- •
The prodromal symptoms (fatigue, burning, and tingling of the affected area) last 12 to 24 hours.
- •
A cluster of lesions generally evolve within 24 hours from a macule to a papule and then vesicles surrounded by erythema ( Fig. 3.166 ) ; the vesicles coalesce and subsequently rupture within 4 days, revealing erosions covered by crusts.

FIG. 3.166
Recurrent painful vesicular eruption on the upper lip (herpes labialis).
- •
The crusts are generally shed within 7 to 10 days, revealing a pink surface.
- •
Rapid onset of diffuse cutaneous herpes simplex (eczema herpeticum) may occur in certain atopic infants and adults. It is a medical emergency, especially in young infants, and should be promptly treated with acyclovir.
- •
Herpes encephalitis, meningitis, and ocular herpes can occur in patients with immunocompromised status and occasionally in normal hosts.
- •
Physical Examination
- •
The most common location of the lesions is on the vermilion border of the lips (HSV-1), the penile shaft or glans penis ( Fig. 3.167 ) and the labia (HSV-2), buttocks (seen more often in women), fingertips (herpetic whitlow) ( Fig. 3.168 ) , and trunk (may be confused with herpes zoster).

FIG. 3.167
Recurrent, painful, grouped vesicles on the penis.
(Fitzsimons Army Medical Center Collection)

FIG. 3.168
Herpetic whitlow. A cluster of painful, confluent vesicles on an erythematous base of the finger.
- •
The vesicles are uniform in size (differentiating it from herpes zoster vesicles, which vary in size).
Diagnostic Tests
- •
Direct immunofluorescent antibody slide tests will provide a rapid diagnosis. Rapid polymerase chain reaction (PCR) is the new gold standard for HSV. Positive results are reported as “HSV-type 1 DNA detected” or “HSV-type 2 DNA detected” or both. Results are generally available on same day with rapid test.
- •
Viral culture can also be used for diagnosis; results are generally available in 1 or 2 days; the lesions should be sampled during the vesicular or early ulcerative stage; cervical samples should be taken from the endocervix with a swab.
- •
Pap smear will detect HSV-infected cells in cervical tissue from women without symptoms.
 Differential Diagnosis
Differential Diagnosis
- •
Impetigo
- •
Behçet’s syndrome
- •
Coxsackievirus infection
- •
Syphilis
- •
Stevens-Johnson syndrome
- •
Herpangina
- •
Aphthous stomatitis
- •
Varicella
- •
Herpes zoster
 Treatment
Treatment
First Line
- •
Penciclovir 1% cream can be used for recurrent herpes labialis on the lips and face. It should be applied Q2H when awake for 4 days. Treatment should be started at the earliest sign or symptom. Its use decreases healing time of orolabial herpes by about 1 day. Topical acyclovir 5% cream can also be used for herpes labialis; when started at the prodrome or papule stage, it decreases the duration of an episode by about one-half day.
- •
Docosanol 10% cream, a long-chain saturated alcohol, inhibits fusion between the plasma membrane and the viral envelope, blocking viral entry and subsequent replication. It is available over the counter and, when applied at the first sign of recurrence of herpes labialis, may shorten the durations of the episode by about 12 hours.
- •
Valacyclovir 2 g PO Q12H for 1 day or famciclovir 500 mg, 3 tablets given at once, begun within the first symptoms of herpes labialis can modestly shorten its duration.
- •
Acyclovir ointment or cream applied using a finger cot or rubber glove Q3H to Q6H (6 times daily) for 7 days may be useful for the first clinical episode of genital herpes.
- •
Primary genital infections may be treated with oral acyclovir 200 mg 5 times daily for 7–10 days. Valacyclovir caplets can also be used for the initial episode of genital herpes (1 g BID for 7–10 days). Famciclovir 250 mg TID for 7–10 days is also effective. Intravenous acyclovir (5 mg/kg infused at a constant rate over 1 hr Q8H for 7 days in patients with normal renal function) may be used for severe cases.
- •
Application of topical cool compresses with Burow’s solution for 15 minutes 4 to 6 times daily may be soothing in patients with extensive erosions on the vulva and penis (decrease edema and inflammation, debridement of crusts and purulent material).
Second Line
- •
Recurrent episodes of genital herpes can be treated with acyclovir. A short course (800 mg TID for 2 days) is effective. Other treatment options include 800 mg PO BID for 3 to 5 days, generally started during the prodrome or within 2 days of onset of lesions; famciclovir is also useful for treatment of recurrent genital herpes (125 mg Q12H for 5 days in patients with normal renal function started at the first sign of symptoms), as is valacyclovir (500 mg Q12H for 3 days in patients with normal renal function).
- •
Patients with six recurrences of genital herpes a year can be treated with daily prophylactic valacyclovir 1 g QD, acyclovir 400 mg BID, or famciclovir 250 mg BID.
Third Line
- •
Acyclovir-resistant mucocutaneous lesions in patients with HIV can be treated with foscarnet (40–60 mg/kg IV Q8H in patients with normal renal function); HPMPC has also been reported to be effective in HSV infections resistant to acyclovir or foscarnet.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Condom use offers significant protection against HSV infection.
- •
Patients should also avoid contact with immunocompromised hosts or neonates when lesions are present.
82
Herpes Zoster (Shingles)
 General Comments
General Comments
Definition
- •
Herpes zoster is a disease caused by reactivation of the varicella zoster virus.
Etiology
- •
Reactivation of varicella-zoster virus (VZV, a human herpes virus 3) may occur several years after the primary infection (chickenpox); the virus becomes latent in the dorsal root ganglia and reemerges when there is a weakening of the immune system (secondary to disease or advanced age).
- •
Herpes zoster occurs in 10% to 20% of the population.
- •
There is an increased incidence in immunocompromised patients (AIDS, malignancy), the elderly, and children who acquired chickenpox when younger than 2 months.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Pain generally precedes skin manifestation by 3 to 5 days and is generally localized to the dermatome that will be affected by the skin lesions.
- •
Constitutional symptoms are often present (malaise, fever, headache).
- •
Pain during and after the rash is often significant.
- •
Secondary bacterial infection with S. aureus or Streptococcus pyogenes may occur.
- •
Regional lymphadenopathy may occur.
- •
Herpes zoster may involve the trigeminal nerve (the most common cranial nerve involved). Involvement of the geniculate ganglion can cause facial palsy and a painful ear, with the presence of vesicles on the pinna and external auditory canal (Ramsay Hunt syndrome).
Physical Examination
- •
The initial rash consists of erythematous maculopapules ( Fig. 3.169 ) , generally affecting one dermatome (thoracic region in majority of cases); some patients may have scattered vesicles outside the affected dermatome.

