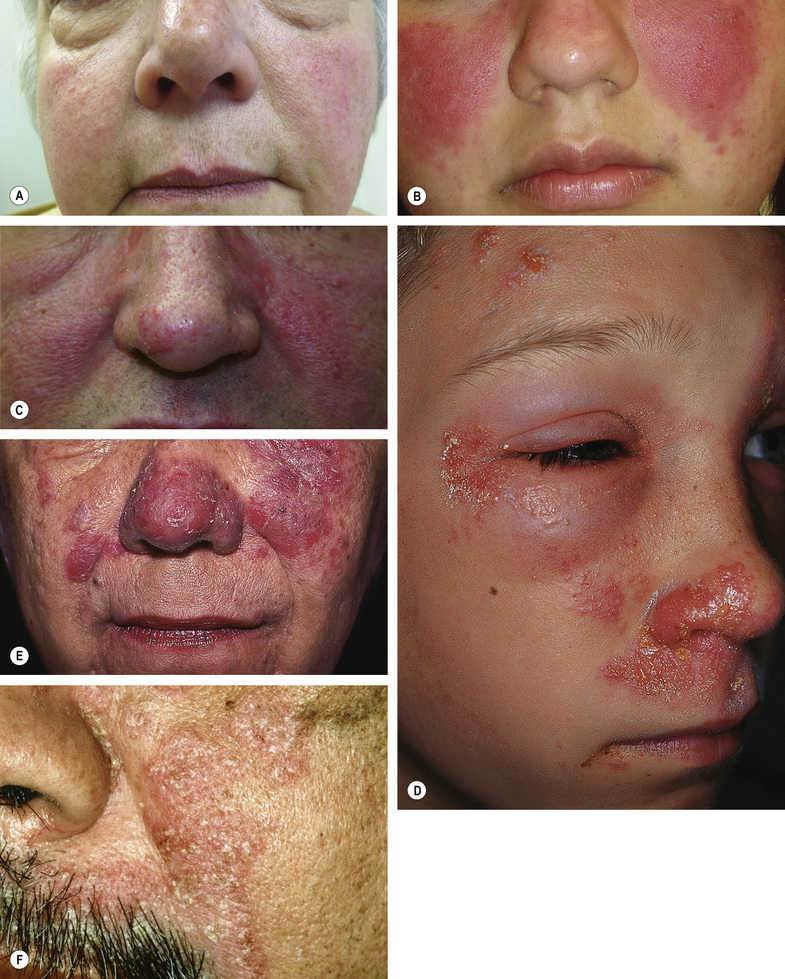
• Angiofibromas of tuberous sclerosis – firm papules clustered near nose/nasolabial folds
• Trichoepitheliomas and/or cylindromas – nose/nasolabial folds or other parts of face, other stigmata of tuberous sclerosis absent
Fig. 2.2Multiple papules, red–pink to brown. A Acne vulgaris. B Acne rosacea. C Granulomatous rosacea. D Angiofibromas of tuberous sclerosis. E Multiple familial trichoepitheliomas. F Multiple cylindromas.A, Courtesy, Andrea L Zaenglein, MD and Diane Thiboutot, MD; B,C, Courtesy, Yale Dermatology Residents’ Slide Collection; D, Courtesy, Brian Shuch, MD. A,C, From Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology, 3e. London: Saunders, 2012, with permission.
• Acne vulgaris – presence of open and closed comedones
• Steroid-induced rosacea – erythematous papules and papulopustules, absent comedones
• Periorificial dermatitis – monomorphous papules, confluent around the mouth
• Keratosis pilaris rubra – “grain-like” follicular papules on a background of erythema
• Trichostasis spinulosa – often on the nose, follicular orifices contain vellus hairs and keratinous debris that can be extruded with pressure
• Pseudofolliculitis barbae – follicular-based papules over the beard area
Fig. 2.3Acneiform lesions. A Comedonal acne vulgaris. B Steroid rosacea. C Periorificial dermatitis. D Keratosis pilaris rubra. E Trichostasis spinulosa. F Pseudofolliculitis barbae.A, Courtesy, Andrea L Zaenglein, MD and Diane Thiboutot, MD; B, Courtesy, Kalman Watsky, MD; C, Courtesy, Yale Dermatology Residents’ Slide Collection; D, Courtesy, Julie V Schaffer, MD; E, Courtesy, Judit Stenn, MD; F, Courtesy, A Paul Kelly, MD. A,B,D–F, From Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology, 3e. London: Saunders, 2012, with permission.