FIG. 3.169
Following a prodrome of burning of the leg, this patient experienced an outbreak of herpes zoster in a dermatomal distribution. These are early lesions that are not yet vesicular.
(John Aeling Collection)
- •
The initial maculopapules evolve into vesicles and pustules by the third or the fourth day ( Fig. 3.170 ).

FIG. 3.170
Crusted, weeping vesicles and pustule of the breast in developed lesions of herpes zoster.
(Fitzsimons Army Medical Center Collection)
- •
The vesicles have an erythematous base, are cloudy, and have various sizes (a distinguishing characteristic from herpes simplex, in which the vesicles are of uniform size).
- •
The vesicles subsequently become umbilicated and then form crusts ( Fig. 3.171 ) that generally fall off within 3 weeks; scarring may occur.

FIG. 3.171
Resolving herpes zoster involving the ophthalmic division of the facial nerve with residual crusting.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
Tzanck smear ( Fig. 3.172 )
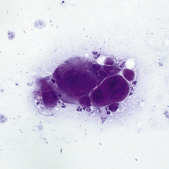
FIG. 3.172
Tzanck preparation demonstrating multinucleated, acantholytic cells in herpes zoster. Although Tzanck preparations are useful in trained health care providers, it does not differentiate between varicella and HSV infections.
(Fitzsimons Army Medical Center Collection)
- •
Viral culture
- •
Serology
 Differential Diagnosis
Differential Diagnosis
- •
Herpes simplex
- •
Contact dermatitis
- •
Varicella
- •
Cellulitis
- •
Impetigo
- •
Pemphigus
 Treatment
Treatment
First Line
- •
Oral antiviral agents can decrease acute pain, inflammation, and vesicle formation when treatment is begun within 48 hr of onset of rash. Treatment options are:
- •
Valacyclovir 1000 mg tid for 7 days
- •
Famciclovir 500 mg tid for 7 days
- •
Acyclovir 800 mg 5 times daily for 7 to 10 days
- •
- •
Wet compresses (using Burrow’s solution or cool tap water) applied for 15 to 30 minutes, 5 to 10 times a day, are useful to break vesicles and remove serum and crust.
- •
Care must be taken to prevent any secondary bacterial infection.
Second Line
- •
If there are no contraindications, corticosteroids should be considered in older patients within 72 hours of clinical presentation or if new lesions are still appearing. Initial dose is prednisone 40 mg/day, decreased by 5 mg/day until finished. When used, there is a decrease in the use of analgesics and time to resumption of usual activities, but there is no effect on the incidence and duration of postherpetic neuralgia.
- •
Immunocompromised patients should be treated with intravenous acyclovir 10 mg/kg Q8H in 1-hour infusions for 7 days, with close monitoring of renal function and adequate hydration; vidarabine (continuous 12-hour infusion of 10 mg/kg/day for 7 days) is also effective for treatment of disseminated herpes zoster in immunocompromised hosts.
- •
Gabapentin 300 to 600 mg QD or pregabalin 75 mg BID are effective in the treatment of pain and sleep interference associated with postherpetic neuralgia.
- •
Lidocaine patch 5% is also effective in relieving postherpetic neuralgia. Patches are applied to intact skin to cover the most painful area for up to 12 hours within a 24-hour period.
- •
Capsaicin cream can be useful for treatment of postherpetic neuralgia. It is generally applied three to five times daily for several weeks after the crusts have fallen off.
Third Line
- •
Patients with AIDS and transplant patients may develop acyclovir-resistant varicella zoster; these patients can be treated with foscarnet (40 mg/kg IV Q8H) continued for at least 10 days or until lesions are completely healed.
- •
Sympathetic blocks (stellate ganglion or epidural) with 0.25% bupivacaine and rhizotomy are reserved for severe cases of postherpetic neuralgia unresponsive to conservative treatment.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
The incidence of postherpetic neuralgia (defined as pain that persists more than 3 months after the rash has healed) increases with age (30% by age 40 years; >70% by age 70 years); antivirals reduce the risk of postherpetic neuralgia.
- •
Incidence of disseminated herpes zoster is increased in immunocompromised hosts (e.g., 15%–50% of patients with active Hodgkin’s disease).
- •
Immunocompromised hosts are also more prone to neurologic complications (encephalitis, myelitis, cranial and peripheral nerve palsies, acute retinal necrosis). The mortality rate is 10% to 20% in immunocompromised hosts with disseminated zoster.
- •
Motor neuropathies occur in 5% of all cases of zoster; complete recovery occurs in more than 70% of patients.
- •
A live attenuated vaccine (“Zostavax”) aimed at boosting immunity to VZV, reducing the risk of herpes zoster, and decreasing the incidence of post-herpetic neuralgia is recommended for adults older than 60 years.
83
Hidradenitis Suppurativa
 General Comments
General Comments
Definition
- •
Hidradenitis suppurativa (HS) is a chronic, relapsing condition that occurs within the terminal follicular epithelium of the apocrine glands (axilla, inguinal folds, perineum, genitalia, and periareolar region) in which keratinous materials occlude the follicles, causing secondary inflammation of the apocrine glands, resulting in chronic infection and draining abscess that lead to scarring.
Etiology
- •
Keratinous materials plug apocrine glands in hair follicles, leading to stasis, dilation, rupture, and reepithelialization.
- •
Bacteria are trapped and multiply, leading to gland rupture with surrounding inflammation and local bacterial infection.
- •
Over time, repeated nodules and infections cause scarring that can lead to deep tissue damage and sinus tracts.
- •
Infectious agents such as Streptococcus, Staphylococcus, and Escherichia coli, and enteric flora have been identified in cultures but are likely a secondary component of the disease.
- •
There is likely a significant genetic component to the disease. Thirty-five percent to 40% of patients report a family history of HS. An HS spectrum of different phenotypes has been characterized involving genetic factors that are not yet well described but may be important for future therapy.
- •
HS has been associated with other endocrine and autoimmune disorders such as diabetes, Cushing’s disease, acromegaly, Crohn’s disease, and inflammatory arthritis.
- •
Metabolic syndrome affects as many as 50% of patients with HS and may exacerbate the associated inflammation.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
The diagnosis is primarily clinical, based on the development of typical lesions in a characteristic distribution, with a relapsing nature. The course of HS is prolonged and marked by intermittent periods of activity and remission.
- •
Early symptoms include pain, itching, burning, erythema, and hyperhidrosis.
- •
Typical lesions include:
- •
Painful erythematous papules and nodules leading to painful abscesses with foul-smelling discharge
- •
Dermal contractures and ropelike elevation of the skin
- •
Comedones in the apocrine, gland-bearing skin
- •
- •
The axilla is the most commonly involved site. Less common sites include the inguinal region, the breasts, and the perineal or perianal skin.
- •
There is a strong tendency toward relapse and recurrence.
- •
There is often a poor response to conventional antibiotics and bacterial pathogens are only variably isolated from cultures of lesions.
- •
The disease is often mistaken for a simple infection, and a long delay in diagnosis is common.
- •
Three clinical subtypes of HS have been recently proposed 1
1 Woodruff CM, Charlie AM, Leslie KS: Hidradenitis suppurative: a guide for the practicing physician, Mayo Clin Proc 90(12):1679–1693, 2015.
:
- •
A classic axillary-mammary HS subtype, representing 48% of cases and characterized by breast and axillary involvement and hypertrophic scarring
- •
A follicular HS subtype, representing 26% of cases manifesting primarily in male smokers with a family history of HS and characterized by follicular lesions, including epidermal cysts, pilonidal sinus, comedones, and severe acne
- •
A gluteal HS subtype, representing 26% of cases, most often seen in smokers with lower body mass index (BMI) and with a morphology characterized by follicular papules, folliculitis, and gluteal involvement
- •
Physical Examination
- •
Initial lesions have the appearance of boils in early adolescence.
- •
Skin lesions and abscesses tend to be bilateral. Multifocal involvement, bridged scarring, and sinus formation may be present ( Fig. 3.173 ). Double comedones are frequently present.