Pustules
Pustules (see Chapter 7) may be sterile or due to an infectious agent, in which case culture studies and/or biopsy may be necessary for a definitive diagnosis.
• Fungal or bacterial infection – erythematous plaque studded with pustules
• Herpes virus infection – clustered vesicles and/or pustules, base may be erythematous
Fig. 2.4Pustules. A Acne vulgaris. B Acne rosacea. C Fungal infection. D Staphylococcal folliculitis. E Herpes simplex virus infection.A,C, Courtesy, Kalman Watsky, MD; B, Courtesy Uwe Wollina, MD; D, Courtesy, Yale Dermatology Residents’ Slide Collection; E, Courtesy, Dirk Elston, MD. A,C,D, From Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology, 3e. London: Saunders, 2012, with permission. B, From Wollina U. Rosacea and rhinophyma in the elderly. Clin Dermatol. 2011;29:61–8. E, From Elston D. Clinical image collection. Dermatopathology, 2e. London: Saunders, 2014.
• Rosacea – overlaps with dermatoheliosis in later stages
• Dermatoheliosis – telangiectasias and erythema over facial prominences
Fig. 2.5Telangiectasia. A CREST syndrome. B Hereditary hemorrhagic telangiectasia (Osler–Weber–Rendu disease). C Erythematotelangiectatic rosacea. D Dermatoheliosis.A, Courtesy, M Kari Connolly, MD; B, Courtesy, Yale Dermatology Residents’ Slide Collection; C, From Two AM, Wu W, Gallo RL. Hata TR Rosacea : Part I. Introduction, categorization, histology, pathogenesis, and risk factors. J Am Acad Dermatol 2015; 72: 749–758, with permission. A, From Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology, 3e. London: Saunders, 2012, with permission.
• Rosacea – erythema is often fixed, telangiectasias in more advanced disease
• Acute lupus erythematosus – sparing of nasolabial folds, small erosions, scale may be present
• Dermatomyositis – involvement of eyelids and nasolabial folds
• Allergic contact dermatitis – edema and weeping lesions
• Pemphigus erythematosus – plaques with scale-crust and obvious erosions
• Seborrheic dermatitis – greasy scale, often accentuated in nasolabial folds
Fig. 2.6Malar erythema. A Erythematotelangiectatic rosacea, early. B Lupus erythematosus, malar rash. C Dermatomyositis. D Allergic contact dermatitis, acute, secondary to poison ivy. E Pemphigus erythematosus. F Seborrheic dermatitis.B,C, Courtesy, Yale Dermatology Residents’ Slide Collection; D, Courtesy, Jean L Bolognia, MD; E, Courtesy, Ronald P Rapini, MD; F, Courtesy, Dirk Elston, MD. D,E, From Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology, 3e. London: Saunders, 2012, with permission. F, From Elston D. Clinical image collection. Dermatopathology, 2e. London: Saunders, 2014.
Juicy Papules/Plaques/Nodules
The infiltrate may be lymphocytic, mixed, neutrophilic, or granulomatous.