FIG. 3.173
Hidradenitis suppurativa. Painful, tender red abscesses and nodules in the axilla, the most common location for this disorder.
(Fitzsimons Army Medical Center Collection)
Diagnostic Tests
- •
The diagnosis is primarily clinical based on the development of typical lesions.
- •
Any purulent discharge should be sampled for bacterial culture and sensitivity.
 Differential Diagnosis
Differential Diagnosis
- •
Folliculitis and other follicular pyoderma furuncles, pilonidal cysts
- •
Granuloma inguinale
- •
Crohn’s disease (perianal and vulvular manifestations)
- •
Bartholin’s cyst infection
- •
Actinomycosis
- •
Lymphogranuloma venereum
- •
Furuncle
- •
Lymphangitis
- •
Cat-scratch disease
- •
Tularemia
- •
Erysipelas
- •
Ulcerative colitis
 Treatment
Treatment
First Line
- •
Systemic antibiotics have not proven to be effective; however, they are the mainstay of treatment. Their antiinflammatory properties may be helpful.
- •
Clindamycin is the only topical antibiotic proven to be effective in a randomized controlled trial and is appropriate for stage I disease.
- •
For oral therapy in stage II: consider clindamycin and rifampin in combination. Cephalosporins, dicloxacillin, erythromycin, minocycline, and tetracycline have also been used.
- •
Severe, recurrent disease can require up to 3 to 6 months of antibiotics.
Second Line
- •
Use NSAIDs for inflammation and pain. Consider gabapentin, pregabalin, or SSRIs for chronic pain management.
- •
Oral contraceptives with low androgenic progesterone (norgestimate, desogestrel, or gestodene) for women show mixed effectiveness. They are especially advantageous for female patients of childbearing age who also require some form of birth control.
- •
Isotretinoin has been used with mixed effectiveness.
Third Line
- •
Intralesional corticosteroids
- •
Metformin has mixed effectiveness, possibly due to related metabolic syndrome and hyperandrogenism.
- •
Trials using zinc gluconate 75 to 118 mg/day in patients with mild (grade 1) disease have shown mixed effectiveness.
- •
Corticosteroids and other immune suppressants such as cyclosporin, infliximab, and etanercept have been used for stage II disease with mixed results.
- •
Adalimumab, an antitumor necrosis factor-α antibody given once per week (dose 40 mg/week), has shown significantly higher clinical response as compared to placebo in phase 3 trials. Infliximab has also been used in trials with variable success rates, with most patients exhibiting clinical improvement within 8 weeks.
 Clinical Pearl(s)
Clinical Pearl(s)
- •
Incision and drainage of nonpurulent lesions is not recommended due to recurrence and scarring.
84
Histoplasmosis
 General Comments
General Comments
Definition
- •
Histoplasmosis is caused by the fungus Histoplasma capsulatum and characterized by a primary pulmonary focus with occasional progression to chronic pulmonary histoplasmosis (CPH) or various forms of dissemination.
Etiology
- •
H. capsulatum is a dimorphic fungus present in temperate zones and river valleys worldwide.
- •
In the United States, it is highly endemic in southeastern, mid-Atlantic, and central states.
- •
H. capsulatum exists as mold at ambient temperature and favors soils enriched with bird or bat droppings.
 Keys to Diagnosis
Keys to Diagnosis
Clinical Manifestation(s)
- •
Conidia are deposited in alveoli, then converted to yeast forms; they spread to regional lymph nodes and other organs, especially the liver and spleen.
- •
One to two weeks later, a granulomatous inflammatory response begins to contain the yeast in the form of discrete granulomas.
- •
Delayed-type hypersensitivity to Histoplasma antigens occurs 3 to 6 weeks after exposure.
- •
Clinical disease manifests in various forms, depending on host cellular immunity and inoculum size.
Physical Examination
- •
Cutaneous lesions are typically multiple small nodules, which may ulcerate.
- •
Oral lesions presenting as erosions and ulcerations are a frequent finding ( Fig. 3.174 ).