• Folliculotropic mycosis fungoides – infiltrated plaque with loss of eyebrow hair
• B-cell lymphoma – pink–red to purple papulonodules
• Lupus tumidus – pink–violet plaques
• Lymphocytic infiltrate of Jessner – often annular, absent scale
• Polymorphous light eruption – edematous pink lesions, occur minutes to hours after sun exposure in spring and early summer
Mixed
• Granuloma faciale – red–brown plaque with prominent follicular orifices
Neutrophilic
• Sweet’s syndrome – crusted bright red papulonodules
Granulomatous
• Sarcoidosis – often affects the nose, infiltrated violaceous to red–brown plaque
Fig. 2.7Juicy papules/plaques/nodules. A Folliculotropic mycosis fungoides. B Lupus tumidus. C Lymphocytic infiltrate of Jessner. D Polymorphous light eruption. E Granuloma faciale. F Sweet’s syndrome. G Sarcoidosis (lupus pernio).A, Courtesy, Rein Willemze, MD; B, Courtesy, Julie V Schaffer, MD; C, E, G, Courtesy, Yale Dermatology Residents’ Slide Collection; D, NYU Slide Collection; F, Courtesy, Kalman Watsky, MD. A–G, From Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology, 3e. London: Saunders, 2012, with permission.
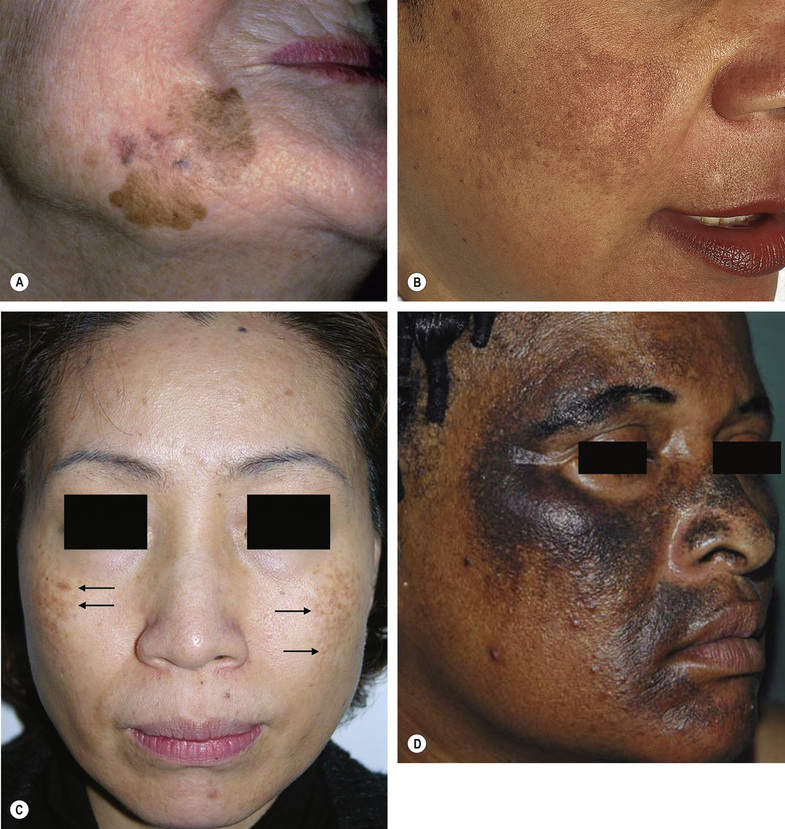
Flat Brown Patch
May be secondary to increased melanocytes, increased melanin, and/or dermal pigment.
• Lentigo maligna (melanoma in situ) – irregular with color variation
• Melasma – evenly light brown with an irregular border
• Hori nevus – light brown to blue–gray macules clustering into patches, on cheeks, typically in Asian women
• Ochronosis – brown to black patches secondary to topical hydroquinone
Fig. 2.8Flat brown patch. A Lentigo maligna. B Melasma. C Hori nevus. D Ochronosis.A, Courtesy, Yale Dermatology Residents’ Slide Collection. B, Courtesy, NYU Slide Collection. D, Courtesy, Regional Dermatology Training Centre, Moshi, Tanzania. A,B, From Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology, 3e. London: Saunders, 2012, with permission. C From, Park JM, Tsao H, Tsao S. Acquired bilateral nevus of Ota-like macules (Hori nevus). J Am Acad Dermatol. 2009;61:88–93. D, From Bolognia JL, Schaffer JV, Duncan KO, Ko CJ. Dermatology Essentials, 1e. Philadelphia: Saunders, 2014, with permission.
Only gold members can continue reading. Log In or Register to continue